
Abstract
Background:
Enhanced recovery program for pancreaticoduodenectomy have become standard care. Little is known about adherence rates and sustainability of the program, especially when pancreaticogastrostomy is used in reconstruction. The aim of this study was, therefore, to evaluate adherence rates and continued outcome, after implementation of an enhanced recovery program.
Methods:
Consecutive patients undergoing pancreaticoduodenectomy at the Department of Surgery, Skåne University Hospital, Lund, Sweden were followed, after implementation of enhanced recovery program, October 2012. In April 2015, some items in the enhanced recovery program were modified, namely earlier removal of nasogastric tubes and abdominal drain. The patients were analyzed in three groups, the implementation group (control) and two post-implementation groups; intermediate and modified group. Sustainability was assessed according to length of stay and adherence rate.
Results:
In total, 160 patients were identified. The overall protocol adherence rate increased from 65% to 72%, p = 0.035. While the pre- and intraoperative protocol items were fulfilled to more than >90%, the postoperative were lower, but increasing over time; 48%, 50%, and 58%, p = 0.033. Postoperative complications and hospital length of stay did not change significantly.
Conclusion:
The positive outcome of an enhanced recovery program for pancreaticoduodenectomy was reasonably well sustained. Compliance with the protocol has increased, but strict adherence remains a challenge, especially with the postoperative items.
Introduction
Enhanced recovery after surgery (ERAS®), or a fast track program, has become standard care in several surgical areas. These programs aim to reduce stress response to surgery in order to accelerate recovery and reduce morbidity. Most experiences originate from colorectal surgery. In recent years, several studies have reported its feasibility in pancreatic surgery settings. A fast track program after pancreaticoduodenectomy (PD) can reduce delayed gastric emptying (DGE) (1, 2) and postoperative length of stay (3–8), without compromising safety or health-related quality of life (8). These programs are also safe for elderly patients (9, 10) and when pancreaticogastrostomy is used in reconstruction (8, 11). Reports on adherence to different items in the programs have been scarce (9, 10, 12) and only two identified studies analyze adherence to preoperative, perioperative, and postoperative elements more thoroughly (2, 6), with somewhat contrary results. However, both reports suggest that low adherence may be associated with postoperative complications.
Reports from colorectal surgery point to an association between adherence to an enhanced recovery protocol with improved clinical outcomes (13). There are also some data indicating a decrease in compliance after the first period of implementation (14, 15). To our knowledge, there are no reports evaluating the sustainability of enhanced recovery protocols in pancreatic surgery over time. The aim of this study was, therefore, to assess whether the achieved benefits of the enhanced recovery program (ERP) were sustained after the implementation phase and to evaluate adherence rates to the protocol items.
Methods
Patients
This study followed consecutive patients undergoing PD at the Department of Surgery, Skåne University Hospital, Lund, Sweden, after October 2012. Patients treated when the ERP was implemented (control group, CG) were compared with the subsequent patients following the same ERP (intermediate group, IG) and patients following a modified protocol for ERP (modified group, MG). The time span for each group was 15 months, with the CG monitored from October 2012 to January 2014, the IG from January 2014 to April 2015, and the MG from April 2015 to August 2016. Information on the CG was collected from a prospectively designed database, and for the two other groups, data were retrospectively collected from medical records. All patients planned for PD at this institution follow ERP care. Patients with both malignant and benign diseases were included, with no exclusions. The study was approved by the Human Ethics Committee at Lund University (2015/833).
PD was performed using a standard technique including resection of the pyloric region, after access through a bilateral subcostal incision. Reconstruction was made by pancreaticogastrostomy with a retrocolic hepaticojejunostomy and gastrojejunostomy performed on the same loop. A nasogastric tube and one intra-abdominal drain were inserted.
Enhanced Recovery Program
Details of the different elements in the ERP (when implemented called “fast track program”) and the postoperative course for the first 50 patients have been presented previously (8). The program corresponds well with the guidelines for perioperative care for PD from the ERAS® Society (16). In summary, the protocol standardizes care for the patients in preoperative (preoperative counseling, carbohydrate loading, and antithrombotic prophylaxis), intraoperative (secondary dose antimicrobial prophylaxis, use of epidural analgesia, restrictive intravenous fluids, and antiemetic cocktail at the end of surgery), and postoperative elements (criteria for removal of nasogastric tube, abdominal drain, epidural analgesia and urinary catheter, and reintroduction of food and standardized mobilization). Discharge was planned within postoperative day (POD) 10 if the following discharge criteria were fulfilled: absence of fever, no need for intravenous fluid, adequate pain control with oral analgesia, passage of first stool/flatus, full mobilization, and patient agreement to discharge. In April 2015, two parameters were revised. Removal of the nasogastric tube was scheduled for POD 1, regardless of drainage volume. In the initial protocol, removal was accepted from POD 1 if the drained volume fell below 300 mL, but at the latest on POD 3. In the modified protocol, removal of the abdominal drain was accepted from POD 3 if the amylase level was below 480 U/L and drain output was less than 400 mL/day, instead of only 200 mL.
Overall adherence to the ERP protocol and individual item adherence was analyzed and compared between the three groups. The different items were also categorized and analyzed as preoperative, intraoperative, and postoperative care elements. Sustainability was assessed according to length of stay (LOS) and adherence rate.
Definitions
Complications were graded according to the Clavien–Dindo system (17) and comprehensive complication index (CCI) (18, 19), at 30 days after surgery or within the primary admission. CCI was calculated with the open access calculator (20). Clavien–Dindo ≥3a was considered to be major complications. A corresponding recognized cut-off within the CCI scoring system does not exist. In this study, a score of ≥26 was chosen, since 26.2 is the equivalent CCI score for Clavien–Dindo 3a. Procedure-specific complications, such as postoperative pancreatic fistula (POPF), postpancreatectomy hemorrhage (PPH), and DGE, were graded according to international standards and assessed 90 days after surgery (21–23). Mortality was registered within 90 days of surgery. LOS was counted from the day of surgery (POD 0) to discharge. Readmission within 90 days related to the PD was noted. The pancreatic fistula risk score described by Roberts was calculated from body mass index (BMI) and pancreatic duct width (24, 25).
Statistics
Descriptive statistics for categorical variables were presented as numbers and percentages and median and range for continuous variables. Differences between groups were evaluated with chi-square test for categorical variables and Kruskal–Wallis test for continuous variables. Adherence rate was presented as mean and compared with analysis of variance (ANOVA). A p-value of ≤0.05 was considered significant. Statistical analysis was conducted using SPSS® version 23.0 (SPSS Inc®, Chicago, IL, USA).
Results
From October 2012 to August 2016, 160 patients had a PD at Skåne University Hospital at Lund. The first 105 were treated according to the initial ERP, of which the first 50 was labeled the “control group” and the next 55 were the “intermediate group.” After modification of the protocol, 55 patients were treated in the “modified group.” The three groups demonstrated comparable patient demographics, median age (66–69, p = 0.116), BMI (24.48–25.64, p = 0.421) and pancreatic fistula predictive score (10–11, p = 0.982), except for a lower frequency of smokers in the CG (24% vs 45%–49%, p = 0.017) compared with IG and MG. The distribution of histopathology was unaltered between the groups, with a majority of periampullary adenocarcinoma (74%–78%), followed by benign/premalignant lesion (including cystic lesions; 15%–20%) and neuroendocrine tumors (4%–5%), p = 0.914. Tumor size was equal (median = 3.0 cm; p = 0.647) in the different groups. Operative time (424–474 min, p = 0.058) and blood loss (350–500 mL, p = 0.073) did not change. There was an increase in vascular resections, one in the CG, five in the IG, and 10 in the MG, p = 0.021.
Table 1 shows parameters of the postoperative care and complications. The nasogastric tube and abdominal drain were removed earlier in the MG, and patients subsequently reached the goal of free fluids earlier, which reflects the changes in the protocol.
Comparison of postoperative parameters and complications for the three groups.
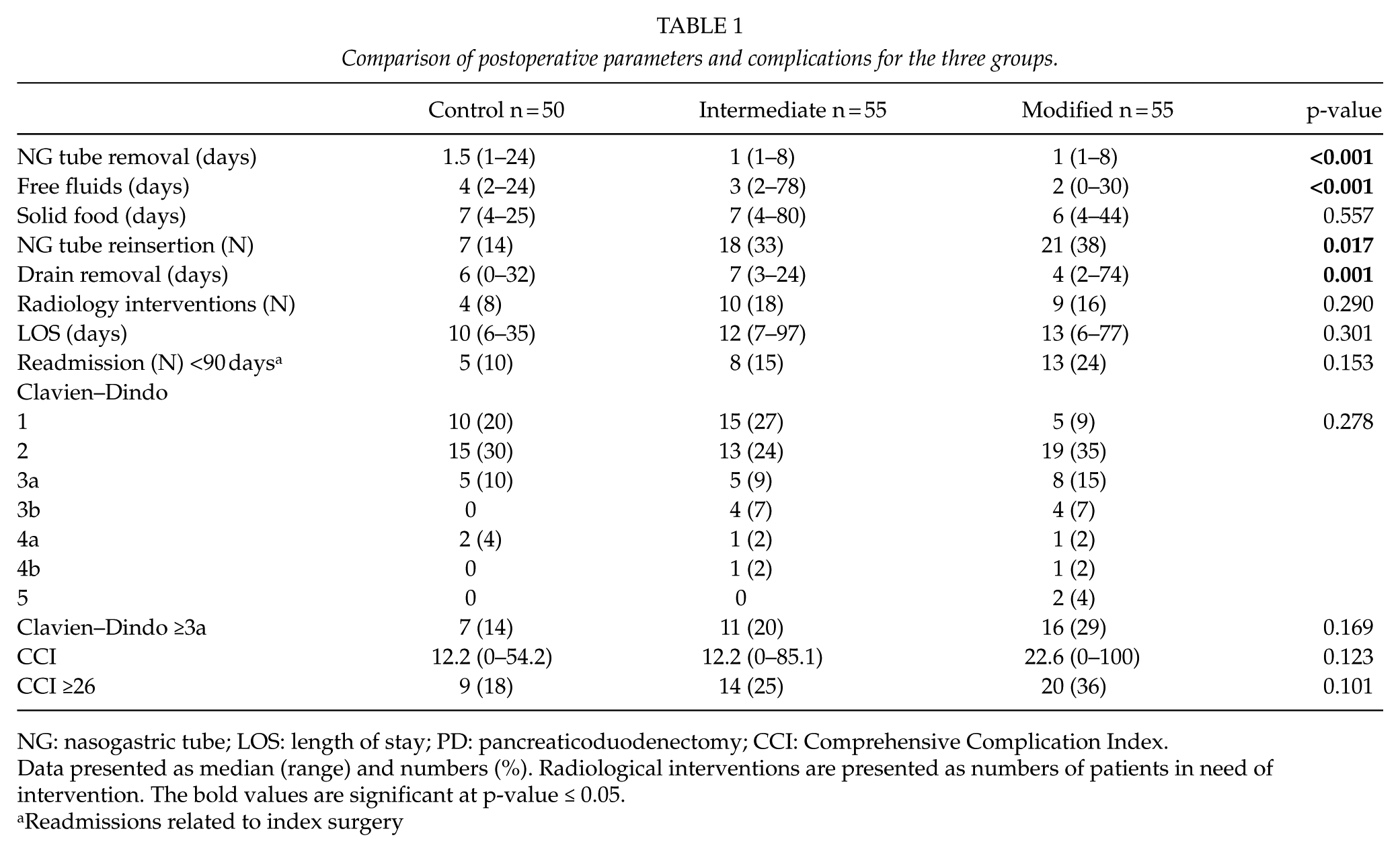
NG: nasogastric tube; LOS: length of stay; PD: pancreaticoduodenectomy; CCI: Comprehensive Complication Index.
Data presented as median (range) and numbers (%). Radiological interventions are presented as numbers of patients in need of intervention.
The bold values are significant at p-value ≤ 0.05.
Readmissions related to index surgery
Postoperative complications, both general and specific to pancreatic surgery, were essentially unaltered. The number of PPH (3/50, 8/55, 6/55, p = 0.409), POPF (12/50, 9/55, 16/55, p = 0.319), and DGE (13/50, 27/55, 27/55, p = 0.157) did not change significantly in the three groups. In total, there were five reoperations in the three groups, one in IG and four in MG. The indication for reoperation were, for the IG, PPH grade C (n = 1) and for the MG, bowel ischemia (n = 1), wound dehiscence (n = 1), and PPH grade C (n = 2). There were two mortalities in MG, caused by multi-organ failure due to sepsis, ischemic bowel due to a postoperative occlusion of the superior mesenteric artery, and none in the other two groups.
Adherence to the Protocol
Overall protocol adherence rate increased over time, from 65% in the CG to 68% in the IG and 72% in the MG, p = 0.035. The parameters were merged into preoperative, intraoperative, and postoperative parameters, showing that the preoperative and intraoperative parameters were fulfilled to more than 90% in all groups, with no statistical difference over time. The postoperative parameters were fulfilled to a lower proportion, but increasing over time, reaching 48%, 50%, and 58%, p = 0.033, in the groups, respectively. Adherence rates are outlined in Fig. 1. Analysis of each parameter in the postoperative course revealed that the only two parameters that changed significantly were removal of the abdominal drain and tolerance for solid food on POD 4, as depicted in Table 2. Patients with high adherence to the protocol had fewer complications and were more likely to be discharged by POD 10. Those with adherence of ≥90% (n = 13), had a median discharge on POD 8 (7–9) and no patient with Clavien–Dindo ≥3a. Groups with lower adherence had longer median stay and higher proportion of Clavien–Dindo ≥3a, increasing with falling adherence (Table 3).
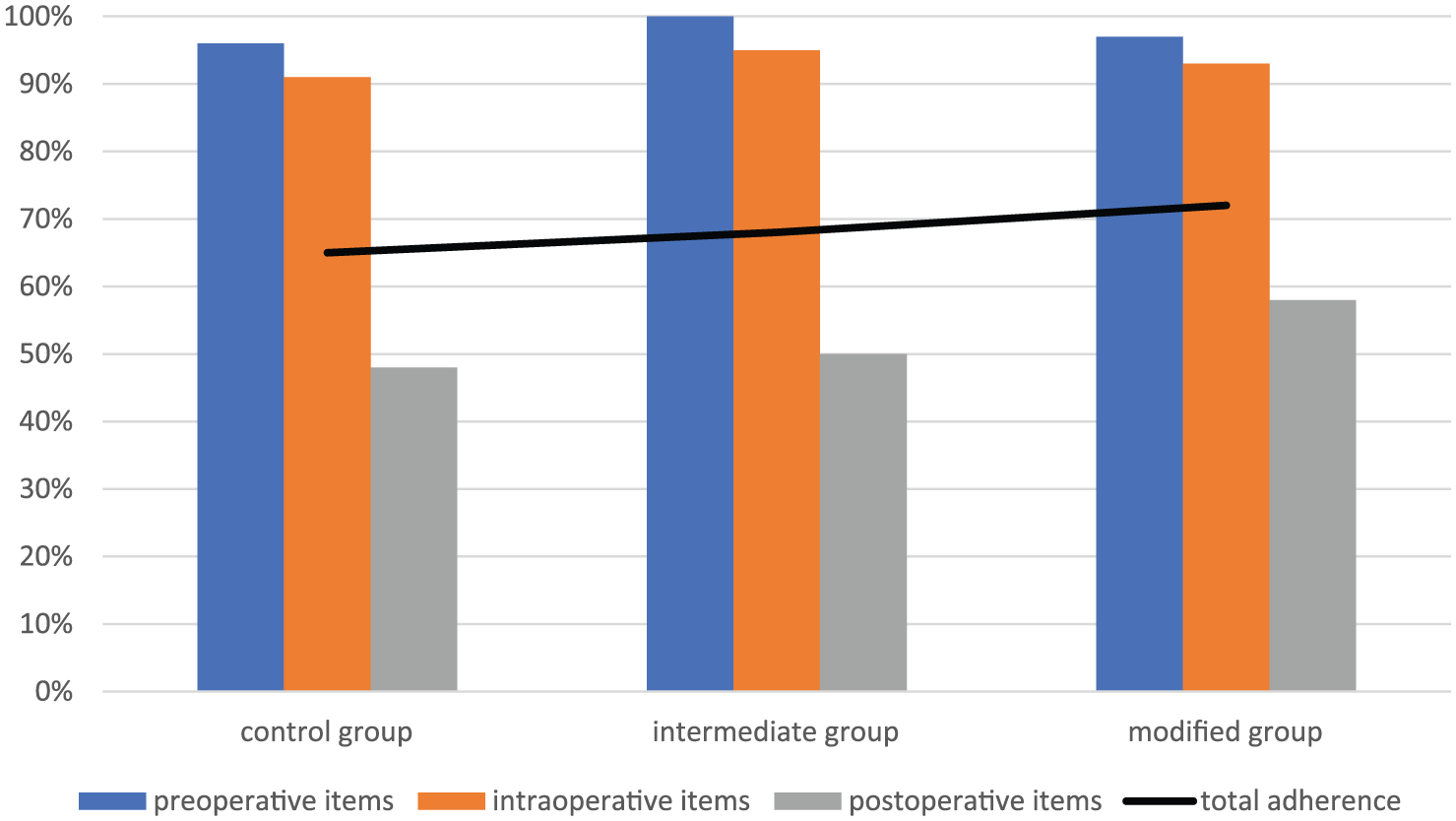
Adherence to preoperative, intraoperative, and postoperative items in the enhanced recovery protocol, as well as total adherence, for the three groups.
Adherence to individual postoperative parameters for the three groups.
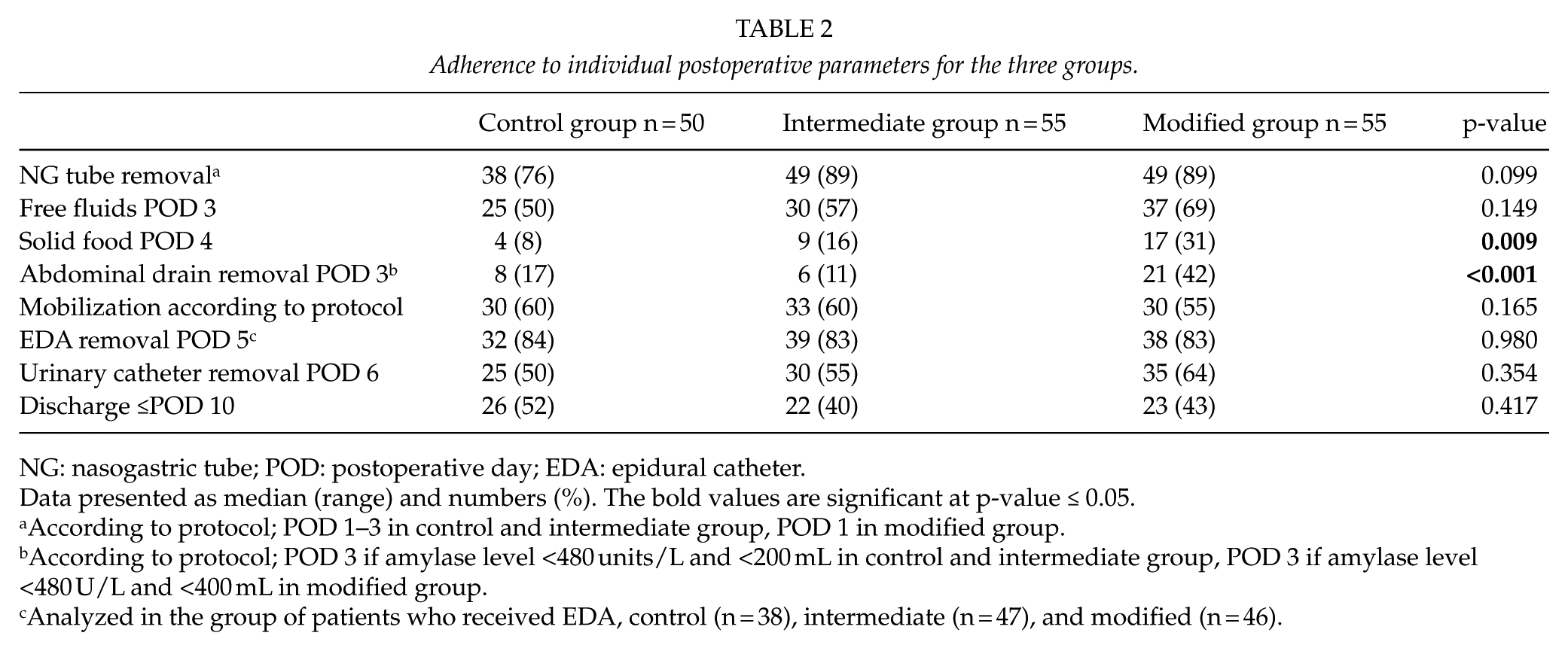
NG: nasogastric tube; POD: postoperative day; EDA: epidural catheter.
Data presented as median (range) and numbers (%).
The bold values are significant at p-value ≤ 0.05.
According to protocol; POD 1–3 in control and intermediate group, POD 1 in modified group.
According to protocol; POD 3 if amylase level <480 units/L and <200 mL in control and intermediate group, POD 3 if amylase level <480 U/L and <400 mL in modified group.
Analyzed in the group of patients who received EDA, control (n = 38), intermediate (n = 47), and modified (n = 46).
Number of patients fulfilling overall adherence to enhanced recovery program, correlated to day of discharge and major complications.
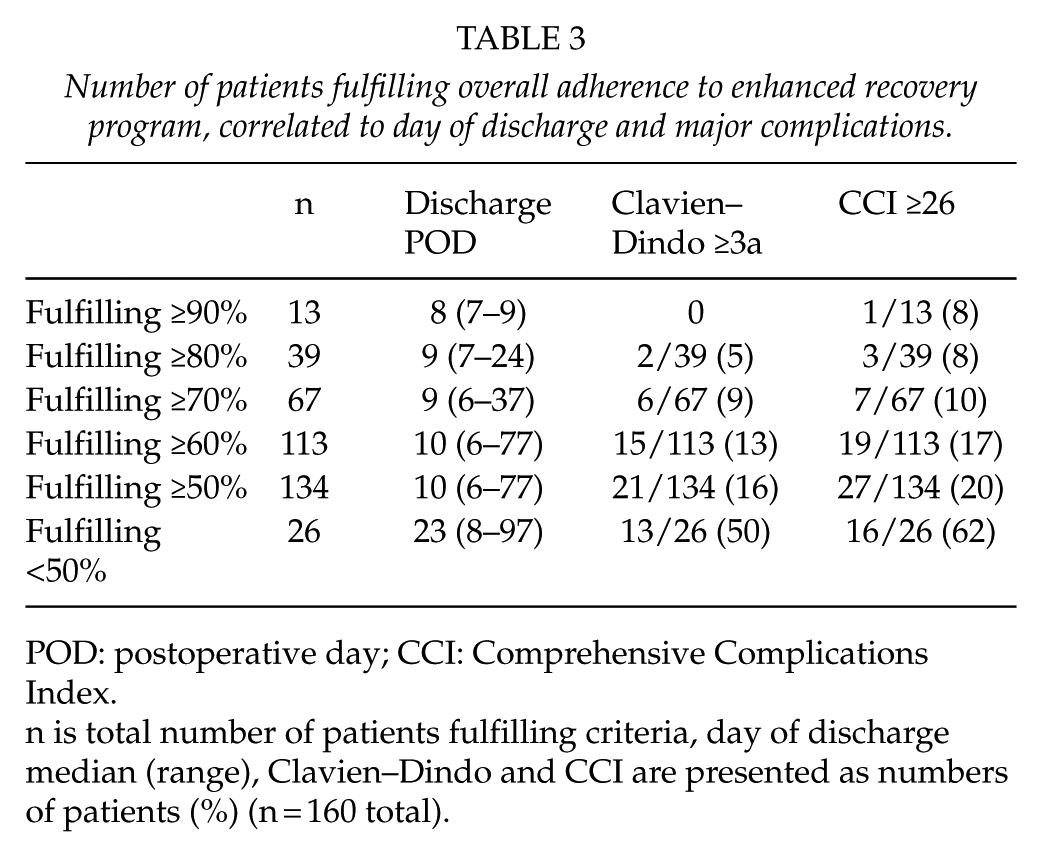
POD: postoperative day; CCI: Comprehensive Complications Index.
n is total number of patients fulfilling criteria, day of discharge median (range), Clavien–Dindo and CCI are presented as numbers of patients (%) (n = 160 total).
Discussion
This retrospective study reports 3 years of follow-up after implementation of an ERP for PD with pancreaticogastrostomy. This study shows that the initial results were reasonably well sustained, even with modification of two items in the postoperative care. Compliance with the protocol has increased, and the postoperative complications or hospital LOS did not change significantly.
The ERP was implemented at this institution on October 2012, resulting in decreased DGE, LOS, and costs, without an increase of complications or readmissions (8). The modification of the criteria for removal of nasogastric tube and abdominal drain arose from the positive experiences with the program and support in literature (16).
There are several reports on outcome of ERPs for PD (1–11, 26), but there is insufficient knowledge about how the patients adhered to these programs. Braga et al. (6) presented a high adherence to preoperative and intraoperative protocol items, 84%–100%, and a postoperative item compliance of 38%–66%. Patients with an uneventful course had significantly higher compliance, suggesting that patients with low early postoperative compliance should be carefully assessed for complications. Comparable results for preoperative adherence and a possible association between low adherence and postoperative complications were presented by Zouros et al. (2). The postoperative adherence rates were though much higher, 75%–96%, in the series by Zouros. In accordance with Braga, this study shows a high adherence to preoperative and intraoperative protocol items (>90%), and lower adherence (48%–58%) to postoperative items. Moreover, the group of patients with a high adherence rate had fewer complications and shorter LOS. The fulfillment of postoperative items is naturally more difficult, since they are affected by complications, lack of patient motivation, or incorrect information from the medical staff.
Implementation of a new routine can be a complex process that requires time as well as personal and financial investments (27). Once implementation has succeeded, there is a risk for relapse into old routines when the novelty effect vanishes. To avoid wasting valuable health-care resources, it is important that achieved benefits are sustained (14). An initial report of a new routine can be prone to the Hawthorne effect (28). In this case, the health-care personnel might have been more vigilant and adhered more strictly to protocol when they were aware on the on-going ERP implementation study, causing a temporary and exaggerated improvement of results (28). To evaluate the true outcome of the ERP, a follow-up was necessary.
This is probably one of the first studies to present the continued adherence rate to the preoperative, intraoperative, and postoperative elements in an ERP for PD. Contrary to reports from colorectal surgery (14, 15), this study did not reveal a decrease in adherence in the post-implementation phase. The modification of the protocol might have influenced the involved health-care personnel, since the modification process brings new attention to the protocol, and repeated education was performed. The importance of repeated training and dedicated personnel for optimal adherence has been previously presented (29). We do not have a specialized nurse practitioner for evaluation and audit of the ERP adherence. The novelty effect might be part of the increasing adherence rates in the MG.
The nasogastric tube was removed earlier, and there was a higher adherence to this item in the post-implementation phase. This reflects the modified criteria for removal of the nasogastric tube. Of note is that reinsertion of nasogastric tubes has more than doubled and is considerably higher than reported by others (1, 3, 30). The reason for this is not clear. Some of the parameters showed indications of worse outcome, such as the rate of DGE, reoperations, and major complications, although none significant. The background data for the groups were well comparable, except for more vascular resections in the MG, suggesting that more advanced tumors were accepted for surgery in recent past. There is a possibility that more challenging resections and reconstructions caused more adverse effects. Another aspect to consider is that studies supporting omission of nasogastric tube following PD, perform a pancreaticojejunostomy in reconstruction (3, 6, 7), and not a pancreaticogastrostomy as standard in our institution. Further evaluation of the most appropriate management of nasogastric tubes is needed.
Postoperative LOS was used as a surrogate marker for patient recovery in this study. Over the study time, there was a tendency to increase, though not significant, LOS in the post-implementation phase. There was no significant increase of complications. During collection of data from medical records, it was clear that, even though patients fulfilled discharge criteria, they stayed hospitalized over weekends to be discharged on Monday. This indicates a decreased tendency in discharging patients during weekends in the post-implementation phase. The phenomenon of not discharging patients despite meeting all discharge criteria has been previously described (12), although for unknown reasons. Functional recovery might have been a better outcome measure but was unfortunately not recorded.
Limitations of this study include its retrospective design. Occasionally, missing data were encountered. The actual performance of care elements could have been underestimated at times, due to a vague registration in the medical record. A confounding effect of postoperative recovery may exist when assessing postoperative components as item compliance (cause) and not as early functional outcome (effect), as advocated by others (15).
Conclusion
The positive outcome of an ERP for PD was reasonably well sustained. Compliance with the protocol has increased, but strict adherence remains a challenge, especially with the postoperative items.
Footnotes
Acknowledgements
This paper was presented at the 12th biennial E-AHPBA Congress 23–26 May 2017, Mainz, Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval by Human Ethics Committee at Lund University (2015/833).