
Abstract
Background and aims:
Early rehabilitation protocols should be assessed in elderly. We aimed to study the outcomes of colorectal surgery and the observance of the modalities of an early rehabilitation protocol in patients over 80 years.
Material and Methods:
All consecutive patients who underwent surgery for colorectal cancer in our center over a 19-month period were included. All of these patients were managed using the same early rehabilitation protocol. Patients older than 80 were compared to younger patients.
Results:
A total of 173 patients were included and 36 were ≥80 years (20.8%). Patients aged ≥80 years had a significantly higher ASA score and were operated on in emergency. In the peroperative period, patients aged ≥80 years were more likely to undergo laparotomy than patients <80 years in univariate analysis (p = 0.048), but in multivariate analysis, the choice for a laparoscopy was influenced by ASA score ≤2 (odds ratio = 3.55, 95% confidence interval = 1.67–7.58) and emergency surgery (odds ratio = 0.18, 95% confidence interval = 0.06–0.50). In the postoperative period, peristalsis stimulation and vascular catheter ablation were significantly better followed in Group 1 (p = 0.012 and 0.031). However, in multivariate analysis, age was not significantly associated with these parameters. Peristalsis stimulation was influenced by ASA score ≥2 (odds ratio = 4.27, 95% confidence interval = 1.18–15.37) and vascular catheter ablation was also influenced by ASA score ≤2 (odds ratio = 2.63, 95% confidence interval = 1.33–5.21). Emergency surgery had a strong trend to influence these parameters (p = 0.08).
Conclusion:
Although age or comorbidities may affect observance for certain modalities such as chewing gum use and vascular catheter ablation, an early rehabilitation protocol can be used after colorectal cancer surgery in patients ≥80 years old, where it would improve functional results and postoperative outcomes.
Introduction
Surgery with or without associated chemotherapy is the current gold standard for the curative treatment of resectable, non-metastatic colorectal cancer. R1 colonic cancer resection is associated with locally advanced poorly differentiated tumors and an increased rate of recurrence (1). However, in some cases of symptomatic cancer with unresectable metastases, palliative surgery can be proposed. The incidence of colorectal cancer is growing: an estimated 132,700 new cases will occur in 2015 in the United States (2). The world population is growing older, and a recent report from Arai et al. (3) concluded that 13% of the total elderly population is in need of care. Today, physicians frequently encounter patients over the age of 80 with colorectal cancer that should be treated surgically. These elderly patients generally present comorbidities that could contribute to postoperative morbidity and mortality (4). Several studies have shown that laparoscopic surgery provides better postoperative outcomes in elderly patients (5–8). However, the age thresholds at which these advantages manifest remain unclear, and only a few studies have focused specifically on people older than 80. One of those studies reported that perioperative morbidity worsened as performance status increased (9). Others showed that laparoscopic surgery in elderly colorectal cancer patients with poor performance status was safe and not inferior to open surgery (7) and that it was not associated with patterns of death (6).
Although the feasibility and safety of surgery in elderly patients have been confirmed in the literature, the use of early rehabilitation protocols has not been thoroughly examined. Several studies reported that rehabilitation protocols can be implemented in patients aged 65 years and older (10–13), noting that one of those studies identified age >80 as a predictor of delayed mobilization and prolonged hospital stay (12). To the best of our knowledge, only one study, excluding emergency surgery, focused on patients aged 80 years or more (14).
Perioperative early rehabilitation protocols developed and recommended by the Enhanced Recovery After Surgery (ERAS) society (15–18) are associated with shorter hospital stays and lower risks of perioperative complications (19–21), but a number of modalities included in those protocols could be difficult to apply in weak patients, essentially because of standing dogmas among clinicians.
The aim of this work was to study the outcomes of colorectal surgery and the observance of the modalities composing our early rehabilitation protocol in patients aged 80 years or more.
Materials and Methods
This is a prospective observational study of a cohort of patients who underwent colorectal resection in one tertiary referral center (Angers University Hospital, Angers, France) between 1 May 2013 and 31 October 2015. The study was approved by the Hospital’s Ethics Committee.
All patients who underwent elective or emergency surgery for colorectal cancer were included in this study. Surgical access and tumor location were not exclusion criteria.
An early rehabilitation protocol used in routine practice in our center since December 2012 was implemented for the included patients.
Patients who needed programmed postoperative intensive care were excluded from the study as they did not follow the protocol.
A total of 173 patients were included and a part of them has been included in a previous study in which we showed that enhanced recovery programs reduce the duration of postoperative ileus (22).
Patient data were recorded in a computerized and anonymous database. Data were recorded prospectively for all patients undergoing colorectal surgery, in the aim to provide a regular audit of our practice, as recommended by the ERAS Society. They included (1) clinical characteristics (age, gender, ASA (American Society of Anesthesia) score, comorbidities, treatment and TNM stage), (2) perioperative care items (those from our protocol), and (3) postoperative outcomes (morbidity, delay to flatus recovery, delay to stool recovery, delay to bowel motility recovery, theoretical length of hospital stay, effective length of hospital stay).
Malnutrition was defined as almost one of the three conditions below:
Serum prealbumin <110 mg/L;
Serum albumin <30 mg/L;
Body mass index (BMI) <20 kg/m2 if age <70 years or BMI <17 if age >70 years.
Postoperative ileus was defined as the absence of stool recovery associated with vomiting lasting more than 3 days. A nasogastric tube was introduced in case of vomiting.
Morbidity was classified using the Dindo et al. (23) classification. Grade III or greater complications were considered severe.
Theoretical length of hospital stay was defined by the day at which the patient could theoretically be discharged, but was not, because he or she was waiting for a transfer to another department.
Effective length of hospital stay was defined by the day at which the patient was effectively discharged to home or another institution.
Two groups were defined: Group 1 comprised patients aged less than 80 years and Group 2 those aged 80 years or more.
Categorical data were expressed as percentages and compared using chi-square or Fisher exact tests. Continuous data were expressed as medians (interquartile ranges) and compared using the Mann–Whitney test. The type I error was set to 0.05. Data analyses were performed using SPSS software, version 15 (SPSS, Chicago, IL).
p < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 173 patients, 36 of whom were aged ≥80 years (20.8%), were included in the study (Table 1).
Patient and surgical characteristics.
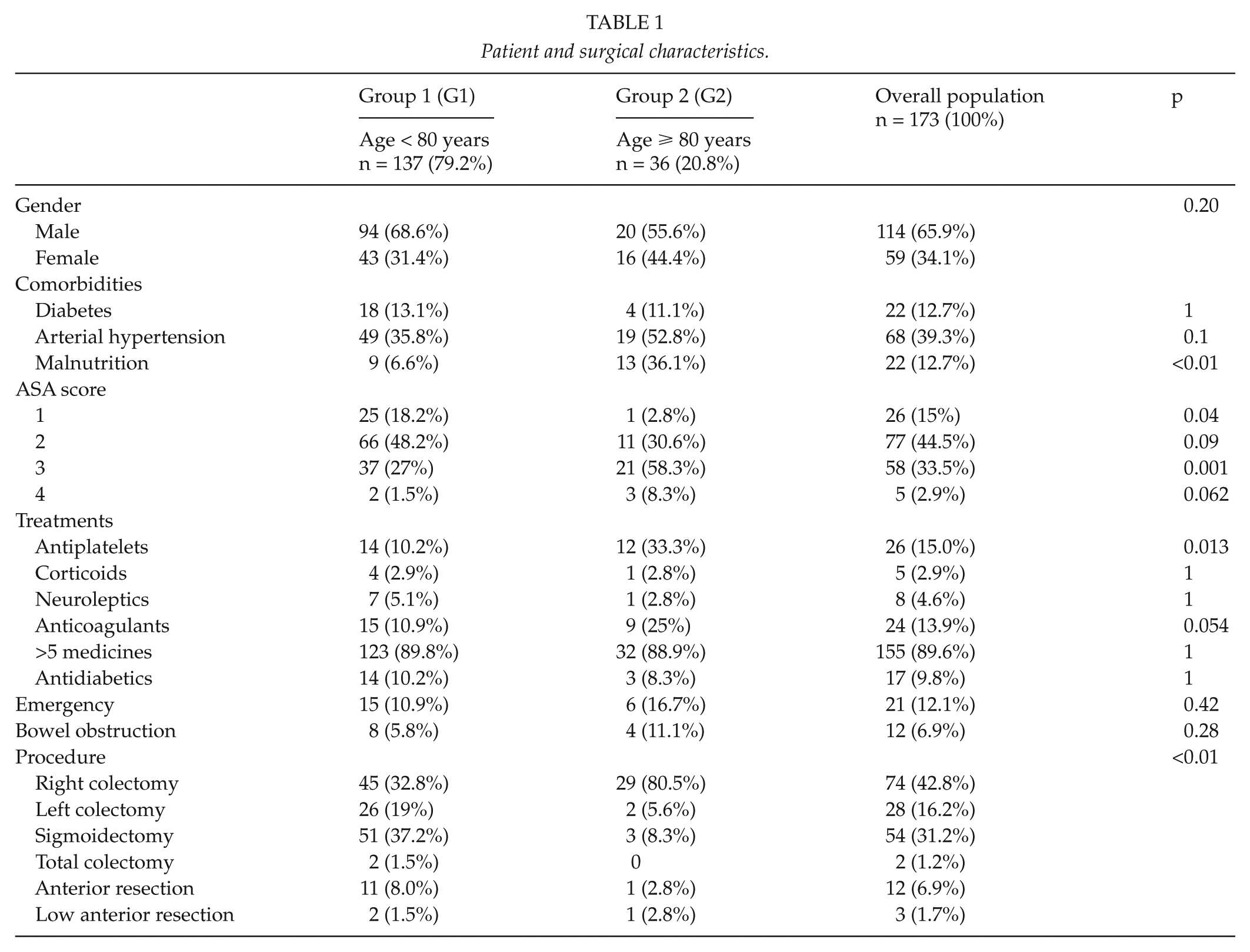
Median ages were 61 years (52; 72) in Group 1 and 85 years (82; 88) in Group 2.
Patients aged ≥80 years had statistically an ASA score higher (ASA, 3–4) (p < 0.0001) than patients aged <80 years and had significantly more malnutrition (p < 0.0001).
Patients of Group 2 had more frequently a treatment with antiplatelets than patients of Group 1 (p = 0.013).
There was a difference as concerns the type of surgical procedure (localization of the colectomy) between the two groups (p < 0.001).
Early Rehabilitation Protocol Modality Observance
Observance of protocol modalities in the overall population ranged from 26% to 100% (Table 2).
Enhanced recovery program observance.
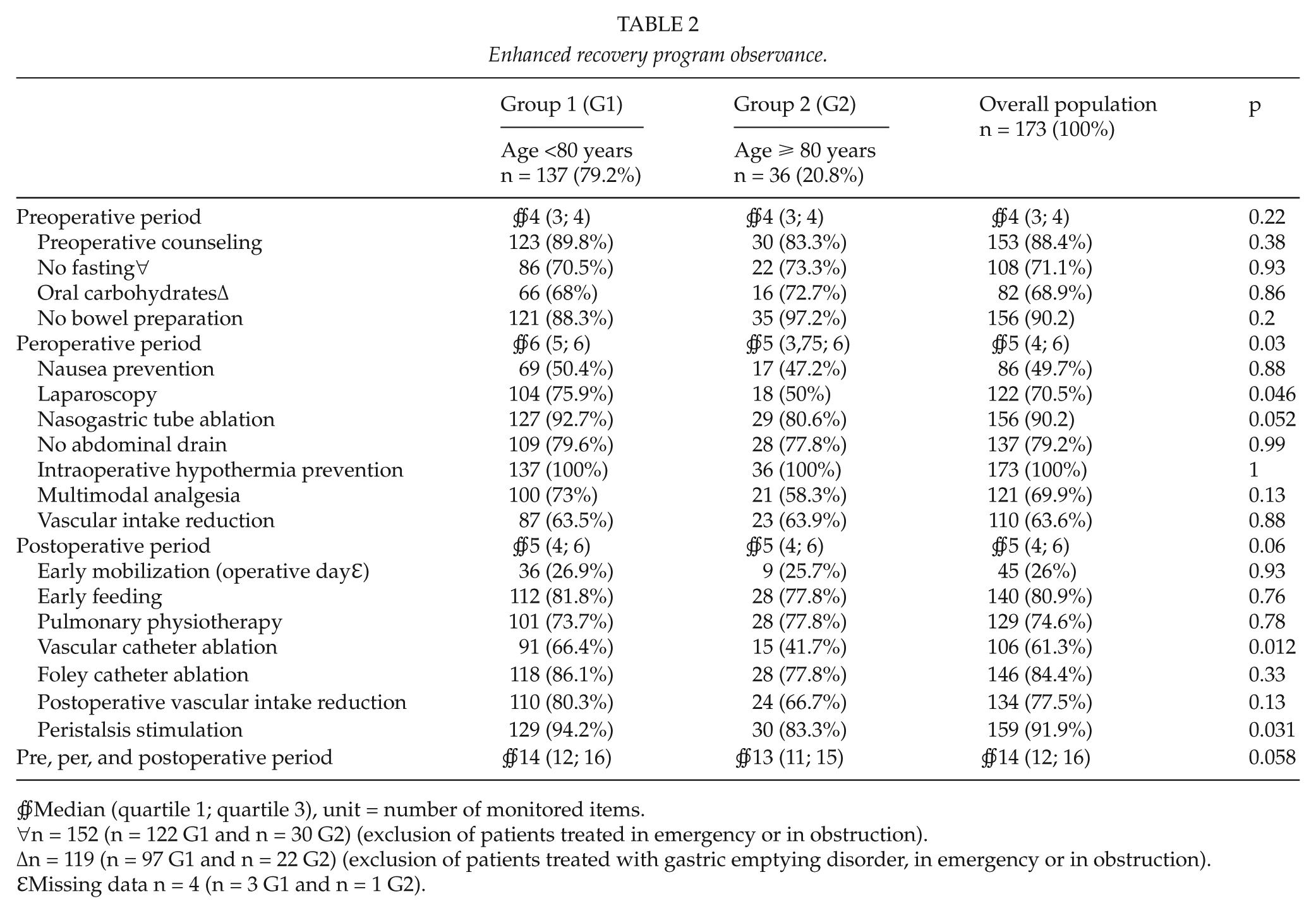
∯Median (quartile 1; quartile 3), unit = number of monitored items.
∀n = 152 (n = 122 G1 and n = 30 G2) (exclusion of patients treated in emergency or in obstruction).
Δn = 119 (n = 97 G1 and n = 22 G2) (exclusion of patients treated with gastric emptying disorder, in emergency or in obstruction).
ℇMissing data n = 4 (n = 3 G1 and n = 1 G2).
In the overall population, the median of the compliance of protocol modalities was 14 items. Patients in Group 2 had a significantly poorer peroperative compliancy than Group 1 (p = 0.03). Laparoscopy was significantly more often used (p = 0.046) in Group 1. In the postoperative period, peristalsis stimulation and vascular catheter ablation were significantly better respected in Group 1 (p = 0.012 and 0.031).
Postoperative Outcomes
Severe complications occurred in 9.8% of the overall patient population (Table 3). There were statistically significant differences between the outcomes, in terms of postoperative ileus and superficial surgical site infection (p = 0.018 and 0.002) what Group 2 was more likely to experiment.
Postoperative morbidity and mortality.
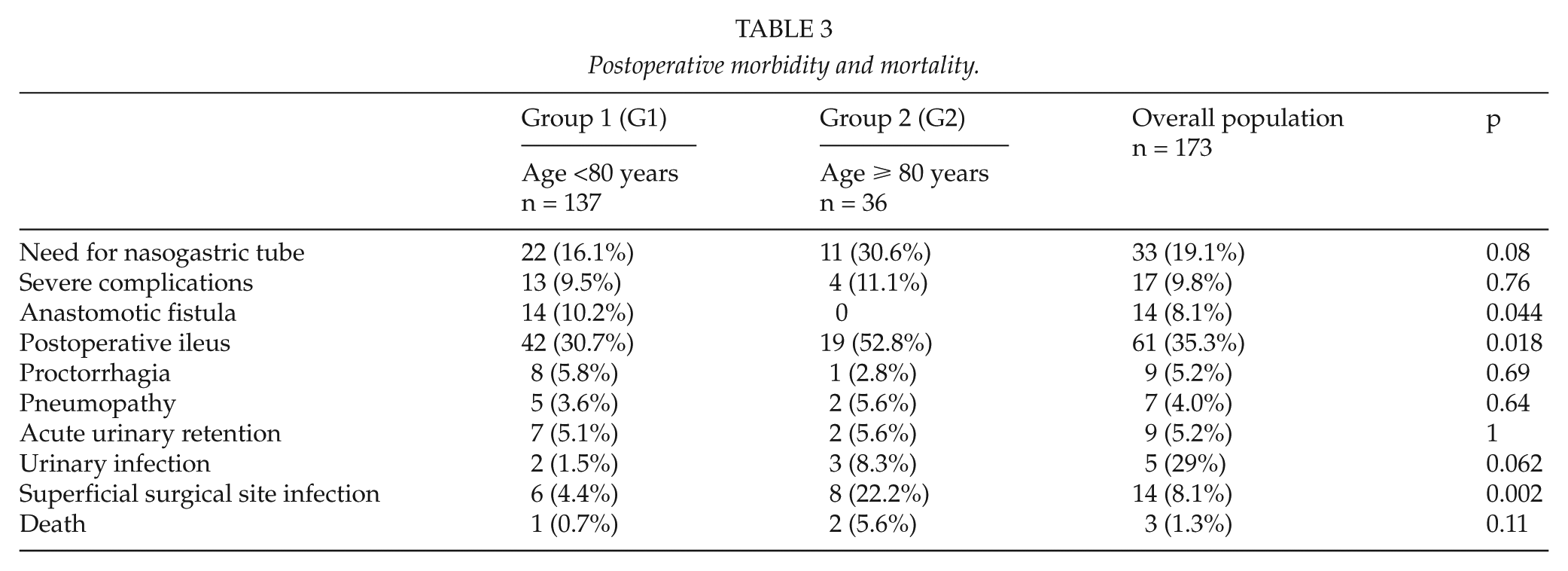
One patient died in Group 1 (0.7%) and two (5.6%) in Group 2.
Delay to Bowel Motility Recovery and Length of Hospital Stay
The median delay to gas recovery (2 days (1; 2) in Group 1 vs 2 days (1; 3) in Group 2) was not significantly different between the two groups (p = 0.07) and the median delay to stool recovery (3 days (2; 4) in Group 1 vs 3 (2; 5) in Group 2) (p = 0.11) was not too.
The median effective lengths of hospital stay were 6 days (4; 9) for Group 1 and 11 days (7.25; 14.5) for Group 2 (p < 0.001). The median theoretical lengths of hospital stay were 5 days (4; 8) for Group 1 and 8 days (5; 11.75) for Group 2 (p = 0.008).
Unexpected Rehospitalization
There were 2 rehospitalizations in Group 2 and 10 in Group 1 (p > 0.5) (12 patients on 134 (9%) for the overall population).
Mutlivariate Analysis
In multivariate analysis, age ≥80 years did not significantly influence laparoscopic use (p = 0.10), compliance with vascular catheter ablation (p = 0.11), compliance with peristalsis stimulation use (p = 0.32), or compliance with immediate nasogastric tube removal (p = 0.12; Table 4).
Multivariate analysis of different items of the enhanced recovery program that differed between the patients ≥ 80 years and the patients <80 years in univariate analysis.
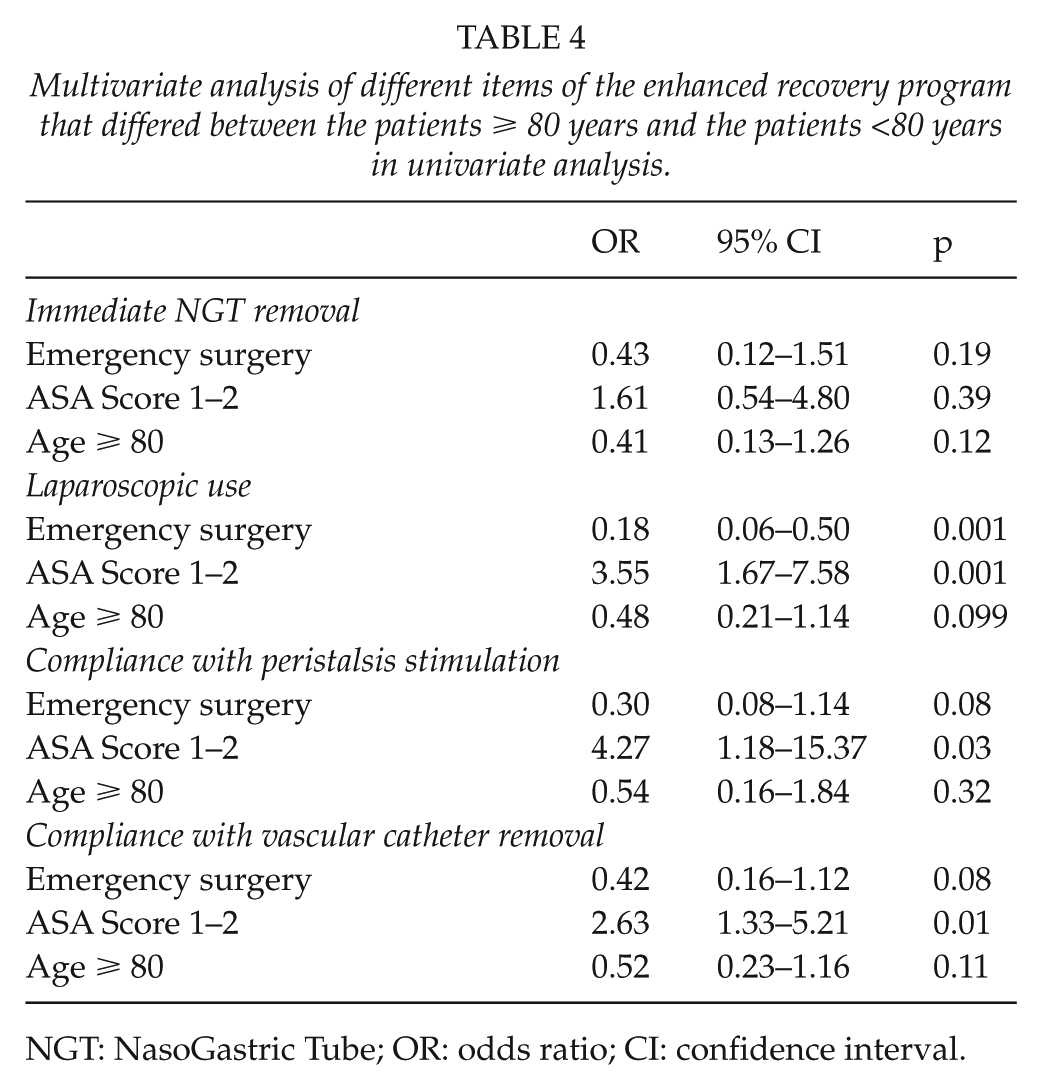
NGT: NasoGastric Tube; OR: odds ratio; CI: confidence interval.
ASA score ≤2 significantly influenced peristalsis stimulation compliance (odds ratio (OR) = 4.27; 95% confidence interval = 1.18–15.37), laparoscopic use (OR = 3.55; 95% confidence interval = 1.67–7.58), or vascular catheter ablation (OR = 2.62; 95% confidence interval = 2.63–1.33), whereas emergency surgery significantly influenced laparoscopic use (OR = 0.18; 95% confidence interval = 0.06–0.50; Table 4).
Discussion
Among the 173 patients included in this cohort, 36 (20.8%) were 80 years or older. In this more elderly population, protocol modality compliance ranged from 25% to 100%.
A recent report focusing on patients aged 65 years or more showed rates of protocol modality compliance between 28% and 87% (10). More recently, Pedziwiatr et al. (14) reported no difference of compliance between a group of patients >80 years and a group of patients <50 years, apart from opioids consumption. They reported more than 80% of compliance in overall population and did not report any difference between groups. We report compliance lesser than this probably because we assessed 18 items (78% were followed in group 1 whereas 72% were in group 2 (p > 0.05)). This difference of compliance may probably be due to the fact that we also included emergency surgery that was excluded by Pedziwiatr et al. Indeed, emergency surgery is known to provide lesser compliance than elective surgery (10), and we found a significant influence of emergency surgery on laparoscopic use (p = 0.001) and a strong trend of its influence on compliance with vascular catheter ablation and peristalsis stimulation (p = 0.08 and 0.08).
Another report stated that very elderly should be considered after 75 years and authors also concluded in the feasibility of enhanced recovery programs over 75 years (24). Our results agreed with the literature because no impact of age was found in multivariate analysis, when age was corrected by ASA score and emergency surgery.
In colorectal populations irrespective of age, Ahmed et al. (25,26) reported protocol modality compliance rates ranging from 25% to 100%, while pointing out that the implementation of certain modalities of early rehabilitation protocols is difficult outside of the clinical study setting (25,26). Our rates of compliance are in accordance with the literature.
Furthermore, in our study, the compliance rates for two modalities differed significantly between Group 1 (age <80 years) and Group 2 (age ≥80 years) in univariate analysis. Indeed, the rate of chewing gum use in the postoperative phase differed from 83.3% for Group 2 to 94.2% for Group 1 (p = 0.031), but in multivariate analysis, only ASA score was significantly associated (OR = 4.27; p = 0.03). Chewing gum has been shown to fasten the recovery of bowel motility (27), but in weaker patients, this modality may not be applicable due to poor oral health, the presence of dental prostheses, or the severity of comorbidities (chronic obstructive bronchopneumopathy).
The other difference between the two groups is the early vascular catheter ablation that was more likely to be followed in younger patients in univariate analysis but not in multivariate analysis in which ASA score was the only factor significantly associated with the compliance with this item (OR = 2.63; p = 0.01). This is probably due to the fear of early complications or the need of treating early complication such as postoperative delirium. Indeed, Raats et al. (28) recently reported a 21% incidence rate for postoperative delirium after colorectal surgery and that this complication occurred in patients with a median age of 82 years. We did not specifically record this complication in our study, but within this dynamic may lie an explanation for the difference in early vascular catheter ablation compliance between our two groups.
Our study does have several limitations. First, a control group of patients aged ≥80 years would have been of interest for our study. However, we did compare this age group to a younger group and found no important differences in characteristics between them, apart from the age.
Also, our compliance rates can be slightly lesser than those reported in the literature, but this is probably because we decided to include patients undergoing urgent surgery. This draws a better picture of our practice, and this is more representative of the population.
Literature is weak on feasibility, compliance, and safety of enhanced recovery programs in elderly, and the need of cohort studies is important. Our results should help and reassure physicians in their choice to implement an early rehabilitation protocol for elderly patients.
Finally, results regarding malnutrition should be considered with caution because our definition did not take into account loss of weight because of a higher part of missing data due to the retrospective characteristic of this study. However, despite this limitation, our results showed a higher proportion of malnutrition in elder patients, as it is reported in the literature (29), and should awake the physician to the potential higher risk of postoperative morbidity of these patients, already at risk of morbidity due to their higher rate of comorbidities.
Conclusion
Age significantly influenced compliance with vascular catheter removal and peristalsis stimulation in univariate analysis but not in multivariate analysis. Differences observed in univariate analysis were due to ASA score difference between the two groups of age. However, age is not a brake to enhanced recovery programs application, but these programs should be adapted to ASA score to suit perfectly to patient individuality and to be performed safely.
Footnotes
Acknowledgements
The authors acknowledge Mr Kevin Erwin for his kind help in the translation of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.