
Abstract
Background:
This study examined short-term clinical outcomes and in-hospital costs of laparoscopic and open colonic resection within fast-track and traditional care pathways.
Material and Methods:
A case–control study was performed. From 2007 to 2009, 116 patients underwent laparoscopic or open colonic resection for benign or malignant disease within fast-track care pathway. The control group consisted of 116 age-, sex-, comorbidity-, type of surgery–, and diagnosis-matched patients who received a traditional perioperative care from 2000 to 2007. The main measures of outcome were postoperative hospital stay and in-hospital costs, with 30-day mortality, morbidity, reoperation, and readmission rates as secondary outcomes.
Results:
The study groups were well balanced for baseline characteristics. Postoperative hospital stay was shorter in the fast-track than in the control group: laparoscopic resection median 3 versus 5 days (p < 0.001) and open resection 4 versus 7 days (p < 0.001). In multivariate analysis fast-track care, laparoscopic surgery and complications were independent determinants affecting the length of hospital stay. Overall, there was a trend toward lower in-hospital costs in the fast-track group compared with the traditional care group, but the difference was not statistically significant. Open surgery within fast-track care was the least costly option compared to laparoscopic or open surgery within traditional care but not significantly so when compared with laparoscopy within fast-track care. Intake of solid food and bowel function recovered 1 day earlier in the fast-track group than in the control group (p < 0.001). Complications were more frequent after open surgery than after laparoscopic surgery (23.3% vs 11.0%, p = 0.012). Reoperation and readmission rates were similar between the study groups.
Conclusion:
Laparoscopy improves the efficiency of fast-track perioperative care without significantly increasing in-hospital costs.
Keywords
Introduction
Randomized trials and meta-analyses have now demonstrated the safety and efficacy of fast-track perioperative care in colorectal surgery, not only in reducing postoperative hospital stay and morbidity but also in improving patient convalescence and satisfaction when compared with traditional care (1–10). The concept is based on multimodal evidence-based care platform and includes preoperative education and optimization of patients, attenuation of surgical stress response, optimized pain control, and postoperative rehabilitation with enforced oral nutrition and early ambulation (11, 12).
The role of laparoscopy in the fast-track setting has been controversial. Several randomized trials comparing laparoscopic versus open resection for colon cancer within traditional perioperative care have shown that the laparoscopic method can provide an equivalent oncologic outcome, a faster short-term recovery, and shorter hospital stay than the open method (13–15). A recent randomized trial (16) showed that laparoscopic colonic surgery within fast-track care resulted in faster recovery and shorter hospital stay than open surgery without increasing in-hospital costs in contrast to another study demonstrating no such difference (7).
At present, level 1 evidence is missing to show that there is an additive effect by combining laparoscopic surgery and fast-track perioperative care (2). It is also uncertain whether laparoscopic colonic surgery improves the economic efficiency of fast-track perioperative care in comparison with open surgery, despite the fact that the cost-effectiveness of enhanced recovery pathways for colorectal surgery is supported by a recent meta-analysis (17). The objectives of this study were to compare short-term clinical outcomes and in-hospital costs between laparoscopic or open colonic resection within either fast-track or traditional perioperative care pathways. Determinants affecting the length of postoperative hospital stay were also examined.
Material and Methods
Patients and Study Design
A non-randomized case–control study was performed. The fast-track group included 116 patients who underwent laparoscopic (N = 73) or open (N = 43) colonic resection for benign or malignant disease from 2007 to 2009. Included were patients with a good mental and physical performance status having an attending person at home and the American Society of Anesthesiologists (ASA) score I–III. Elderly patients fulfilling the predefined criteria were also included. Excluded were patients who underwent emergency surgery or a major multiorgan resection. Body mass index >35 kg/m2 and patients with significant cardiac/pulmonary comorbidity in whom a prolonged laparoscopic surgery would have been potentially harmful were relative contraindications to laparoscopy. Data on patients who underwent open or laparoscopic surgery in the fast-track setting were collected prospectively. The control group consisted of 116 age-, sex-, comorbidity-, type of surgery–, and diagnosis-matched patients who received a laparoscopic or open colonic resection within traditional perioperative care from 2000 to 2007. Data on open surgery were collected retrospectively, whereas laparoscopic data were retrieved from a prospective colorectal database. Hospital records were reviewed regarding perioperative data and instrument use. All patients were followed up for 30 days to assess morbidity and readmissions. The study was approved by the ethics committee of the hospital.
Fast-track and Traditional Perioperative Care Protocols
In accordance with a recent international consensus review (12), the fast-track protocol included 20 evidence-based fast-track elements (Table 1). Briefly, extensive preoperative counseling, oral carbohydrates until 2 h before surgery, totally intravenous anesthesia (TIVA) using short-acting anesthetics (propofol–remifentanil and cis-atracurium for muscle relaxation) instead of traditional inhalation anesthesia (oxygen-sevoflurane and cis-atracurium for muscle relaxation), short duration of postoperative opioid-sparing analgesia (ropivacaine and fentanyl) with epidural catheter and a single-use pump scheduled to be removed on the second postoperative day, oral paracetamol and nonsteroidal anti-inflammatory drug (NSAID) started 2 days after surgery, and use of opioids only for breakthrough pain were the main differences between fast-track and traditional care. Furthermore, fast-track recovery was protocol driven with discontinuation of intravenous (IV) fluids as soon as possible, early postoperative feeding, removal of urinary catheter on the first postoperative day, and early mobilization. Prophylactic dexamethasone was not routinely used for postoperative nausea and vomiting during the study period. In both study groups, patients were discharged when they were afebrile, fully mobilized, tolerated three meals per day, had adequate pain control on oral analgesics, and adequate home support.
Comparison of fast-track and traditional care elements.
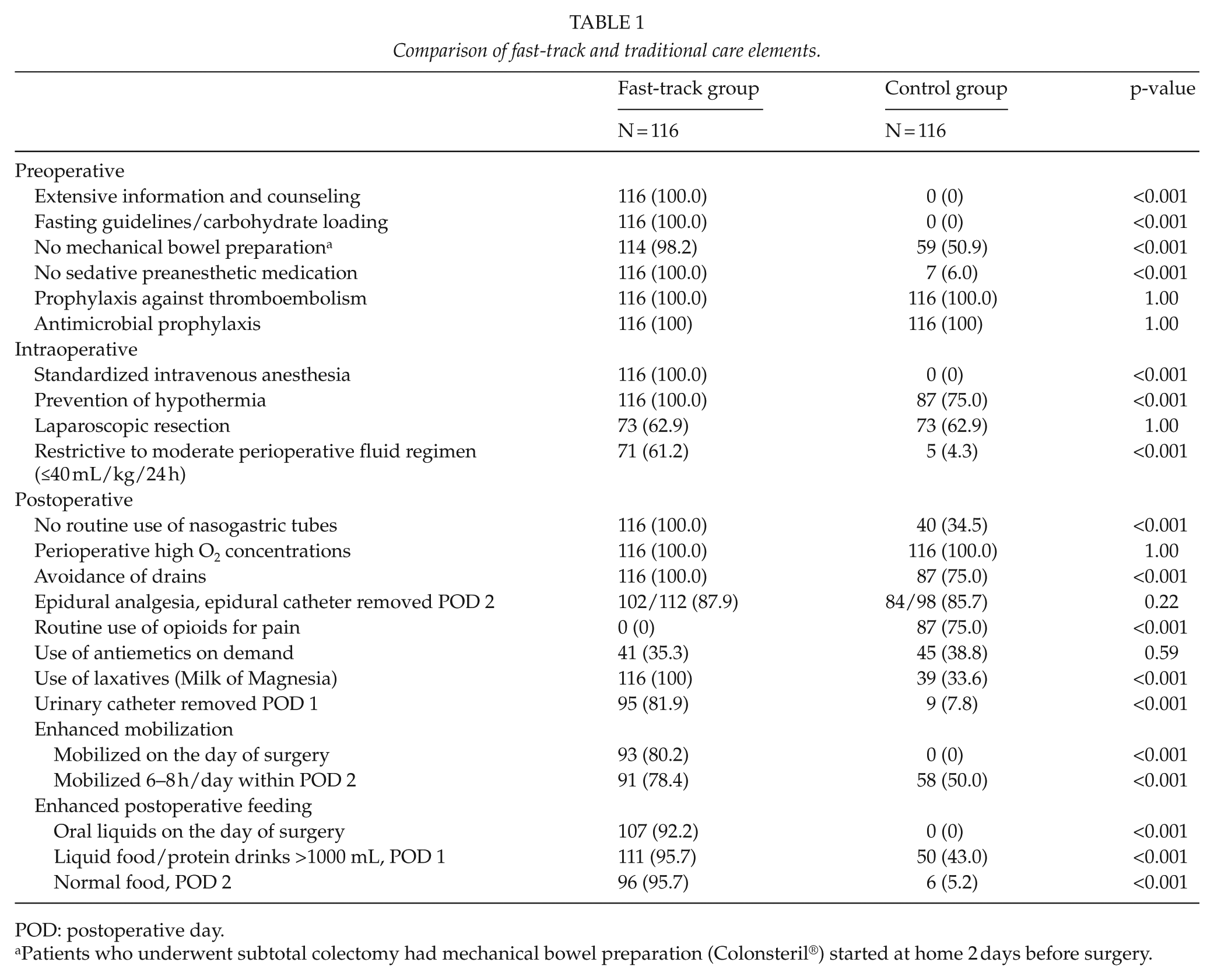
POD: postoperative day.
Patients who underwent subtotal colectomy had mechanical bowel preparation (Colonsteril®) started at home 2 days before surgery.
Surgical Technique
The operations were performed by senior staff surgeons with the participation of residents in training. The decision to do laparoscopic or open surgery within the inclusion criteria was left to the discretion of the operating surgeon. Laparoscopic colonic resection was performed using the five-trocar technique for right and left hemicolectomies. Specimens were extracted through a Pfannenstiel incision (left hemicolectomy) or a peri-umbilical incision (small bowel and ileocolic resection, right hemicolectomy). In the fast-track group, open surgery was performed using transverse incision for right hemicolectomies and midline incision for left hemicolectomies, whereas in the control group, open surgery was performed using midline incisions.
Definitions
Conversion to open surgery was defined as a necessity to interrupt the laparoscopic procedure and to proceed using conventional technique. Paralytic ileus was defined as the absence of bowel function for ≥5 days or the need for reinsertion of a nasogastric tube after starting oral diet in the absence of mechanical bowel obstruction. Complications were classified according to the Dindo–Clavien (18) classification. Postoperative hospital stay during index admission was defined as days spent in the hospital after surgery. Length of total hospital stay included preoperative, postoperative, and readmission-related days spent in the hospital.
Cost Evaluation
All costs were calculated according to the year 2010 prices (€). Pre-existing data on some major resources and their allocated costs in 2010 were obtained from the hospital administration (Table 2). Costs of operating room resources (basic costs, anesthesia and nurses, surgical team, instrument use) and recovery room services were calculated according to the time spent in the operating and recovery rooms, duration of surgery, and the level of training required. The costs of disposable instruments including circular and linear staplers for open and laparoscopic surgery, trocars, laparoscopic diathermy scissors, Harmonic scissors, and bipolar vessel sealers were calculated according to the use. Excluded were capital costs of reusable instruments and standard laparoscopic equipment, administration and traveling costs, and costs of different adjuvant chemotherapy treatments for stage III colon cancer.
Major resources and their allocated costs.
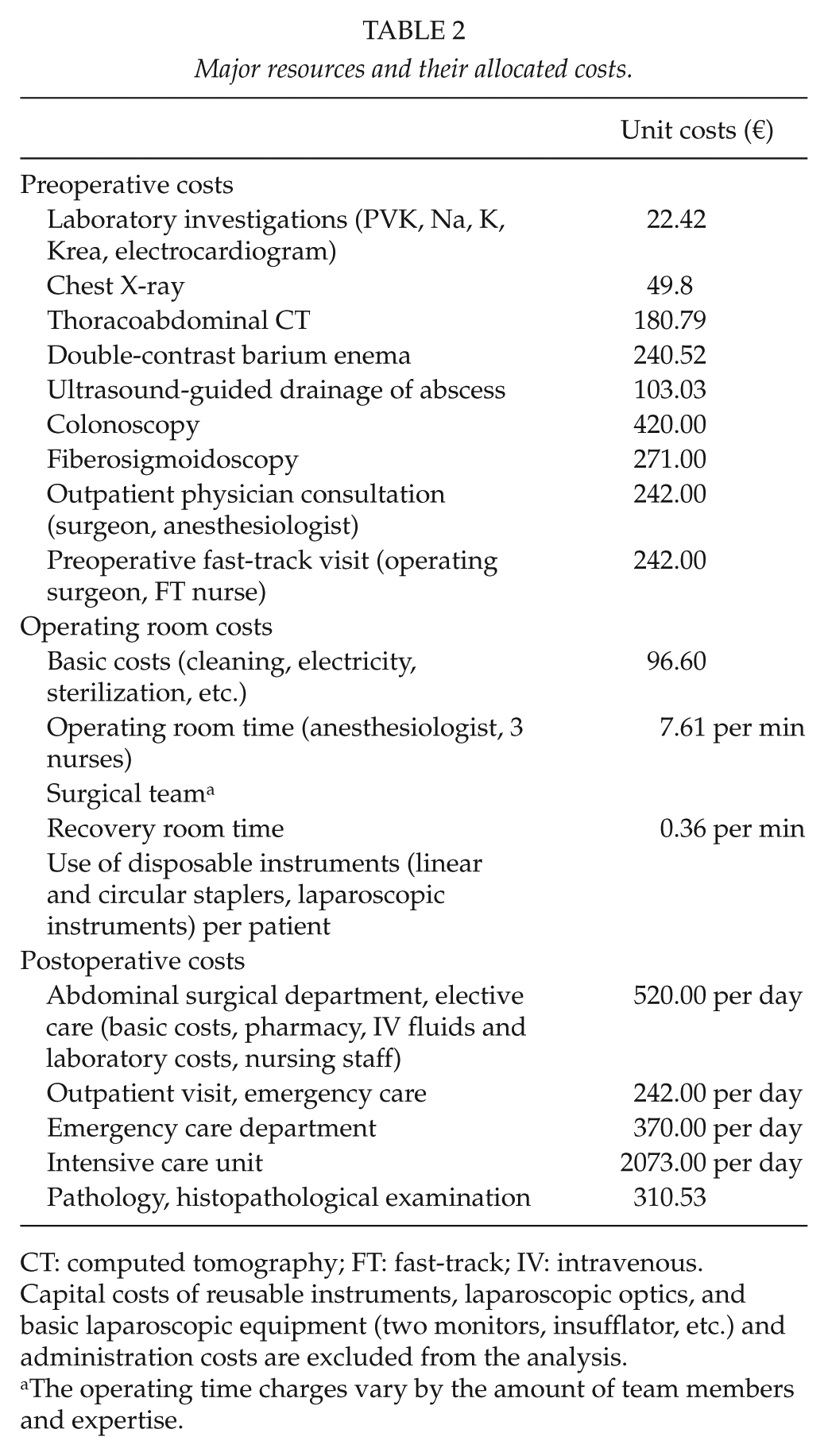
CT: computed tomography; FT: fast-track; IV: intravenous.
Capital costs of reusable instruments, laparoscopic optics, and basic laparoscopic equipment (two monitors, insufflator, etc.) and administration costs are excluded from the analysis.
The operating time charges vary by the amount of team members and expertise.
Statistical Analysis
The data were analyzed on an intention-to-treat basis considering laparoscopic and converted laparoscopic resections together. Results are given as mean (standard deviation, SD) or median (interquartile range, IQR). The comparison between groups was made using analysis of variance (ANOVA), Kruskal–Wallis, or chi-square test. Because the cost data in this study were very skewed, a bootstrap-type analysis (10,000 repetitions) was used. Analysis of determinants affecting postoperative hospital stay was done using univariate and multivariate zero-truncated Poisson regression models with robust standard errors or negative binomial regression (zero-truncated) models, when overdispersion is present. The length of hospital stay (LOS) ratio was expressed as the ratio of mean hospital days. Variables with p < 0.20 at univariate analysis were entered in the multivariate analysis. All statistical tests were two-sided. A p-value less than 0.05 was considered significant. STATA (StataCorp 2009. Stata release 12, Statistical Software. StataCorp LP, College Station, TX) was used for statistical analysis.
Results
Differences between fast-track and traditional care elements as well as the degree of adherence to the 20 predefined fast-track elements are shown in Table 1. Baseline characteristics did not differ significantly between the study groups (Table 3). Colon cancers and benign diseases (mainly adenomas and diverticular disease) were evenly distributed in the study groups. A total of 73 patients underwent laparoscopic and 43 open resection in the fast-track and control groups, respectively. Conversion to open surgery occurred in 6.8% and 5.5% of laparoscopically operated patients within fast-track and traditional perioperative care groups due to severe adhesions from previous open surgeries or diverticulitis.
Baseline clinical characteristics.
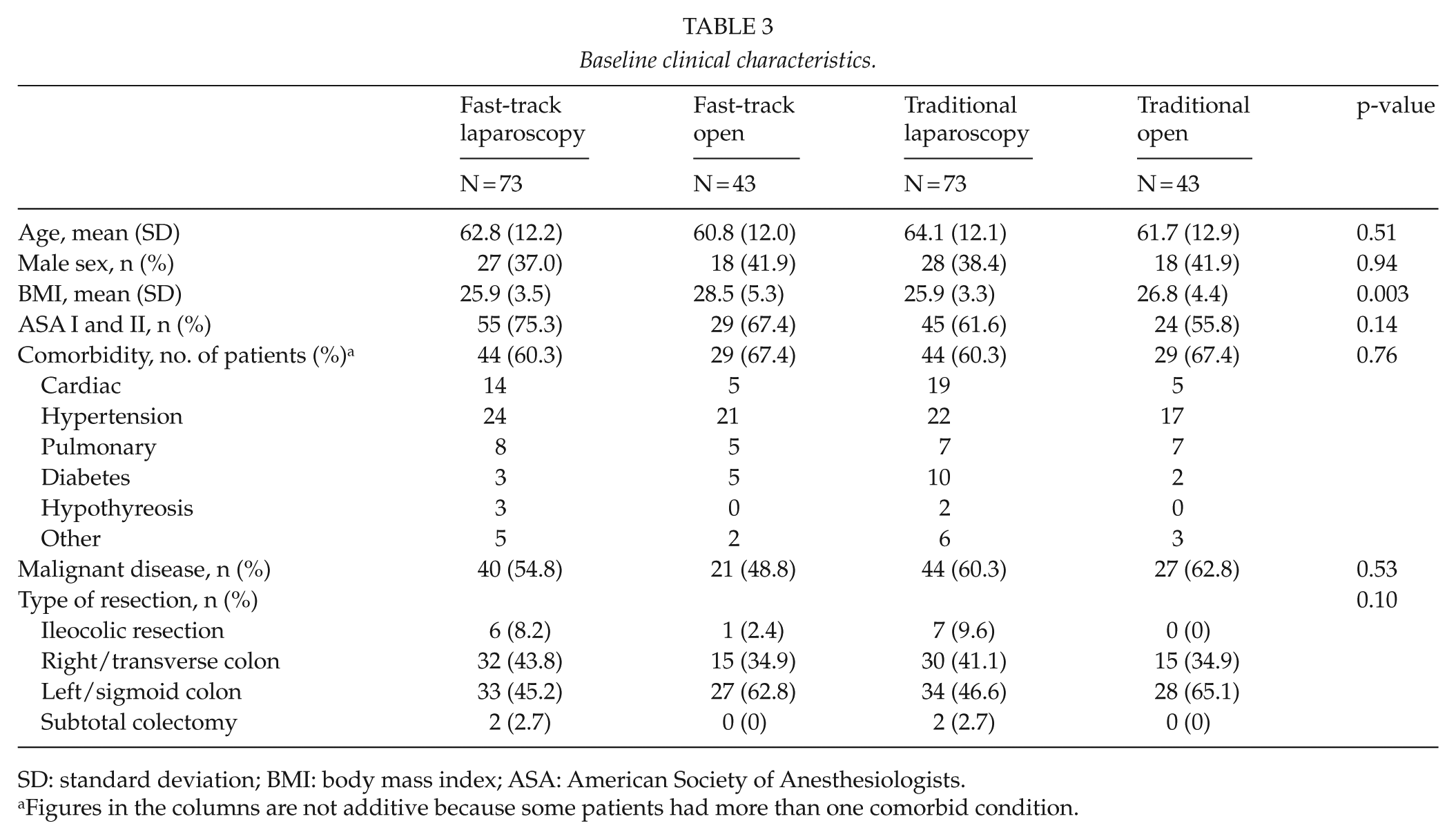
SD: standard deviation; BMI: body mass index; ASA: American Society of Anesthesiologists.
Figures in the columns are not additive because some patients had more than one comorbid condition.
Main Measures of Outcome
Postoperative hospital stay was shorter after laparoscopic than open surgery both in the fast-track group and in the control care group (Table 4): laparoscopic resection within fast-track care median 3 (IQR 3–4) days versus traditional care 5 (IQR 4.5–6) days (p < 0.001) and open resection within fast-track care median 4 (IQR 3–6) days versus traditional care 7 (IQR 6–9) days (p < 0.001). Using univariate and multivariate regression analysis, traditional perioperative care (LOS ratio 1.56 (95% confidence interval (CI): 1.39–1.74), p < 0.001), open surgery (1.17 (1.04–1.33), p = 0.009), general (1.73 (1.38–2.15), p < 0.001), surgical (1.85 (1.52–2.25), p < 0.001) complications, and severity of complications (Dindo–Clavien grade 3a-5 1.89 (1.55–2.31), p < 0.001) were factors increasing the LOS.
30-day surgical outcome.
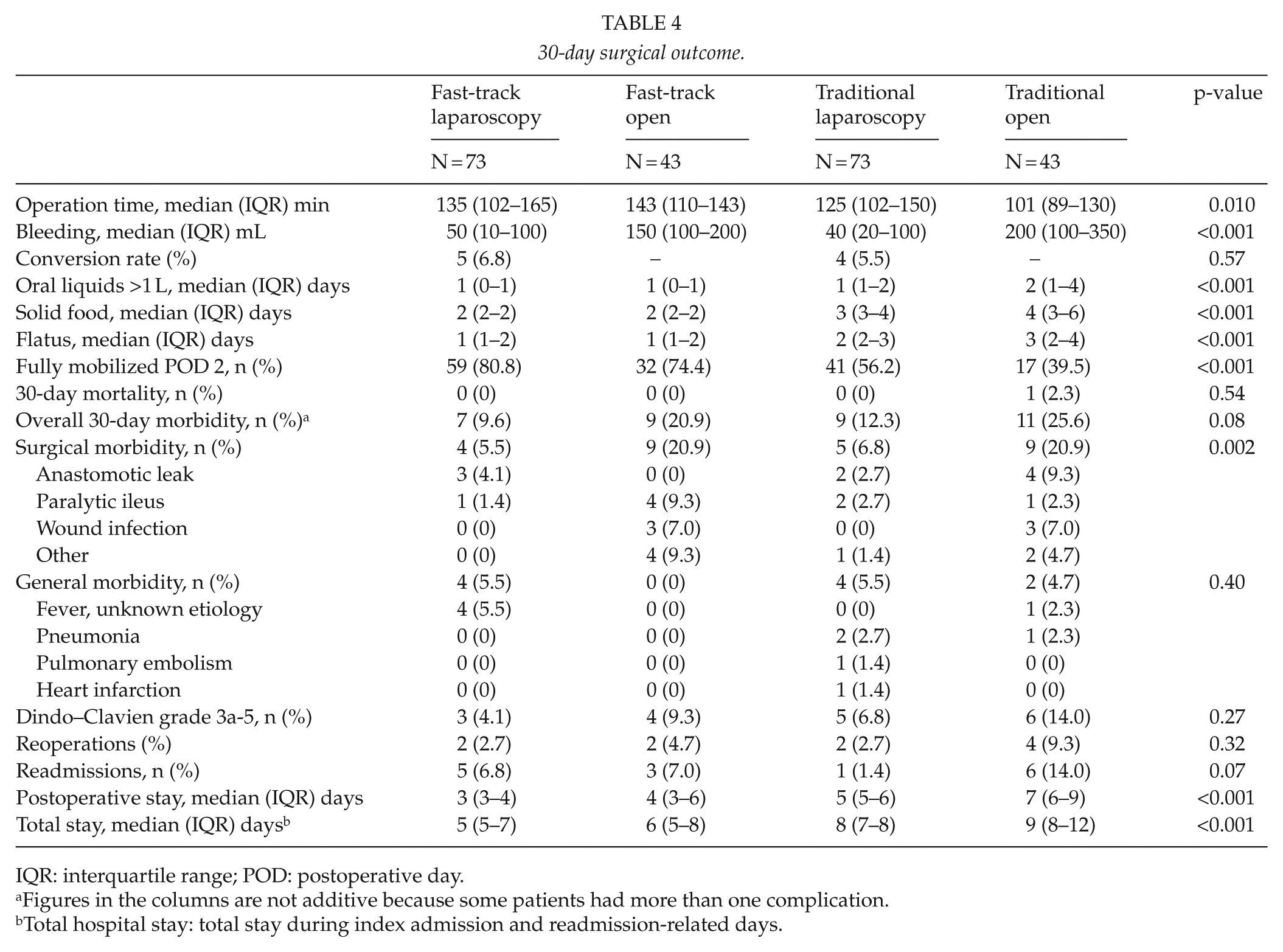
IQR: interquartile range; POD: postoperative day.
Figures in the columns are not additive because some patients had more than one complication.
Total hospital stay: total stay during index admission and readmission-related days.
Overall, there was a trend toward lower in-hospital costs in the fast-track group compared with the traditional care group (Fig. 1; Table 5). Open surgery within fast-track care was the least costly option compared to laparoscopic or open resection within traditional care but not significantly so when compared to laparoscopy within fast-track care. Preoperative costs between the study groups were similar because the fast-track group included only one extra additional preoperative visit for information and counseling. The per-patient operating room costs were higher in the laparoscopic than in the open surgery group mainly due to an increased use of disposable instruments (mean difference €678 (95% CI: €598–€722), p = 0.001). The per-patient postoperative expenses were lower in the laparoscopic than in the open group, the main reason being a shorter stay in the elective abdominal ward (mean difference €−922 (€−1576 to €−329), p = 0.0043).
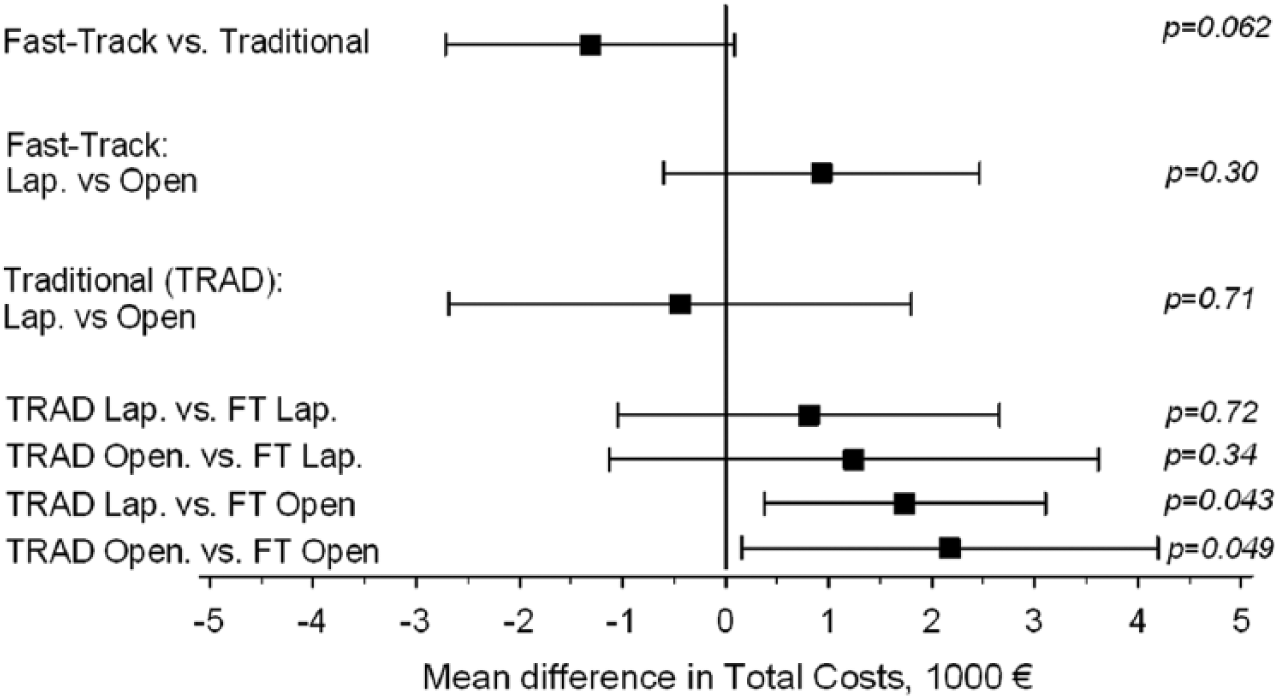
Mean (95% CI) differences in in-hospital costs according to treatment strategy.
Mean in-hospital costs (95% CI).
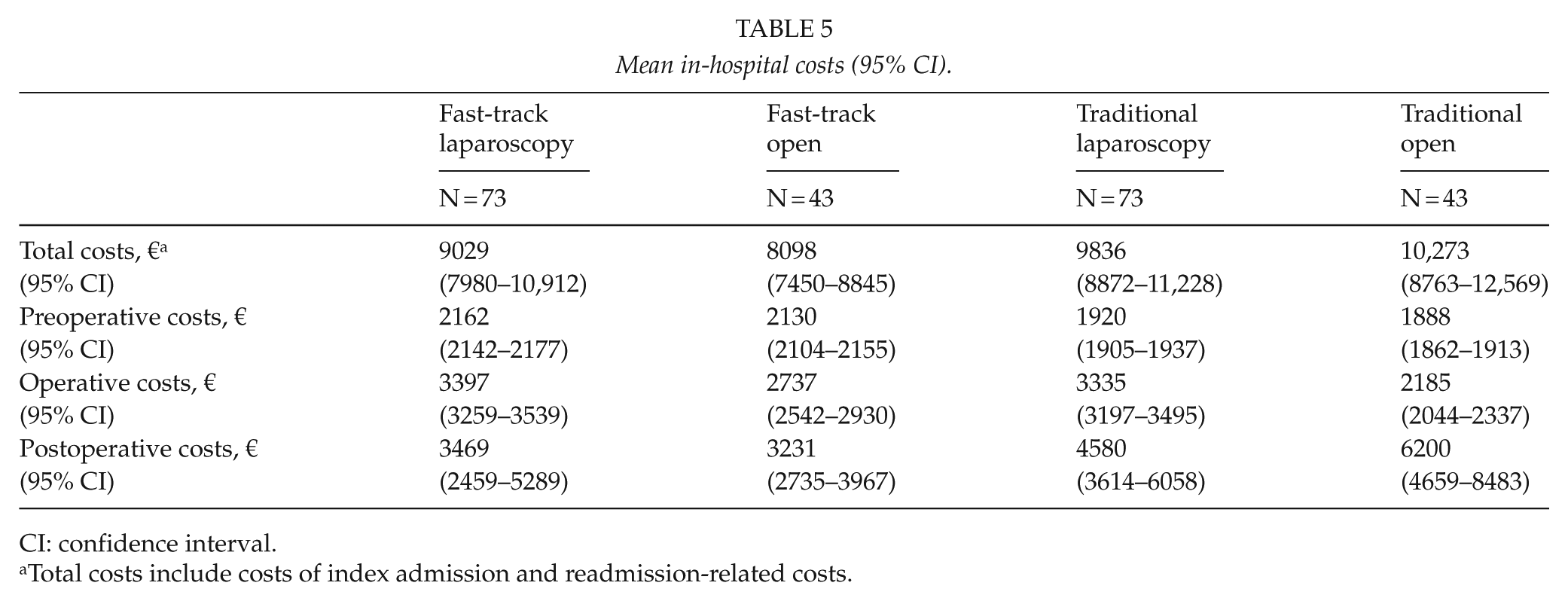
CI: confidence interval.
Total costs include costs of index admission and readmission-related costs.
Secondary Outcomes
Intake of solid food and bowel function recovered 1 day earlier in the fast-track than in the control group (p < 0.001) (Table 4). One patient in the standard group died of heart infarction and postoperative pneumonia. Overall 30-day morbidity was similar between the four study groups. However, complications were more frequent after open surgery than after laparoscopic surgery either within fast-track or traditional care (23.3% vs 11.0%, p = 0.012). Reoperation rates were similar between the study groups. After discharge from hospital, 8 patients (7.4%) in the fast-track group and 16 (13.8%) in the control group were sent to a general practitioner–guided nursing facility, whereas other patients went home. Readmission rates did not differ significantly between fast-track and traditional study groups.
Discussion
The role of laparoscopy in improving postoperative outcome within fast-track perioperative care pathway has been controversial, but a recent randomized study (16) and meta-analysis (2) concluded that laparoscopic colorectal surgery within fast-track multimodal management has shorter postoperative and overall hospital stay than open surgery within fast-track care. Here, while aiming at the rationalization of perioperative care in daily clinical practice, we show that laparoscopic colonic resection within fast-track perioperative care in comparison with traditional care pathway significantly reduced the LOS without compromising patient safety or increasing hospital costs, and could be done with a relatively high rate of protocol compliance. Fast-track care and laparoscopic surgery were independent determinants reducing the length of postoperative hospital stay, whereas complications adversely affected the length of postoperative hospital stay.
A recent randomized trial reported a shorter postoperative hospital stay after laparoscopic than open colonic surgery (5 vs 6 days) in the fast-track setting (16). In line with that, the postoperative hospital stay after colonic resections in our study was 3 days after laparoscopic and 4 days after open surgery within fast-track care compared to 5 and 7 days within traditional care. Although postoperative hospital stay of 2 days has been reported after fast-track colonic surgery, Andersen et al. (19) showed that the readmission rate was around 10% instead of 20% by planning discharge 3 days instead of 2 days after surgery within fast-track care. Accordingly, our readmission rate in the fast-track group was well below 10%. Overall, the development of complications had the strongest adverse impact on the length of postoperative stay. Efforts to improve the quality of care are therefore important.
From a health economics point of view, a systematic review of the costs of laparoscopic colorectal surgery within traditional perioperative care reported similar total costs for laparoscopic surgery than open surgery despite greater operating room costs (20). Previous meta-analyses of randomized trials comparing fast-track and traditional care pathways in colorectal surgery (1–3), and a recent systematic review (17) also tend to support the cost-effectiveness of enhanced recovery pathways for colorectal surgery as a result of shorter postoperative hospital stay and slightly reduced postoperative morbidity (1, 2). However, the quality of the current evidence is limited (17). A recent randomized trial showed no statistically significant differences in in-hospital costs between laparoscopic or open colonic resection within fast-track or traditional care (16). Another randomized study reported lower costs after open surgery within fast-track care than within traditional care (21). This study shows that despite a trend toward lower costs in the fast-track than in the traditional care group, the difference was not statistically significant. Open surgery within fast-track care was the least costly option compared to laparoscopic or open surgery within traditional care but not significantly so when compared with laparoscopy within fast-track care. Because laparoscopic colonic resection within fast-track care resulted in shorter hospital stay and lower complication rate than open surgery without significantly increasing in-hospital costs, the combination of laparoscopic surgery and fast-track care seems to be the optimal strategy for elective colonic surgery.
In our study, greater operating room costs in laparoscopic surgery were mainly due to the increased use of disposable instruments and partly counterbalanced by a shorter hospital stay. With respect to postoperative hospital costs, the main determinant increasing costs was the length of stay in the hospital. In multivariate analysis, postoperative complications were the major determinant prolonging the LOS.
It is well known that the clinical outcome and costs of colorectal surgery are dependent on surgeon’s experience and the quality of surgery. The safety of laparoscopic colonic surgery, in terms of short-term results, has been demonstrated in many randomized trials (13–15). Short-term outcomes in this study were comparable to those reported by other studies (13–15), suggesting that the quality of surgery in this cohort of patients was as good as elsewhere. A small proportion of patients developed complications increasing the length of postoperative hospital stay or led to reoperations, unplanned intensive care unit (ICU) admissions, or readmissions to hospital, thereby increasing in-hospital costs. Overall postoperative morbidity in our study was significantly lower in patients who underwent a laparoscopic colonic resection instead of open resection. This is in contrast to randomized trials which failed to demonstrate a decrease in morbidity after laparoscopic or open colonic surgery in the fast-track setting (16, 21).
A major challenge with this study was the lack of randomization which may have caused some selection bias. Historical controls operated on before the implementation of fast-track care were used for comparison to avoid the contamination of the traditional care elements with more modern fast-track elements if more recently operated patients were included. Capital costs of laparoscopic equipment were excluded because laparoscopic equipment is nowadays considered standard operating theater equipment. Moreover, in our hospital, laparoscopic equipment is used not only for colorectal surgery but also for many different kinds of procedures, including gallbladder and common bile duct stone removal; fundoplications; hernia surgery; colorectal, liver and pancreatic surgery; adrenal gland surgery; esophageal resections; thoracic surgery; and staging, making the capital costing very difficult. Another limitation was that the research was conducted in one hospital and included the learning curve when implementing the fast-track pathway. However, senior surgeons had a large experience in laparoscopic and open colorectal surgery. Also, the adherence with different fast-track elements was higher than usually reported.
Conclusion
Laparoscopic colonic resection within fast-track perioperative care is safe, improves postoperative recovery, is not significantly more costly than open surgery, and results in shorter hospital stay, thereby improving the efficiency of fast-track perioperative care.
Footnotes
Acknowledgements
This study was approved by the ethics committee of the hospital.
Declaration of Conflicting Interests
The authors have no conflicts of interest to declare.
Funding
This study was funded by the local EVO (Erityisvaltionosuus) funding of Central Hospital of Central Finland.