
Abstract
Background and Aims:
The death of any young individual is associated with the loss of many potentially fulfilling years of life. It has been suggested that the relative mortality of fracture patients may be higher in younger age groups than in older cohorts. We determined the mortality and causes of death in a cohort of 16- to 30-year-old patients that had been hospitalized for fractures.
Material and Methods:
We collected data using criteria based on the diagnosis code (International Statistical Classification of Diseases and Related Health Problems, 10th Revision), surgical procedure code (Nordic Medico-Statistical Committee), and seven additional characteristics of patients admitted to the trauma ward at the Central Finland Hospital between 2002 and 2008. Patients were then followed to ascertain their mortality status until the end of 2012. Standardized mortality ratios were calculated and causes of death were determined by combining our registry data with data provided by Statistics Finland.
Results:
During the study, 199 women and 525 men aged 16–30 years had sustained fractures. None of these patients died during the primary hospital stay. At the end of follow-up (mean duration 7.4 years), 6 women and 23 men had died. The standardized mortality ratio for all patients was 6.2 (95% Confidence Interval: 4.3–8.9). Suicides and intoxications comprised over half, and motor vehicle accidents and homicides comprised nearly a third of the post-fracture deaths.
Conclusion:
We found a concerning increase in mortality among young adults that had been hospitalized due to a fracture compared to the general population that had been standardized by age, sex, and calendar-period. Leading causes of death were suicides and intoxications or motor vehicle accidents and homicides, which may be indicative of depressive disorders or impulse control disorders, respectively. Identification of the underlying psychosocial problems may provide an opportunity for preventive interventions.
Introduction
Post-fracture mortality research has traditionally focused on older adults, particularly those with hip fractures, and most of these studies have not differentiated between in-patient and out-patient care (1–10). The death of a young individual leads to the loss of many years of a potentially productive and fulfilling life. Yet despite this, post-fracture mortality and causes of death among young adults are unknown. Some previous studies have suggested that the relative mortality after fractures in relatively young cohorts increased (11, 12). We have recently shown that after they had sustained upper extremity fractures, the relative mortality was the highest in patients below 30 years of age (13).
The aim of this study was to determine the mortality and causes of death among 16- to 30-year-old patients that had been hospitalized for fractures and thereby begin addressing the paucity of published data for this cohort. We examined hospital-based registry data and national mortality data, provided by Statistics Finland.
Materials and Methods
This study included all fracture patients between 16 and 30 years of age that had been admitted to the trauma ward of the Central Finland Hospital (CFH), Jyväskylä, Finland, between 2002 and 2008, which were subsequently followed until the end of 2012. The CFH is a public hospital that offers trauma treatment to a population of 250, 000, which represents approximately 5% of the population of the country. Patients living in the catchment area of the hospital district that had fractures requiring surgical treatment were referred to the CFH. These patients were hospitalized due to the severity of the fracture, or for other injuries associated with the fracture.
A hospital registry was maintained with records of the social security number, municipality, diagnosis (
The first sustained fracture was regarded as the index fracture. The mortality status of patients by the end of 2012 as well as the causes of death were acquired from the Statistics Finland database.
Statistics
The Cox proportional Hazards Model was used to estimate age- and sex-adjusted risk of mortality for each group. The Standardized mortality ratio (SMR), defined as the ratio between the observed and expected numbers of deaths, was calculated based on the subject-years method, with 95% confidence intervals (95% CI), and assuming a Poisson distribution. The expected number of deaths was calculated on the basis of sex-, age-, and calendar-period-specific mortality rates in the Finnish population.
Results
Of 5985 adult patients (45.2% men), a total of 724 patients (72.5% men) were aged 16 to 30 years and hospitalized for the treatment of a fracture in the CFH between 2002 and 2008. The mean age of these patients was 23.3 years (standard deviation (SD) ± 4.0). The five most common fracture sites were ankle, tibia, spine, forearm, and wrist (Fig. 1); 55 (7.6%) patients had multiple fractures. This cohort of young patients with fractures was followed for a total of 5310 person years (3842 for men and 1468 for women). The median follow-up time was 7.4 years (interquartile range (IQR): 5.7–9.0); (Fig. 1).
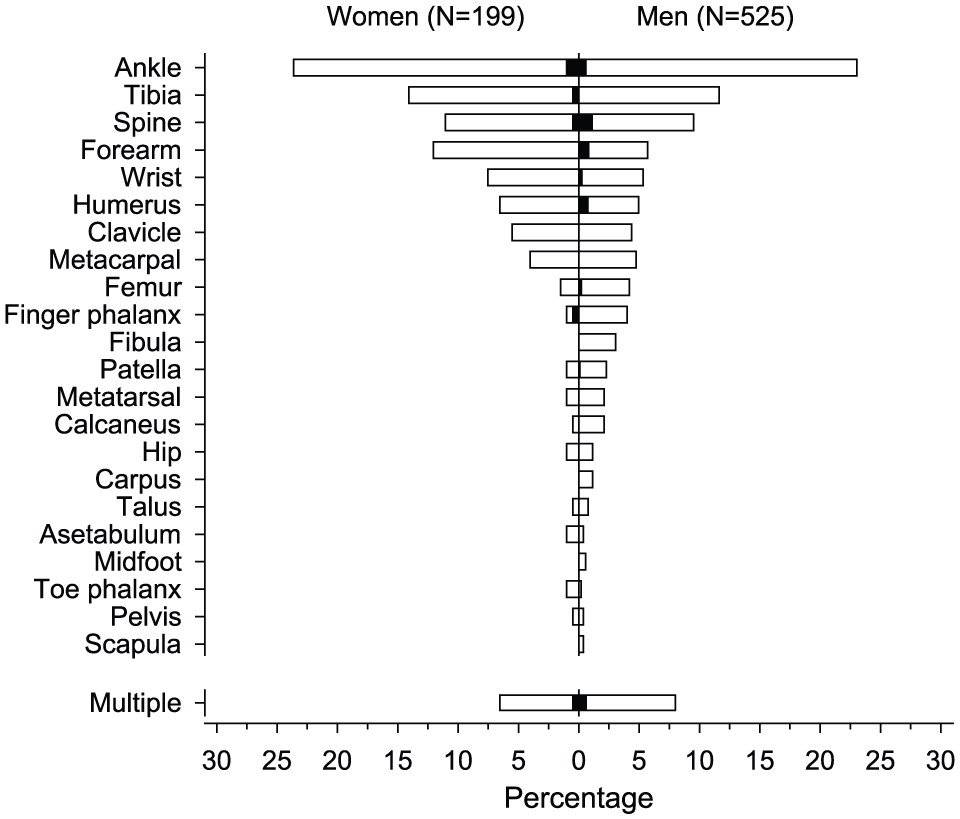
Distribution of different types of fractures (white boxes) and deaths (black boxes) among 724 adult patients (aged 16−30 years) with fractures.
Six women and 23 men of the 724 young patients with fracture had died by the end of the follow-up period. No patient died during the treatment period of the index fracture. Deaths did not accumulate for any particular fracture site (Fig. 1).
The cumulative mortality (Fig. 2), expressed as deaths per 1000 person years, was 4.1 (95% CI: 1.8–9.1) for women and 6.0 (95% CI: 4.0–9.0) for men. The age-adjusted hazard ratio (HR) of deaths between men and women was 1.46 (95% CI: 0.59–3.59), with no significant difference (p = 0.41). The age- and gender-adjusted HR for death associated with multiple fractures compared to death associated with a single fracture was 2.62 (95% CI: 1.01–6.86). The SMR of all patients was 6.17 (95% CI: 4·29–8.88). The corresponding SMRs for women and men were 11.16 (95% CI: 5.02–24.85) and 5.52 (95% CI: 3.67–8.31), respectively.
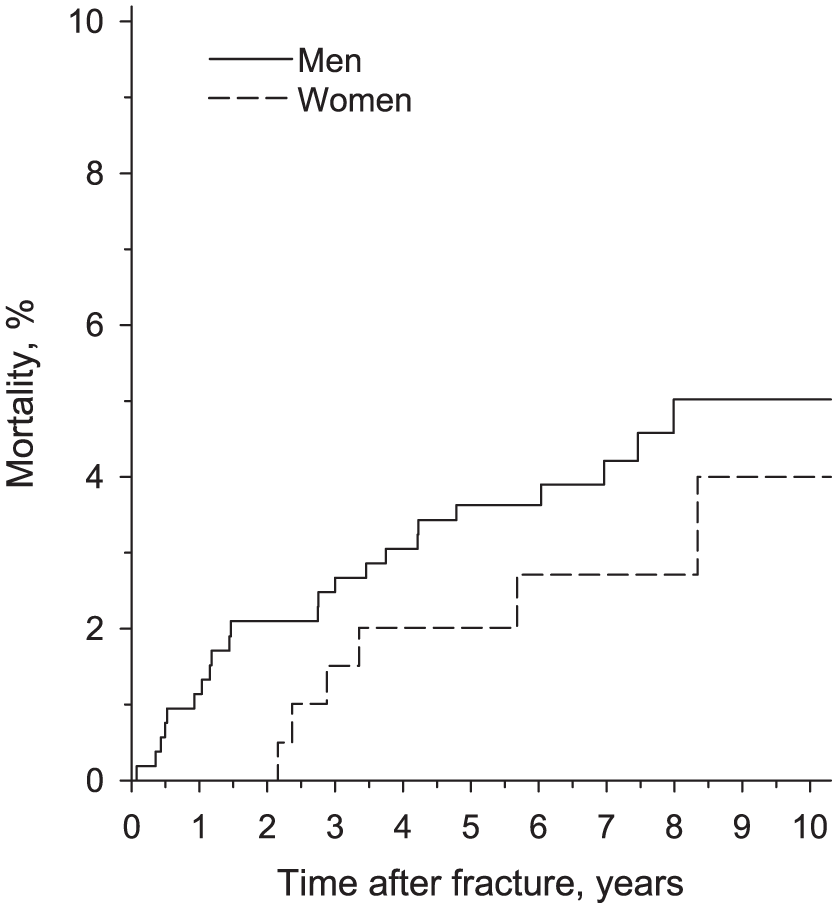
Post-fracture mortality among male (continuous line) and female patients (dashed line) with fractures, aged 16−30 years.
Suicide (28%) and intoxication (24%) were the leading primary causes of death. Motor vehicle accidents (MVAs) and homicides accounted for 17% and 10% of deaths, respectively. A mental or behavioral disorder (ICD-10 subgroup F) was listed as a contributing to the cause of death in 33% of deaths in women and 48% of deaths in men. One-fifth of the deaths were due to infections, neoplasms, or unknown causes. The time from fracture to death stratified by cause of death is shown in Fig. 3.
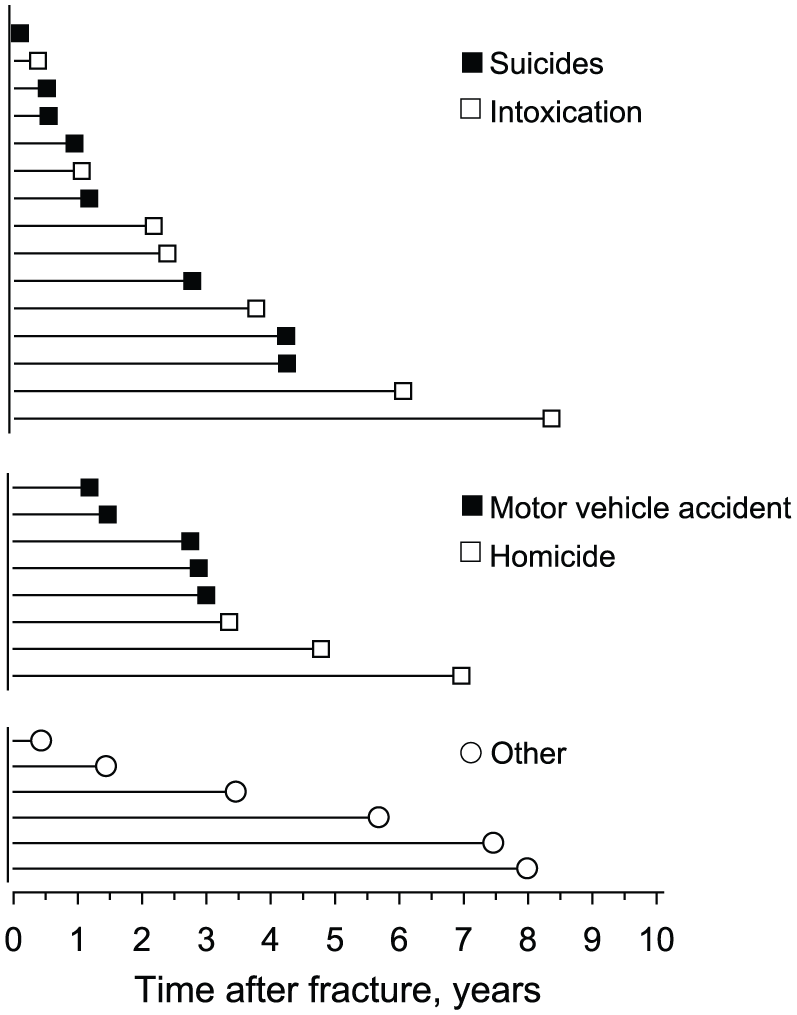
Causes of death over time, starting after the index fracture (t = 0). “Other” deaths were due to infections, neoplasms, or unknown causes of death.
Discussion
The novel finding in this study was that young adults who had been treated as inpatients for a fracture had a sixfold risk of death compared to the general population, when adjusted for age, sex, and calendar-period. Previous studies have suggested that relative death rates tended to increase in relatively young patients who had sustained fractures (11, 12). However, to our knowledge, this phenomenon has not been specifically investigated in a cohort of young adults with fractures that required hospitalization, until now.
The causes of death among young patients with fractures differed markedly from those among older patients. Over half the deaths in our cohort that followed in-patient fracture treatments were due to suicide or intoxication and nearly a third were due to MVAs and homicides. By comparison, it has been reported that cardiovascular diseases accounted for nearly half of the deaths in older age groups (13). The causes of death of young individuals in the general population in an earlier Finnish study are similar to those in our cohort (14).
Viilo et al. (15) reported that hospitalization-requiring injuries were common among young adults who later committed suicide and they found that 33% of young male and 44% of young female suicide victims had been hospitalized for an injury or for intoxication. Barak-Coen et al. (16) also identified sustained injuries as being a risk factor for suicide, although fractures were not separately addressed in that study. Furthermore, self-harm patients are subject to a 40-fold risk of suicide (17).
Poor socio-economic background seems to correlate with adverse health behavior, injuries, and accidents but not with mental illness or with suicide (14, 18). Injuries and fractures in young adults may be indicative of a risky lifestyle and early death. People that were intoxicated while sustaining an injury were shown to present with more serious injuries and longer hospital stays than patients that were not intoxicated (19). On the contrary, alcohol abuse can be a means for masking depression; particularly for men (20, 21). The data of this study show that 8/9 individuals that committed suicide were men.
We hypothesize that suicides and deaths due to intoxication may be associated with depressive disorders. In psychological autopsy studies, up to 90% of individuals that committed suicide were shown to have depression, either diagnosed or undiagnosed (22, 23). Furthermore, substance use disorders are commonly associated with depression (24). Deaths due to MVAs and homicides might be indicative of underlying impulse control disorders (25, 26). However, in this group of patients, depression and alcohol abuse are also commonly associated (27, 28).
Study Strengths and Limitations
All deaths in Finland are recorded by Statistics Finland. Cases with unclear death certificates are evaluated by a panel that consists of medical and nosological experts; therefore, the mortality statistics can be regarded as fairly accurate (29). A significant number of deceased patients had death certificates that listed a psychiatric disease as a contributing cause of death. In Finland, however, contributing diagnoses are optional; thus, we suspect that the actual number of contributing psychiatric diagnoses was higher than our results indicated.
CFH is the only public hospital that offers trauma care in its catchment area. The strength of our study was that we analyzed a representative sample of young fracture patients and the cohort was followed-up for over 5000 person years. However, deaths are relatively rare among young adults, and even in this high-risk group, only 29 persons died. A multicenter study would be required for investigating our results on a larger scale. It is possible that some patients with severe injuries may have died in the emergency or intensive care units and, thus, were not admitted to the ward. Furthermore, patients with cervical spine fractures or fractures associated with severe traumatic brain injury are transferred directly to university hospitals and were not captured by this analysis. Thus, our results most likely have underestimated the early mortality of young patients hospitalized for fractures.
Many patients that sustain trauma are under the influence of alcohol or other substances at the time of sustaining the injury (30). However, our registry did not include data on blood alcohol levels or the use of illicit drugs at the time the patients arrived at the emergency department. Therefore, we were unable to investigate the correlation between substance use and fractures in this study.
Conclusion
We observed a remarkably high relative mortality in young adults who had been treated for fractures as in-patients. Most deaths were due to suicide, intoxication, MVA, or homicide. The majority of deceased individuals were men. It is possible that the causes of death in the general young adult population are similar to that found in young fracture patients’ subgroup. It is unclear why the relative mortality of young fracture patients is six times higher than in the general young adult population. An underlying, undiagnosed, serious mental illness may have already been present in some young adults that had received in-patient fracture care. Health professionals should therefore consider the possibility of a severe, undiagnosed mental illness when treating young adults hospitalized for a fracture.
Footnotes
Acknowledgements
The authors would like to thank Hannu Kautiainen for his invaluable help during designing of the study as well as during analysis and interpretation of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
None of the patients included in the register used in this study were contacted during the study and therefore the need for approval by an Ethics Committee was waived.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Finnish Medical Association (Finska Läkaresällskapet) and the Perklén Foundation.