
Abstract
Introduction
Recently, the incidence of ductal carcinoma in situ (DCIS), a noninvasive breast malignancy, has increased. This has resulted in an increase in the incidence of breast-conserving surgery (BCS). Numerous studies have suggested that intraoperative frozen section analysis (IFSA) could reduce the rate of additional excisions required to obtain adequate resection margins. However, DCIS is a known risk factor for positive margin status during BCS. Furthermore, some authors have concluded that IFSA may not be reliable for the detection of DCIS.
Aim
The aim of this study was to evaluate the safety and efficacy of IFSA in patients with DCIS.
Methods
The operative and pathological reports of patients with DCIS, who underwent BCS at our institute between 2006 and 2015, were retrospectively reviewed. The results of IFSA and the pathological findings of final reanalyzed frozen tissue specimens were analyzed.
Results
In total, 25 patients were included in our analysis. None of the patients required additional operations. The correct diagnosis rate for IFSA was 89.6%, with a sensitivity and specificity of 60.0% and 95.8%, respectively.
Conclusion
IFSA could be beneficial for determining safety resection margins in patients with DCIS.
Introduction
Recently, breast-conserving surgery (BCS) has become the standard treatment for patients with early-stage breast cancer. One severe complication of BCS is ipsilateral breast cancer recurrence. Horiguchi et al 1 reported a positive microscopic surgical margin as a risk factor for local recurrence in the conserved breast. Therefore, the need for ensuring an adequate safety margin has surfaced as an important issue in BCS. Currently, there are at least three methods for intraoperative margin assessment, including gross examination after slicing the specimen, frozen section analysis, and imprint cytology. 2 These methods have significantly reduced the rate of additional operations.
In particular, many clinics use intraoperative frozen section analysis (IFSA) for ensuring adequate safety margins of resected specimens. IFSA is a relatively simple procedure with a high sensitivity and specificity. 2 IFSA can also be used as a planning strategy for the surgeon as to which direction requires a greater excision margin for safety by using the pathologist's report. However, the hospital has to employ the pathologist, the result is also at the discretion of the pathologist, and this step can add approximately 20–30 minutes to the operating time. Additionally, and perhaps most significantly, some authors 3 have concluded that IFSA may not be reliable for the detection of ductal carcinoma in situ (DCIS).
We aimed to evaluate the safety and efficacy of IFSA in patients with DCIS. To the best of our knowledge, we are the first to examine the relationship between IFSA and DCIS. Therefore, we believe that this study is of relevance.
Methods
Patient selection
A retrospective analysis of all patients with DCIS, who underwent BCS at Presbyterian Medical Center (Jeonju, South Korea) between 2006 and 2015, was performed. All participants have provided a written informed consent. This study was approved by the appropriate Ethical Review Board committee of our institution. Research was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
All patients for whom discharge and electronic medical records with the International Classification of Disease 19 codes (D05) used by the author's hospital were available were included. In total, 46 patients were diagnosed with DCIS during the study period. Of these, 21 patients were excluded. Nine patients who had undergone total mastectomy were excluded. These included four patients who wanted additional breast reconstructive surgery, two patients who had experienced no cosmetic benefit, one patient who did not want additional radiotherapy, one patient with diffused Paget's disease, and one patient with poor compliance (did not attend clinic regularly and whose family wanted a one-step treatment, because they had not believed her). The remaining 12 patients were excluded because preoperative diagnostic excisional biopsy results showed no signs of residual cancer.
In total, 25 patients were selected for analysis (Fig. 1 and Table 1).

Study flow chart.
Reasons for exclusion from study.

Surgical and pathological procedures
Margins were considered positive if the tumor extended to within 1 mm of the margin in resected specimens or contained within the margin of resected specimens.
Intraoperative evaluations were performed by the operating surgeon. The surgeon determined how close the tumor was to the resection margin by gross examination. If the surgeon determined that it looks safe from cancer, the specimen was tagged with its direction for ease of knowing by the surgeon and immediately sent to the pathologist, who prepared frozen sections from the cut end of the specimen. The pathologist checked the whole direction of the specimen. If the IFSA findings were positive for cancer, then the pathologist reported to the surgeon and the surgeon resected additional tissue from the residual breast. The specimen was immediately sent to the pathologist, and the process was repeated until a negative resection margin was obtained. Each operation was completed after a check was performed for the presence of cancer by IFSA. We counted each separate one frozen section as a single step.
After the operations were completed, the pathologist carefully reanalyzed all intraoperative frozen tissue sections and reported the final result. This process required a period of approximately three to five days. Permanent pathological result defined this final pathological report.
Statistical analyses
Clinical characteristics were summarized for the additional repeat excision and nonrepeat excision groups, including mean age, first presenting symptom at diagnosis, clinical symptoms upon physical examination, prior excisional biopsy experience, permanent pathological findings, and median follow-up duration. The two groups were compared using Student's t-tests and chi-squared tests.
We defined both positive IFSA result and positive pathologic result by the cancer cell presence or extension to within 1 mm from the margin of resected specimens, and negative IFSA results and permanent pathological results were defined by the cancer cell absence or extended to without 1 mm from the margin of resected specimens. The differences between the initial findings of IFSA during BCS and the permanent pathological findings of the pathologist were analyzed. Additionally, we determined the correct diagnosis rate according to the patients' symptoms at the initial clinical presentation, including microcalcification on mammography and palpable or nonpalpable masses on ultrasonography, and calculated for each individual clinical presenting symptom. Two-group comparisons were conducted using chi-squared tests.
The sensitivity, specificity, false-positive and false-negative rates, positive and negative predictive values, and correct diagnosis rate were calculated using standard methods for proportions and exact 95% confidence limits overall and for each individual characteristic. The reliability of the correct diagnosis rate was checked using the kappa index. All statistical analyses were conducted using Statistical Package for the Social Sciences for Windows, software version 20.0 (IBM Corp.). P < 0.05 was considered statistically significant.
Results
In total, 25 women with DCIS met the inclusion criteria and underwent BCS during the study period. A summary of the patients' characteristics is provided in Table 2. The mean age of the patients was 53.0 years. The mean age of the patients with positive IFSA findings was 37.7 years compared to 55.0 years for patients with negative IFSA findings, which was statistically significant (P = 0.027). The median follow-up duration was 31.8 months. None of the patients experienced recurrence during the follow-up period, although two patients (8.0%) were lost to follow-up and one patient (4.0%) died of other medical complications (Table 2). Most BCSs were performed within the last 12 months (Fig. 2). Consequently, longer follow-up durations may be necessary to draw meaningful conclusions.

Operation case numbers of each year. Most cases existed for the past one year. It means that follow-up periods are not enough.
Clinical features of patients with and without additional resection during breast-conserving surgery.

Clinical presentation: classify by first presenting symptom when patient diagnostic period
microcalcification on mammography, not microcalcification but mass on ultrasonography.
Physical examination
if physician can palpate by physical examination: defined palpable, if physician cannot palpate by physical examination: defined nonpalpable.
Two patients were lost to follow-up and one patient died of other medical complications.
Five patients (20.0%) had palpable cancer lesions. The remaining 20 patients (80.0%) had nonpalpable cancer lesions, probably because the lesions were too small or there was only microcalcification on mammography.
The first resection specimens of all 25 patients were checked using IFSA (Fig. 1). According to IFSA findings, 22 patients (88.0%) completed surgery after confirmation of negative resection margins. The remaining three patients (12.0%) who had positive IFSA findings required an additional repeat excision during operation. Following the second intraoperative excision, two patients completed surgery after confirmation of negative resection margins' results and one patient with IFSA detected cancer cells in the second repeat excision specimen margin. This patient required a third intraoperative repeat excision. This patient completed surgery after confirmation of negative resection margins' result after the third intraoperative excision.
In total, there were 29 frozen sections from the first, second, and third intraoperative excisions, which were used to predict safety margins.
One section exhibited a false-positive result and two sections exhibited a false-negative result. In the sections with a false-negative result, cancer cells were detected within 1 mm of the resected specimen margin, but not in the margin itself (Fig. 1). For this reason, none of the patients required delayed secondary operations for additional resections after the initial operation.
The sensitivity and specificity were 60.0% and 95.8%, respectively. The positive and negative predictive values were 25.0% and 92.0%, respectively. The correct diagnosis rate was 89.6% (kappa index, 0.606; P = 0.01). The sensitivity and specificity for mass lesions were 33.3% and 94.7%, respectively. Conversely, the sensitivity and specificity of microcalcification lesions were 100.0% and 100.0%, respectively.
In total, there were three patients who required repeat intraoperative excision. Two patients with nonpalpable mass lesions completed surgery after the second intraoperative repeat excision. However, one patient with nonpalpable and microcalcification lesion required third intraoperative repeat excision to achieve negative resection margin.
We analyzed the correct diagnostic rate according to the characteristics of cancer (ie, palpable versus nonpalpable and mass lesions versus microcalcification lesions). Palpable or nonpalpable masses (P = 0.557) and mass lesions or microcalcification lesions (P = 0.557) were not significantly associated with a correct diagnosis (Table 3).
Relationship between diagnosis correction and characteristics of cancer.

Physical examination
if physician can palpate by physical examination: defined palpable, if physician cannot palpate by physical examination: defined nonpalpable.
Clinical presentation: classify by first presenting symptom when patient diagnostic period
microcalcification on mammography.
Fisher's exact test: three cells (75%) have expected count less than 5. The minimum expected count is 0.72.
Table 4 reveals a high degree of concordance between IFSA results and permanent pathological results (odds ratio, 34.5; P = 0.01).
Relationship between result of frozen section analysis and result of final rechecked pathology.
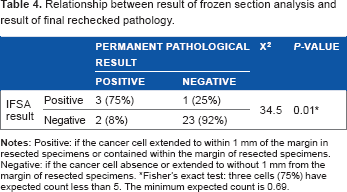
Fisher's exact test: three cells (75%) have expected count less than 5. The minimum expected count is 0.69
Discussion
A number of diagnostic tools have been developed to detect breast cancer at an early stage and small size. BCS can possibly follow this situation.
Clinicians often prefer to perform BCS to treat early-stage breast cancer because it can improve patient satisfaction levels and reduce complications associated with total mastectomy. Successful BCS requires adequate safety margins and the removal of minimal volumes for cosmetic purposes.
A number of methods for evaluating intraoperative resection margins have been investigated. The most representative methods include gross examination after slicing the specimen, frozen section for surgical margins, and imprint cytology.2,3 Recently, some authors 3 have reported on near-infrared fluorescence optical imaging, X-ray diffraction, high-frequency ultrasound, microcomputed tomography, and the margin probe system as methods for evaluating intraoperative resection margins. Gross evaluation is one of the most straightforward identification methods for palpable masses. 4 However, this method is limited by the presence of identifiable boundaries and, thus, may not be helpful for identifying nonpalpable masses, microcalcification lesions, and pre-excisional biopsy lesions.
Several studies2,5,6 of IFSA have reported that sensitivity and specificity rates range from 58.1% to 100.0% and 77.8% to 100.0%, respectively. The accuracy of IFSA has been reported to range from 83.0% to 98.0%.6–12 Many studies5,6,13 have demonstrated that IFSA reduces positive margin rates and additional excision rates from 27.0% to 9.8% and 27.0% to 6.0%, respectively. Recently, Osako et al 14 reported a study using entire circumferential IFSA. The authors concluded that this method could reduce the need for additional operations with improved clinical outcomes. Another study conducted by Ohno et al 15 used tangential IFSA, in which the method stated could aid in decision-making for selective part of re-excision. Therefore, many modified methods should be evaluated to determine the most effective approach. However, how effective IFSA is for patients with DCIS remains to be determined. Another study 16 has already reported that it is not easy to distinguish between patients with low-grade DCIS and typical ductal hyperplasia. Fukamachi et al 6 reported on the use of total circumferential IFSA and demonstrated that this method had significantly reduced the margin positive rate. However, DCIS is a risk factor for positive margin status during BCS, and these authors confirmed that their study showed similar findings.
Imprint cytology is another method that can be used to assess resection margins intraoperatively. Klimberg et al 17 reported sensitivity and specificity values for imprint cytology of 100.0% and 100.0%, respectively. A study by Esbona et al 5 demonstrated that using imprint cytology reduced additional excision rates from 26% to 4%. In addition, this method required a shorter evaluation time than IFSA. However, it has limited capabilities to distinguish between carcinomas in situ and invasive carcinomas. Imprint cytology is also difficult to implement when evaluating close margins. 2
Recently, there have been differing opinions concerning safety margins. In the BCS guidelines used in Japan, margins are defined as positive if cancer is confirmed within 5 mm. 6 However, many recent studies18,19 assert that margins resulting in no ink on the tumor are appropriate because radiotherapy can be used in combination with surgery.
In the present study, a positive margin was defined as the presence of cancer cells within 1 mm of the resected specimen. The correct diagnosis rate was 89.6%. The sensitivity and specificity were 100.0% and 95.8%, respectively. The positive and negative predictive values were 25.0% and 92.0%, respectively. However, none of the final excised specimens contained cancer cells. As a result, if we proceed with the definition that negative margins mean no ink on the tumor, then the correct diagnosis rate may be elevated up to approximately 100.0%.
This study has several limitations. First, the limited samples sizes that make it difficult to draw definitive conclusions. Only 3 of 25 patients (12.0%) had positive margins after the first resection. The majority of patients (n = 22; 88.0%) had negative margins after the first resection. Low-grade DCISs are localized, noninvasive, and much more likely to have negative resection margins. Therefore, the higher the correct diagnosis rate, which is probably a consequence of the more patients we have in first resection negative arm, the higher the accurate predictive rate. Due to the limited sample sizes, especially the small number of patients with positive resection margins, it is difficult to conclude that IFSA is beneficial for patients with DCIS. Second, none of the patients in this study had recurrence during follow-up, and many of the operations were performed in the last 12 months (Fig. 2). The majority of breast cancers relapse within five years of the initial treatment. However, some breast cancer subtypes relapse within 15 years of the initial treatment. Therefore, if we want to check for recurrence of breast cancer, we must do so within a 5- to 15-year window. This suggests that the follow-up durations were not long enough in the present study, and long-term results should be evaluated.
Conclusion
Although the efficacy of IFSA is controversial and we have included only a relatively small number of patients, our study has demonstrated that IFSA is a useful tool for ensuring adequate safety margins in patients with DCIS. Our study is also the first to examine the efficacy of IFSA for only patients with DCIS. Nevertheless, further large-scale studies are necessary to validate our findings. Many studies have recently investigated more effective methods for evaluating resection margins, including combination approaches and a modified IFSA, among other techniques, which should also be explored further.
Author Contributions
Conceived and designed the experiments: MJK, CSK, YSP, EHC, KDH. Analyzed the data: MJK. Wrote the first draft of the manuscript: MJK, CSK, YSP. Contributed to the writing of the manuscript: MJK, CSK, YSP. Agree with manuscript results and conclusions: MJK, CSK, YSP, EHC, KDH. Jointly developed the structure and arguments for the paper: MJK, CSK, YSP, EHC, KDH. Made critical revisions and approved final version: MJK, CSK. All authors reviewed and approved of the final manuscript.