
Abstract
Purpose:
The use of prophylactic antibiotics in the mesh repair of inguinal hernias remains controversial. The aim of this study was to determine the perception of surgeons about surgical site infection and how this affects their clinical practice.
Methods:
A SurveyMonkey of general surgeons and senior surgical trainees was conducted via the local trust network and the questionnaire was displayed on the website of the Association of Surgeons of Great Britain and Ireland and Association of Surgeons in Training.
Results:
Eighty-one responses were received from surgeons who perform an average of 75 hernia repairs per year – the majority by open technique. Thirty-six (44.4%) used routine antibiotic prophylaxis, 40 (49.4%) selectively, and five (6.2%) not at all as the five surgeons who did not use antibiotics perceived their surgical site infection rate to be <1% and have never removed an infected mesh from a hernia wound. There was no clear difference between those who use prophylactic antibiotics routinely or selectively as the experience of mesh explantation is similar (56% versus 55% had 2–10 meshes removed respectively). Seventy-seven (95%) of surgeons felt a new specific set of guidelines was required.
Conclusion:
This study highlights the fact that in the absence of clear guidelines, most surgeons base their use of prophylactic antibiotics on their perceived risk or experience of surgical site infection. There is a strong need for a new set of guidelines to address the use of prophylactic antibiotics in groin hernia surgery.
Introduction
Inguinal hernia repair is one of the most commonly performed procedures in the United Kingdom with approximately 71,000 primary and recurrent repairs being performed per year (1). Although considered a clean surgical procedure, meaning that prophylactic antibiotics are not usually indicated, the implantation of a mesh involves the introduction of a foreign body that might result in disastrous consequences in the face of infection. Surgical site infection (SSI) varies greatly following repair of inguinal hernias being reported in between 1% and 9% of cases (2). The use of prophylactic antibiotics in the mesh repair of inguinal hernias remains a disputed topic. A recent Cochrane meta-analysis of 17 randomized controlled trials (3) found a reduction in SSI rates with antibiotic prophylaxis; however, this was not considered to be significant enough to recommend its use. Another smaller meta-analysis from 2012 found a significantly reduced infection rate when prophylactic antibiotics were used (4). The debate is further confused by conflicting guidelines from important bodies. The National Institute of Clinical Excellence (NICE) recommends that prophylactic antibiotics should be used for clean procedures that involve the implantation of a foreign body (5). However, this is contrasted by the European Hernia Society who recommends that prophylactic antibiotics are currently not indicated for routine use during inguinal hernia repair (6). The aim of this study was to determine the perception of surgeons about SSI and how this affects their clinical practice with regard to use of prophylactic antibiotics in inguinal hernia repair.
Methods
An online SurveyMonkey was conducted of general surgeons and senior surgical trainees who perform inguinal hernia repairs. The questions involved in this survey can be found outlined in Appendix 1. The survey was distributed to clinicians through the local trust network and was displayed on the website of the ASGBI (Association of Surgeons of Great Britain and Ireland) and ASIT (Association of Surgeons in Training). The responses to this survey were analyzed.
Results
A total of 81 completed responses were received. A higher proportion of the surgeons surveyed were male (53/81, 65%). Responses were obtained from both consultants (54/81, 67%) and senior surgical trainees (27/81, 33%). The mean number of hernia repairs performed each year by each clinician was 75.4 (median = 60). In total, 53% of respondents (43/81) only performed open surgery while the remaining 47% (38/81) also performing different levels of laparoscopic surgery. The proportion of repairs performed laparoscopically is shown in Fig. 1.
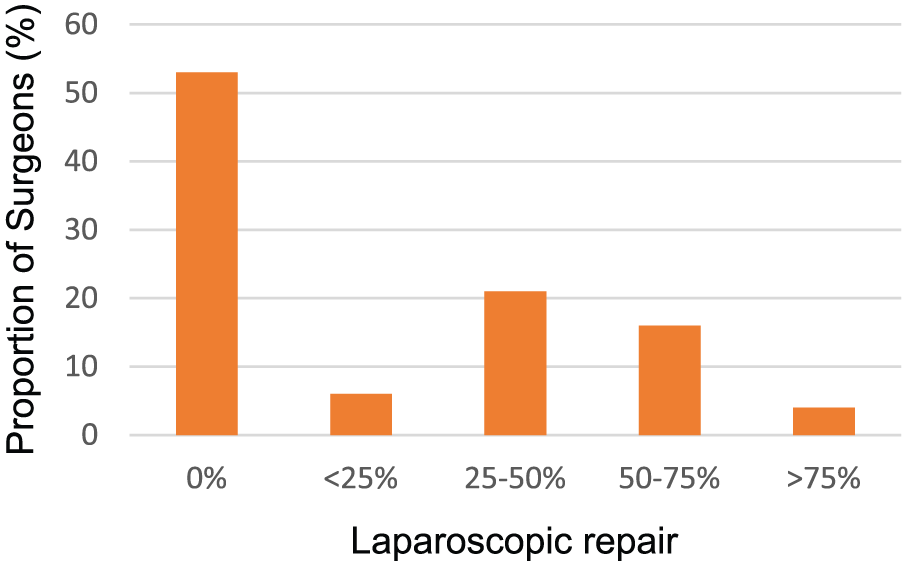
Relative proportion of laparoscopic repairs performed by responding surgeons.
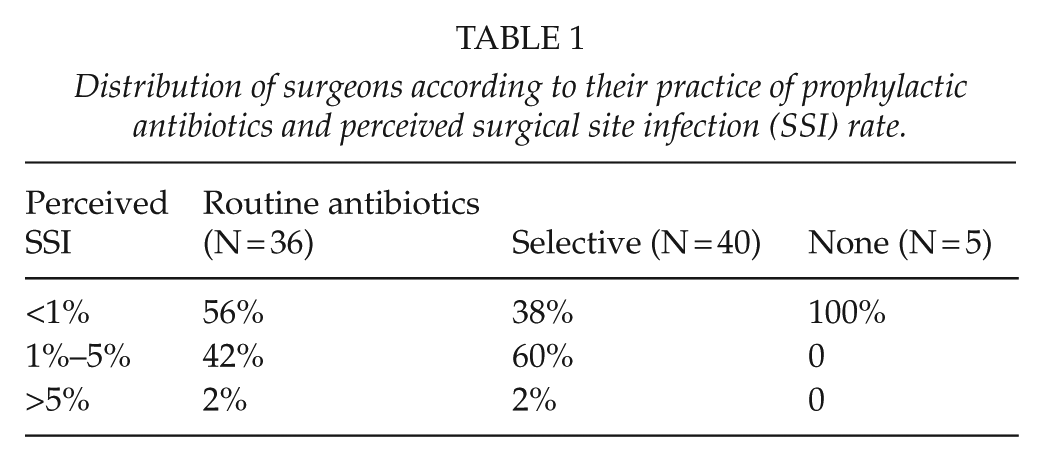
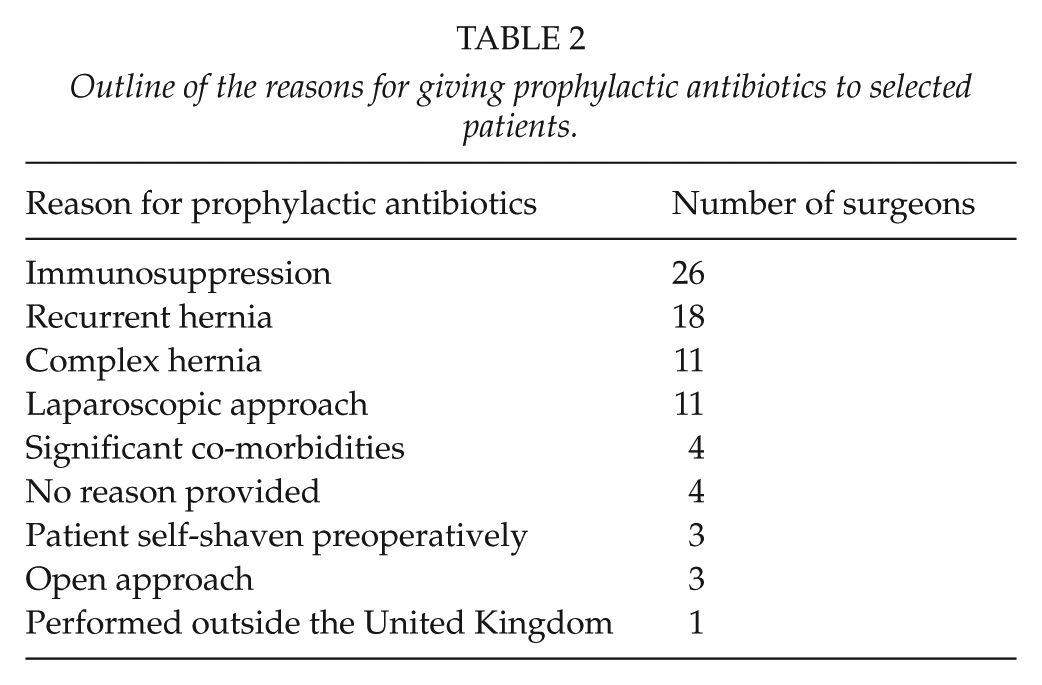
The distribution of respondents according to whether they offered prophylactic antibiotics to all patients, selected patients, or no patients is shown in Table 1. Surgeons who offered no antibiotic prophylaxis reported a perceived SSI rate of <1%. Sixty percent of surgeons (24/40) who practice selective use of antibiotic prophylaxis reported a perceived SSI rate of between 1% and 5%. For those who offer antibiotics to all patients, 56% (20/36) reported a mixed perceived SSI rate of <1% whereas 42% (15/36) had a perceived SSI of 1%–5%. The reasons given for selective use of antibiotic prophylaxis are shown in Table 2.
Distribution of surgeons according to their practice of prophylactic antibiotics and perceived surgical site infection (SSI) rate.
Outline of the reasons for giving prophylactic antibiotics to selected patients.
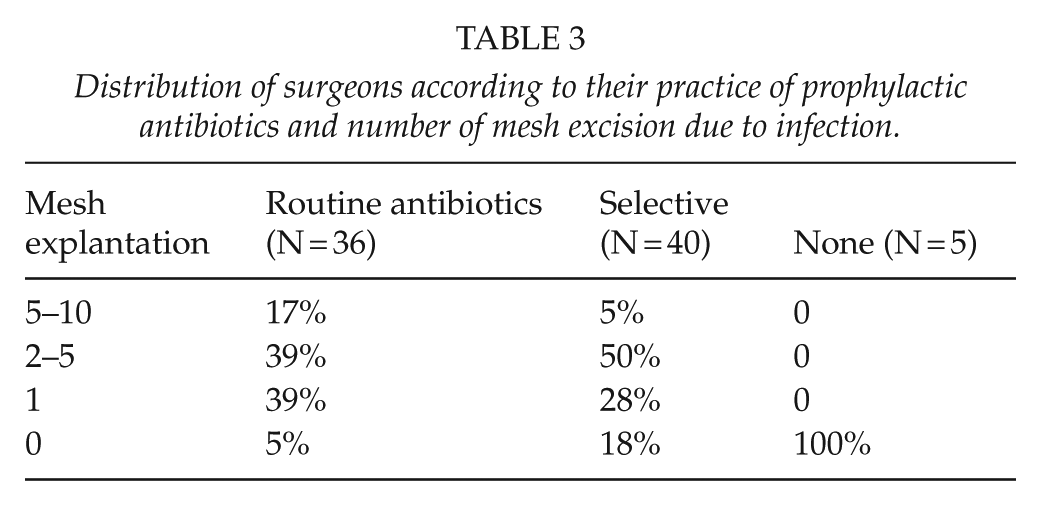
All surgeons who do not offer antibiotic prophylaxis to any patients have no experience of mesh explantation due to infection. The majority of surgeons (20/40, 50%) who offer antibiotic prophylaxis on a selective basis have experience of 2–5 mesh explantations during their surgical practice. A significantly greater proportion (7/36, 18%) of those who offer routine antibiotic prophylaxis to all patients have experience of >5 mesh explantations (Table 3).
Distribution of surgeons according to their practice of prophylactic antibiotics and number of mesh excision due to infection.
Only 37 (46%) surgeons stated that they were aware of existing guidelines. An overwhelming majority of 95% (77/81) of surgeons surveyed felt a new specific set of guidelines were required.
Discussion
The use of prophylactic antibiotics in groin hernia surgery remains controversial and the available guidelines (5–7) are often contradictory. The SIGN national clinical guidelines from 2008 provide information regarding the use requirement for prophylaxis prior to any surgery (7). They recommend that antibiotic prophylaxis is not required for open or laparoscopic hernia repair. The British Hernia Society (8), in collaboration with the Royal College of Surgeons and the European Hernia Society (6), recommend that although prophylactic antibiotics are not routinely required, they should be considered in “high risk” patients. The British Hernia Society defines high-risk patients as those with recurrent hernias or who are immunosuppressed. The European Hernia Society, however, uses the risk of wound infection or “surgical factors” to define patients at high risk. The most recent NICE guidelines (5) were constructed in 2008 on this matter and it has been recommended that in any clean surgery that involves the implantation of a foreign body, prophylactic antibiotics should be used.
This survey is limited by the relatively small number of responses received. However, the respondents are people with an interest in hernia surgery who appear to be performing significant numbers per annum. This survey clearly demonstrates that surgeons are pragmatic with the use of prophylactic antibiotics in inguinal hernia repair with 49.4% (40/81) using them on a selective basis (Table 3). The five (6.2%) surgeons who did not use antibiotics perceive their SSI rate to be <1% and have never removed an infected mesh from a hernia wound. As shown in Tables 1 and 3, there is no clear difference between those who use prophylactic antibiotics routinely or selectively. The experience of mesh explantation is similar in both groups – 56% versus 55% had 2–10 meshes removed, respectively. Similarly, only 2% in each group think that SSI rate following hernia repair is >5%.
The cost-effectiveness of prophylactic antibiotic use must also be taken into consideration. Estimations by Aufenacker et al. (9) place the current per patient cost of prophylaxis at £11.86, which is increased to a value between £237.20 and £1186 if considering a typical infection rate of 1%–5%.[TS: Please insert appropriate symbol for ‘£’ in all instances.] This is comparable to the £480.72 estimated cost of treating a SSI following inguinal hernia repair (10). Another key consideration that must be made is regarding the emergence of antibiotic resistance. With modern medicine striving to reduce the levels of unnecessary antibiotic prescribing, the use of antibiotic prophylaxis has been under increasing scrutiny. As a result of this, there must be a clear reason and relative risk reduction supporting their use. With the majority of hernia repairs being performed as day case procedures (11), this has led to many SSIs being reported in subsequent outpatient appointments or in General Practitioner clinics. This leads to an unknown level of antibiotic prescription that is not factored into analysis of antibiotic use. If a patient attends their General Practitioner clinic post operatively with a wound that is showing some signs of potential infection, antibiotics would commonly be prescribed so this additional practice must be considered (12).
The current guidelines are conflicting and do not provide clinicians with clear-cut guidance regarding the use of antibiotic prophylaxis. With 95% of clinicians in this survey agreeing that a new set of guidelines are required, this survey provides a strong impetus for such a development. As well as this, there are currently no specific national guidelines on the use of prophylactic antibiotics for elective laparoscopic cholecystectomy, which is an equally performed procedure in the United Kingdom, and surgeon opinion varies (13). This is another area that further research and guidance are required.
Conclusion
This study highlights the fact that in the absence of clear guidelines, most surgeons base their use of prophylactic antibiotics on their perceived risk or experience of SSI. There is a strong need for a new set of guidelines to address the use of prophylactic antibiotics in groin hernia surgery.
Footnotes
Appendix 1
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.