
Abstract
Background
Increased demand for arthroplasty also increases the number of complications of arthroplasty, especially surgical site infection (SSI). One of the effective strategies in preventing surgical site infection is the use of appropriate prophylactic antibiotics.
Objective
To identify and analyse information from clinical studies regarding factors affecting the effectiveness of prophylactic antibiotics in arthroplasty patients.
Methods
A scoping review was conducted through the PubMed, Scopus, and Google Scholar databases within a publication range from January 2004 to August 2020. Study data are extracted and analysed by a minimum of two reviewers.
Results
The search results found 2.419 articles, with 39 articles were included for further analysis. Cefazolin monotherapy was the most frequently studied antibiotic (15 articles) followed by vancomycin monotherapy (8 articles). Most widely used antibiotics in arthroplasty were cefazolin mono-therapy (997.599 procedures with SSI incidence range: 0,20–16,05%) followed by vancomycin mono-therapy (125.170 procedures with SSI incidence range: 0.27–3,88%) The correct antibiotic dose has a lower percentage of the SSI than the wrong antibiotic dose. Meanwhile, administration of antibiotics within single dose or <24 h had a lower SSI percentage than administration of antibiotics >24 h. Administration antibiotics before incision also have a lower SSI percentage than after incision. There were no studies that discussed re-dosing of antibiotics in this scoping review.
Conclusions
There is still a need for further research related to the duration and specific timing of first dose of prophylactic antibiotics, especially regarding single dose or multiple dose antibiotics to obtain maximum effectiveness of antibiotic prophylaxis
Introduction
Osteoarthritis patients are increasing every year. This is due to an increase in factors that can increase the number of osteoarthritis (OA) such as obesity, population aging, and an increase in the number of sports-related injuries. 1 Several studies predict that 67 million adults will be diagnosed with osteoarthritis by 2030, with 25 million people experiencing activity limitations due to arthritis. 2 Along with the increase in the number of people with osteoarthritis, the demand for arthroplasty has also increased dramatically. Research from the UK, Canada, Sweden, New Zealand, and Denmark has also predicted an increase in joint replacement surgery over the next two decades, although the estimation is varied widely. 1
Given the increasing number of joint arthroplasties performed each year, the number of arthroplasty complications has also increased. Surgical Site Infection (SSI) is one of the complications that is quite dangerous. Surgical Site Infection (SSI) in orthopaedic surgery cases prolong hospital stays from 12 to more than 20 days (about double the length of hospitalization in general) and increase health care costs by more than 300%. Patients with orthopaedic surgical site infections are also constrained by greater physical limitations which result in a decrease in the patient's quality of life 3
One strategy that has been shown to be effective in preventing and controlling surgical site infections is the use of prophylactic antibiotics. In general, prophylactic antibiotics will be effective in preventing surgical site infections if the antibiotics used are sensitive to potentially contaminating microorganisms and are able to maintain high levels of concentration during the surgical procedure. This can be achieved if prophylactic antibiotics can meet the four principles of prophylactic use of antibiotics, namely: the appropriate dose of prophylactic antibiotics, timely administration of the first dose of prophylactic antibiotics, repeated doses of prophylactic antibiotics under appropriate conditions, and the appropriate duration of prophylactic antibiotics.4,5
ASHP/IDSA/SHEA recommends cefazolin as a prophylactic antibiotic in patients with total joint atrophy. Clindamycin is also considered adequate alternatives if the patient is allergic to beta-lactam antibiotics. Vancomycin also can be used as an alternative agent for prophylactic antibiotics in health facilities with a high prevalence of MRSA (Methicillin-Resistant Staphylococcus Aureus) and for patients with known MRSA colonization. 4
The ASHP/IDSA/SHEA recommended dose of cefazolin is two grams. This recommendation was also followed by the Guidelines for the Use of Antibiotics at RSUD Dr Soetomo with the provision of giving cefazolin 1-2 grams iv drip for 15 min. If cefazolin is contraindicated, vancomycin may be given at a dose of 1 g every 12 h (∼30 mg/kg/day). The dose will certainly be different in patients with obesity conditions. 4 Some surgeons are unaware of changing the dose of cefazolin in this condition. This results in less cefazolin levels in the blood so that the protective effect against surgical site infections is not optimal. A retrospective study showed that cefazolin underdose was common, especially in obese patients. 6
The timing of the first dose of antibiotics is also one of the factors that affect the effectiveness of prophylactic antibiotics. The timing of the first dose of prophylactic antibiotics from various scientific literatures shows a variety of time options, namely: less than 30 min before surgery, 30–60 min before surgery, or 60–120 min before surgery. ASHP/IDSA/SHEA recommends administering prophylactic antibiotics within 60 min prior to incision, but there is also conflicting scientific evidence and the possible benefit of administering prophylactic antibiotics as close to the time of incision as possible. 4
Redosing of prophylactic antibiotics, especially in long-term surgery, is one of the important factors to maintain prophylactic antibiotic levels in blood and tissues. Intraoperative antibiotic redosing is necessary to ensure adequate serum and tissue antimicrobial concentrations if the duration of the procedure exceeds twice the antimicrobial half-life or there is massive blood loss (> 1500 mL). 4 Failure to re-dosing antibiotics, especially long-duration surgery, increases the risk of surgical site infection. 7
Based on the description above, there are several studies related to the use of prophylactic antibiotics with different research results. Therefore, it is necessary to conduct a literature review to summarize and present the information and results obtained from these studies. Therefore, this study tries to conduct a literature review in the form of a scoping review.
Materials and methods
This scoping review seeks to explore comorbid conditions that are at risk for surgical site infection in arthroplasty surgery and the factors that influence the effectiveness of prophylactic antibiotics in arthroplasty surgery. There are four stages of scoping review, 8 namely:
Identify questions
What are the clinical studies related to the use of prophylactic antibiotics in arthroplasty patients?
What is the condition of patients who are at risk for surgical site infections during arthroplasty?
How is the effect of the time of first administration of prophylactic antibiotics, dose of prophylactic antibiotics, re-dosing of prophylactic antibiotics, and duration of prophylactic antibiotics on the incidence of surgical site infection in arthroplasty patients?
Inclusion and exclusion criteria
The inclusion criteria for this review were: research articles in English or Indonesian, research conducted in the form of quantitative and qualitative research (RCT (Randomized Controlled Trial), cohort, case control, cross sectional, case report), and research subjects aged 18 years. Meanwhile, the exclusion criteria for this review were studies that discussed the use of antiseptics, local antibiotics, and postoperative antibiotic management, arthroplasty revision surgery, as well as research in the form of literature review and narrative review.
Selection of scientific article database and search strategy
Search was done through the PubMed, Scopus, and Google Scholar databases with publications ranging from 2004 to August 2020. This review used the keyword “surgical antimicrobial prophylaxis arthroplasty”
Data collection from selected studies
The selected research data were collected in the form of a table containing the research number, author, year and place of research, research objectives, number of samples, study design, inclusion/exclusion criteria, interventions performed, comparisons/controls used (if any), and main research data obtained from the study (SSI events and/or other outcomes assessed from the study). Data extraction was carried out by at least two researchers to reduce bias.
Analysis evidence and presentation of the results
A description of the data was carried out based on the year of study, study design, type of arthroplasty procedure, gender, SSI risk factors, type of SSI, and antibiotics used.
Each antibiotic group was then analysed descriptively based on the intervention group (dose of antibiotics used, time of administration of the first dose of antibiotics, re-dosing of antibiotics, and duration of antibiotics) associated with the incidence of SSI that occurred in each related study.
The results of the descriptive analysis of each antibiotic group are then made in the form of a table containing the antibiotic group, number of the article, the interventions carried out, the number of SSI, the number of arthroplasty procedures, and the incidence of SSI that occurred.
Result
An electronic literature search using the PubMed, Scopus, and Google Scholar databases yielded 2419 articles. After checking for duplication and reviewing the contents of the articles, 39 articles were obtained for further analysis6,9–46 (list of selected articles can be found in supplementary). Figure 1s
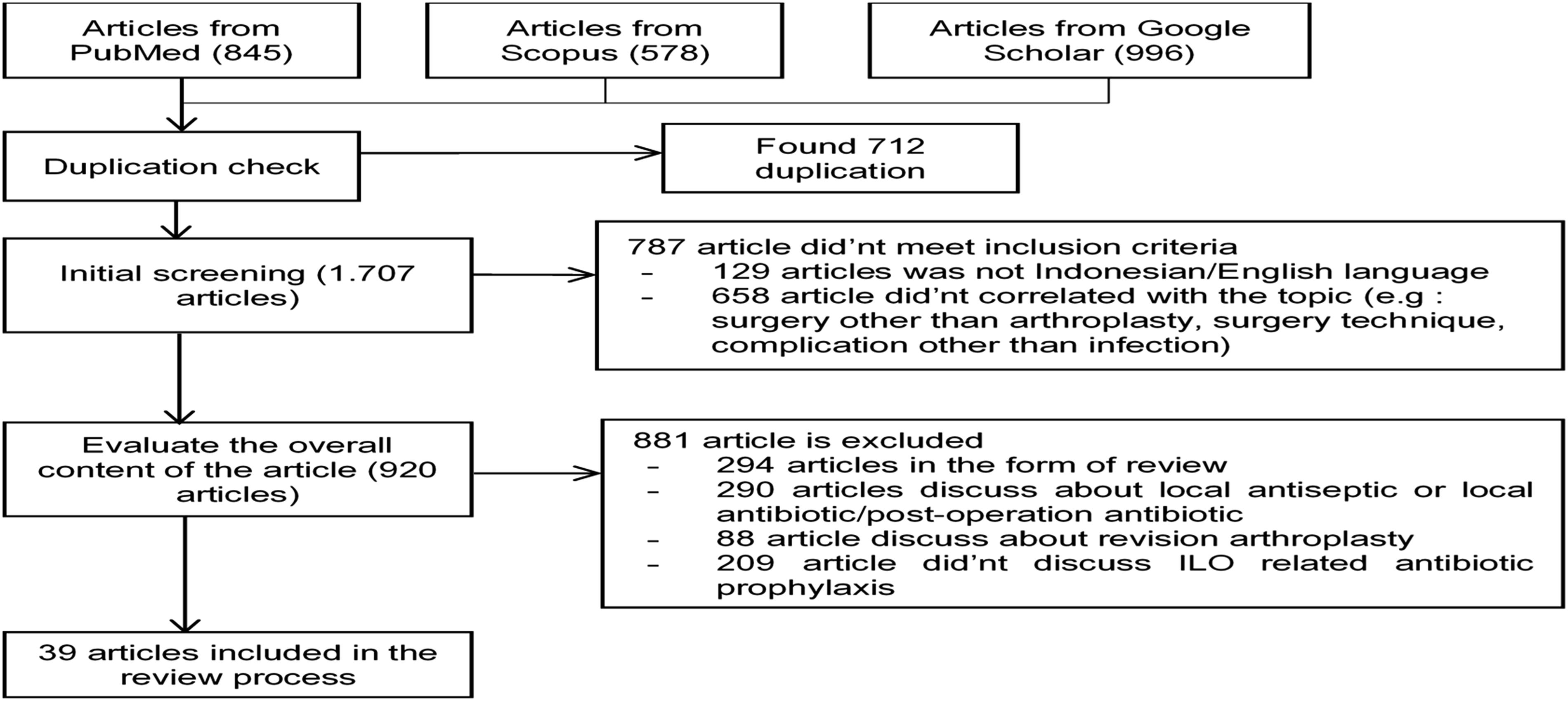
PRISMA diagram.
Study time
All selected article were generally conducted in 2003–2014. One of the reasons for the large number of studies related to prophylactic antibiotics in that year was the significant increase in MRSA cases. A study in the United States stated that S. aureus infections in hospitals increased by 42% and MRSA infections increased by 81% since 2000 with S. aureus contributing to 45.9% of all isolates of patients with skin and soft tissue infection and MRSA contributing to approximately 30% of S. aureus infections in hospitals. 47 These conditions encourage research to determine the effectiveness of the use of prophylactic antibiotics in surgical procedures, especially in operations with a risk of severe infection such as arthroplasty.
Study design
More than 80% (34 articles) of the studies were cohorts, while other studies were RCTs and case controls. RCTs are the golden standard for assessing the benefit of treatment. However, lower-level evidence can be used only if there are no good randomized controlled trials to answer a particular clinical question. High-quality observational studies can be used because they extend the evidence to a wider population and tend to predominate in hazard identification. In addition, observational studies can also be used when randomized controlled trials are unethical or impractical. 48 SSI study is generally conducted in the form of a retrospective cohort because SSI observations take a long time and the number of SSI events is small.
Types of arthroplasty procedures
Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) are the two most common types of arthroplasties in this scoping review. Meanwhile, studies related to other arthroplasty procedures, such as Unicompartmental Knee Arthroplasty (UKA) or Hemiarthroplasty, have only studied less than five studies. One of the reasons for the large number of studies related to total joint arthroplasty is the large number of these procedures performed around the world. Many factors have been reported or may be the cause of the increase in joint arthroplasty, including: aging population, increasing obesity worldwide, increasing prevalence of osteoarthritis, significant benefits of arthroplasty in improving the quality of life and joint function of patients, expansion of surgical indications, and patient behaviour. 49
SSI type
All studies show that superficial SSI is the most common SSI. This may be due to superficial SSI occurring in the skin or subcutaneous tissue which is in frequent contact with the external environment, thereby facilitating contamination. Superficial SSI accounts for more than 50% of SSIs for all categories of surgery.
SSI risk factors: comorbid conditions
Comorbid diseases that are often experienced by patients with arthroplasty surgery are diabetes and rheumatoid arthritis (RA). Six of eight studies examining the association of DM with SSI showed that the percentage of SSI in DM patients was higher than in patients without DM. However, almost all studies that have included SSI risk factors in this scoping review stated that diabetes did not have a statistically significant relationship with the incidence of SSI (p > 0.05). The same condition also occurs in RA patients. Several conditions that caused this result to differ from the results of previous studies, among others, were the diverse research conditions and the insufficient number of samples in both the SSI and non-SSI groups.
The American Diabetes Association defines uncontrolled diabetes if the HbA1c level is 8%. Using this threshold, studies have shown a higher incidence of postoperative surgical site infection in cardiac and orthopaedic patients who have HbA1C levels 8%.5,50 In addition, rheumatoid arthritis (RA) patients also have a higher initial risk for infectious disease compared to the general patient population which may result in higher infection rates, although published data do not consistently support this condition. The use of immunosuppressive drugs (glucocorticoids, cytostatics, interferons, and tumour necrosis factor inhibitors) in RA patients is considered to be one of the causes of the increased risk of SSI.51,52
SSI risk factors: gender
7 out of 10 studies examining the association of sex with SSI showed that male patients had a higher percentage of the incidence of SSI than female patients. Male patients have an SSI incidence range of 0.8%–23.5%, while female patients have an SSI incidence range of 0.4% - 14.1%. Langelotz, et. al., in his study with 438,050 patients, stated that men experienced SSI more often than women (p < 0.001). 53 Aghdassi, et. al. also tried to examine the relationship between sex and the incidence of SSI using a larger sample of 1,266,782 patients. The same results were also obtained with men experiencing more frequent SSI events than women. However, there are differences between this study and previous studies. Aghdassi, et. al. explained that the results of the analysis of the incidence of SSI in orthopaedic and traumatological procedures showed that men experienced SSI more often with one exception in the condition of the hip prosthesis due to fracture which showed no significant difference between men and women. 54
SSI risk factors: obesity
The condition of the patient's weight is also one of the risk factors associated with the incidence of SSI, especially in obese patients. Six of seven studies showed that obese patients had a higher incidence of SSI incidence than non-obese patients. Obese patients have an SSI percentage range of 1.3%–3.8%. A meta-analysis study showed that obese patients undergoing orthopaedic surgery were twice as likely to develop SSI. The cause of obesity as one of the risk factors for SSI is multifactorial. Obese surgical patients have a reduced oxygen supply to the subcutaneous tissue and require more inspired oxygen to achieve the same arterial oxygen pressure as normal weight patients, thus predisposing to SSI. 55 In addition, excess adipose tissue can increase the risk of inflammation and reduce the immune response so that it is more susceptible to infection. 56
Prophylactic antibiotics used in selected studies
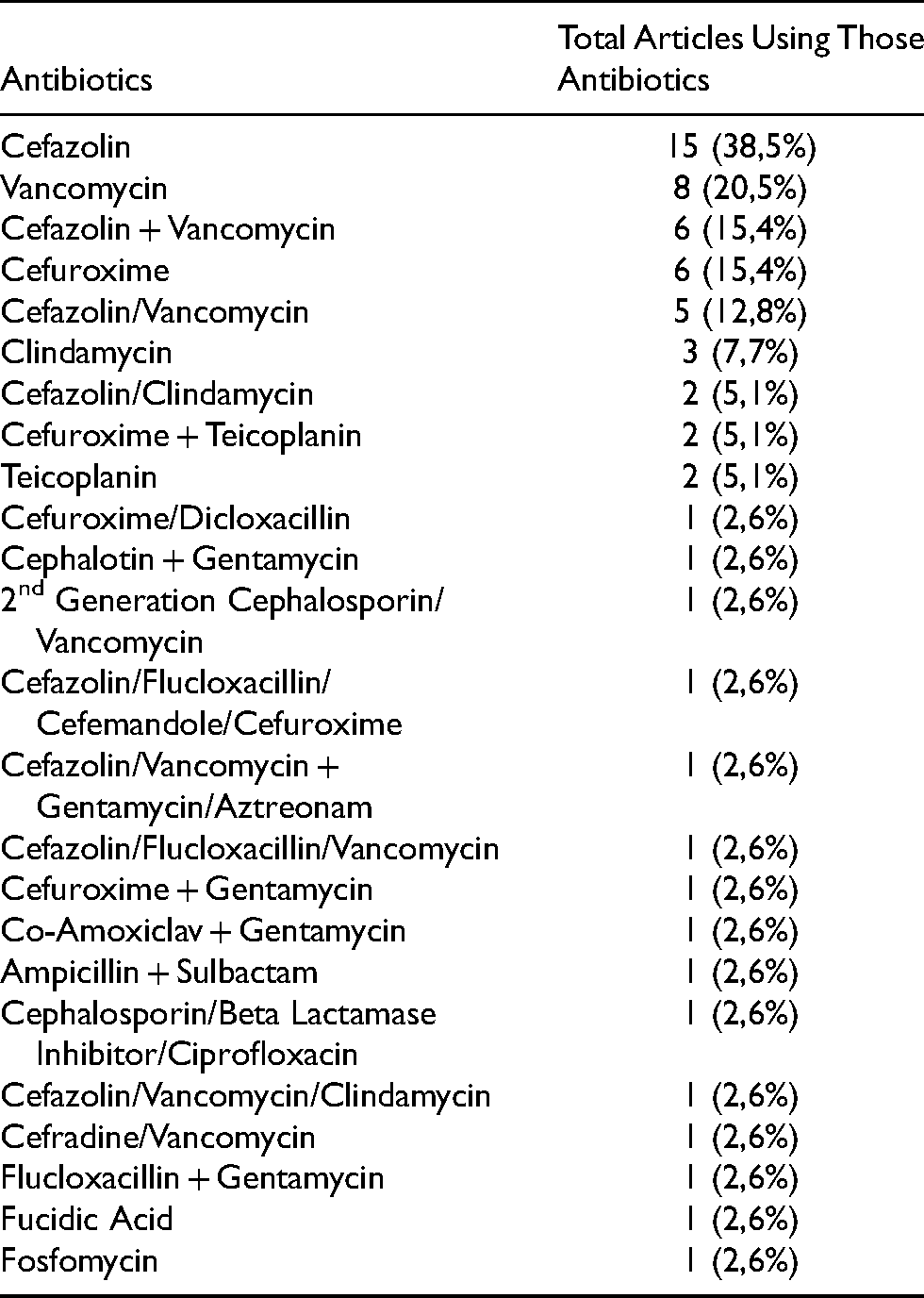
Only six types of antibiotic combinations with the percentage of use in the selected study above five percent, namely cefazolin (38.5%), vancomycin (20.5%), the combination of cefazolin and vancomycin (15.4%), cefuroxime (15.4%), cefazolin/vancomycin (12.8%), and clindamycin (7.7%) Table 1.
Antibiotics used in selected articles.
Cefazolin is a first-generation cephalosporin that is often used as a prophylactic antibiotic in joint replacement. Cefazolin has a spectrum of activity against organisms commonly encountered in surgery, is safe, and has low cost. 4 Cefazolin is very active against gram-positive bacteria and less active against gram-negative microorganisms.
Cefazolin has a longer half-life (± 2–3 h) and greater protein binding (± 80%) compared to other first-generation cephalosporin antibiotics so that cefazolin has high blood levels. 57 Cefazolin has the highest peak bone concentration of all first-generation cephalosporins. Cefazolin reaches peak concentrations within 40 min after parenteral administration with a serum half-life of 108 min and a bone half-life of 42 min. 58 The concentration of cefazolin in bone also exceeds the MIC90 of Staphylococci. 59
Percentage of SSI incidence between prophylactic antibiotic regimens
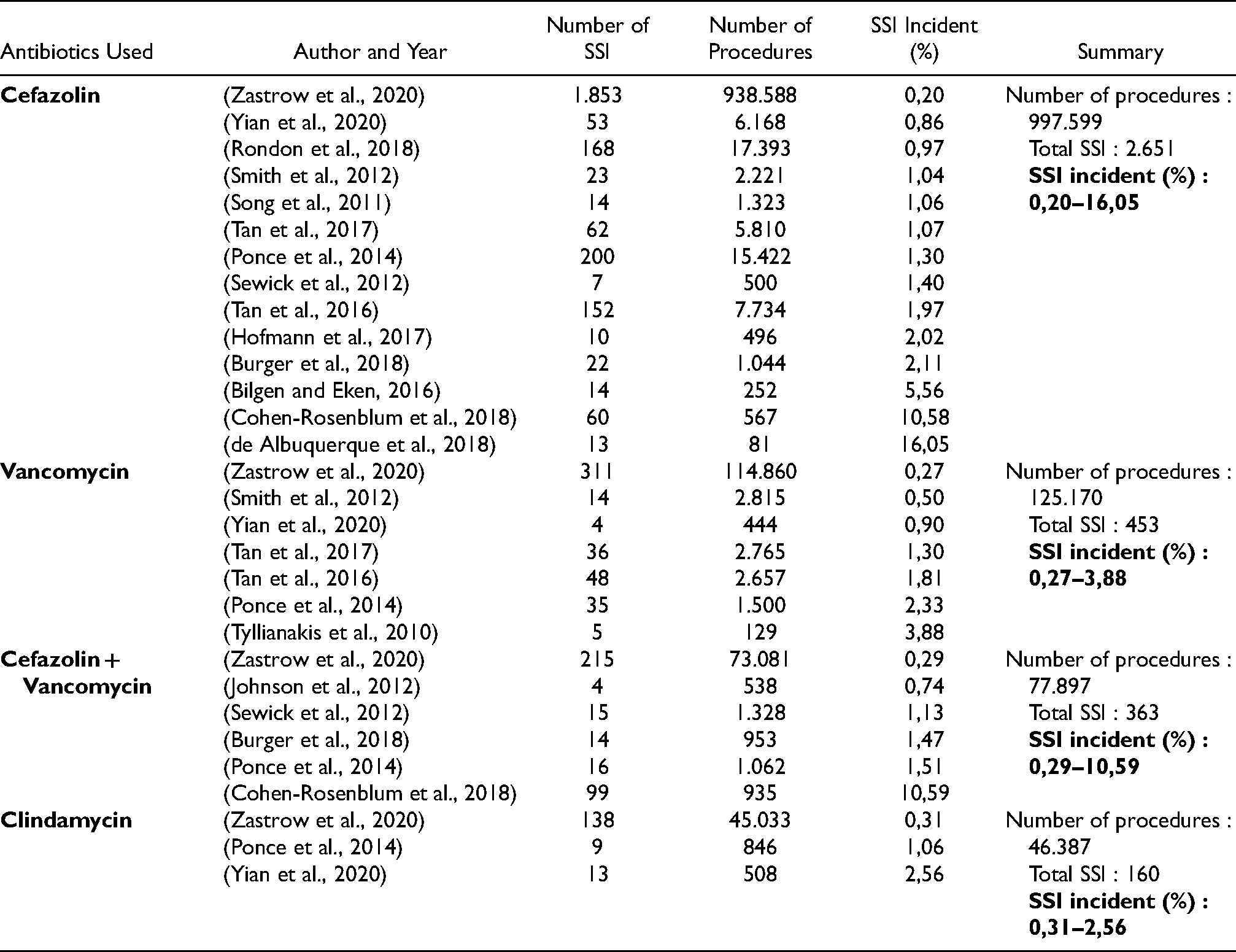
Of the 24 antibiotic regimens identified in this scoping review, only 4 were used in more than 10,000 arthroplasty procedures. The four antibiotics were cefazolin, vancomycin, cefazolin + vancomycin, and clindamycin. Table 2
Prophylactic antibiotic that used more than 10,000 arthroplasty procedures.
Cefazolin is the main prophylactic antibiotic for arthroplasty, so it is often studied and used as a comparison to other prophylactic antibiotics. Several studies in this scoping review tried to compare several prophylactic antibiotics with the standard antibiotic cefazolin. Study from Yian et. al. with 7140 patients that examined clindamycin in patients with total shoulder arthroplasty stated that there was a significantly higher risk of SSI with the prophylactic IV antibiotic clindamycin compared to the prophylactic IV antibiotic cefazolin. The overall risk of infection was 3.5 times higher when IV clindamycin was used compared with IV cefazolin (HR = 3.45, 95% CI 1.84–6.47, P = 0.001). This could be due to the decreased ability of clindamycin to fight bacteria that often cause infections in shoulder arthroplasty, such as MSSA, C. acnes, and even MRSA. 41 Different conditions occur in the use of clindamycin in knee and hip arthroplasty. Study from Ponce et. al. with 18,798 patients stated that the incidence of SSI between clindamycin was not significantly different from that of cefazolin monotherapy (unadjusted OR = 0.80; adjusted OR = 0.79, 95% CI = 0.41–1.55). 33
In addition to clindamycin, the use of vancomycin and the combination of vancomycin with cefazolin have also been investigated as prophylactic antibiotics with varying results. Several studies have shown that the risk of developing SSI with vancomycin monotherapy is the same or tends to be better than that of cefazolin monotherapy. Study from Yian et. al. with 7140 patients found that there was no difference in the risk of SSI in the use of IV vancomycin compared with IV cefazolin in cases of total shoulder arthroplasty (p = 0.760). 41 In the case of THA & TKA, study from Smith et. al. with 5036 patients stated that the use of vancomycin monotherapy as a perioperative antibiotic was the only variable that caused a decrease in the PJI rate (p = 0.03). 21 Study from Tan et. al. with 18,958 patients also reported that IV vancomycin did not affect the risk of SSI in patients undergoing THA and TKA (p > 0.05), but it found that patients receiving vancomycin monotherapy had a higher risk of experiencing gram-negative bacterial SSI (p = 0.049)10,36
In addition to those studies, several studies with larger samples found that the use of vancomycin actually increased the risk of SSI incidence. Study from Ponce et. al. with 18,798 patients found that there was an increased risk of SSI with vancomycin monotherapy (unadjusted OR = 1.72; adjusted OR = 1.73, 95% CI = 1.20 to 2.49). 33 This evidence is also supported by other studies with larger samples. Study from Zastrow et. al. with 1,299,192 patients also stated that a higher probability of SSI was seen with vancomycin use in THA (OR = 1.36; CI 1.09–1.71) and TKA (OR = 1.29; CI 1.10–1.52), whereas clindamycin (OR = 1.29). = 1.38; CI 1.11–1.71) and the combination of vancomycin with cefazolin (OR = 0.96; CI 0.82–1.11) in TKA. 18 While in the vancomycin and cefazolin combination group, study from Sewick et. al. with 1828 patients, study from Burger et. al. with 1871 patients, and study from Ponce et. al. with 18,798 patients stated that there was no significant difference in the incidence of SSI between cefazolin and the combination of cefazolin and vancomycin (p > 0.05)27,33,43
Several studies above indicate that vancomycin monotherapy tends to increase the risk of SSI. Causes of increased risk of SSI in multifactorial vancomycin monotherapy. Vancomycin has a narrower antimicrobial spectrum than cephalosporins, i.e., it does not include gram-negative bacteria. 60 In addition, vancomycin, although sensitive to MRSA, is less effective against MSSA (Methicillin Sensitive Staphylococcus Aureus) bacteria based on several research data. This condition causes the need for a combination of vancomycin with cefazolin. 4
Percentage of SSI incidence and dosage of prophylactic antibiotic
The accuracy of antibiotic dosing affects the risk of SSI. There are three regimens of antibiotic prophylaxis that have been studied (list of detailed information can be found in supplementary). Study from Rondon et. al. with 17,393 patients stated that the group of patients who received underdose cefazolin had a higher SSI percentage (1.50%) than the group of patients who received the right dose of cefazolin (0.86%). Cefazolin underdose is common, especially in patients weighing >120 kg. Patients who were underdose of cefazolin had a higher risk of PJI than patients who received the correct dose of cefazolin (p = 0.002). Patients who often experience underdose are obese patients weighing more than 120 kg. These obese patients should have received a dose of three grams of cefazolin, but in practice these patients were only given a dose of two grams. 6
Dose mismatches also occur with vancomycin. Study from Kheir et. al. with 1828 patients found that many patients were underdose of vancomycin. The group of patients who received the right dose of vancomycin had an SSI percentage of 1.74%, while the group of patients who received vancomycin overdose and underdose had an SSI percentage of 1.67% and 1.77%, respectively. Although there was no statistically significant difference in SSI cases between patients who received the right dose of vancomycin and those who did not receive the right dose of vancomycin (p = 0.995), patients who received the right dose of vancomycin had an effective blood level of vancomycin (<15 mg/L) (p < 0.001) and did not experience SSI due to MRSA. 24
In addition, studies related to the dose of other prophylactic antibiotics, such as ampicillin + sulbactam, were also carried out Yuasa et. al. with 357 patients. The group of patients who received the doubled dose had a lower SSI percentage (1.08%) than the group of patients who received the standard dose (2.91%). However, the results of statistical analysis did not find a significant difference between the use of standard doses and doubled doses in preventing SSI (p = 0.268). 17
Percentage of SSI incidence and duration of prophylactic antibiotic
There are four regimens of antibiotic prophylaxis that have been studied (list of detailed information can be found in supplementary). The use of single dose cefazolin has an SSI percentage of 1.40%, while the use of cefazolin <24 h have an SSI percentage range of 1.06%–10.58%. For other antibiotic regimens, in general, the group of patients receiving single dose or <24 h of prophylactic antibiotics had a lower percentage of SSI than the group of patients receiving prophylactic antibiotics >24 h.
When viewed from the percentage value of SSI, there is indeed evidence that shortening the duration of prophylactic antibiotics is associated with a decrease in the incidence of SSI. However, considering the statistical results of each study, it is not certain that shortened prophylactic antibiotics reduce the risk of SSI. This can be seen in study from Tan et. al. with 20,682 patients, study from Wyles et. al. with 292 patients, study from Barbero et. al. with 554 patients, and study from van Kasteren et. al. with 1992 patients which found that there was no significant difference in the incidence of SSI between patients receiving received single and multiple doses of antibiotics postoperatively (p > 0.05).11,12,44,46 Study from Chandrananth et. al. with 1019 patients and study from Finkelstein et. al. with 1454 patients only explained that there was no significant difference (p > 0.05) in the incidence of SSI between patients receiving antibiotics < 24 h and > 24 h.13,39
The results of the above study indicate that the shortest effective duration of antibiotic administration to prevent SSI is not known with certainty. Therefore, well-designed studies with larger numbers of patients are needed to ensure the safety of shortening the duration of prophylactic antibiotics.
Percentage of SSI incidence and timing of first dose of prophylactic antibiotics
The timing of the first dose of prophylactic antibiotics also affects the incidence of SSI with antibiotics with a long infusion duration, such as vancomycin. Vancomycin infusion is generally performed over an interval of 60 to 90 min; therefore, it may take at least 45 min to reach 50–75% of the total vancomycin dose to be administered prior to surgical incision. There are three regimens of antibiotic prophylaxis that have been studied (list of detailed information can be found in supplementary). On the cefazolin regimen with vancomycin, study from Burger et. al with 1871 patients found that vancomycin administration at least 45 min before incision had a significantly (p < 0.01) lower percentage of SSI events (0.21%) compared to vancomycin administration less than 45 min before incision (2.73%). 43
Different results regarding the timing of the first dose of prophylactic antibiotics were found in study from Finkelstein et. al. with 1454 patients. The article stated that the time of giving the first dose of antibiotics commonly used in orthopaedic surgery, which is 60 min before incision, had a higher percentage of SSI (4.13%) compared to the time of giving the first dose of antibiotics between one to two hours before incision (3.60%), although the result was not statistically significant (p = 0.79). 39 A well-designed study regarding the timing of the first dose of prophylactic antibiotics with a larger number of patients is still needed to determine the appropriate timing of the first dose of prophylactic antibiotics.
Percentage of SSI incidence and redosing of prophylactic antibiotics
The last factor that affects the effectiveness of antibiotics is re-dosing of prophylactic antibiotics. Intraoperative antibiotic redosing is necessary to ensure adequate serum and tissue antimicrobial concentrations if the duration of the procedure exceeds twice the antimicrobial half-life or there is massive blood loss (> 1500 mL). Redosing of antibiotics is also necessary if there are factors that shorten the half-life of the antibiotic (e.g. hypoalbumin). 4
In this scoping review study, there were no studies that discussed the re-dosing of prophylactic antibiotics in arthroplasty. This is because the time of arthroplasty surgery generally does not reach the half-life of cefazolin, which is ± 3–4 h. This condition can be seen from the duration of the longest operation, which was stated from the selected studies which was only around 2–3 h, so there was no need for re-dosing of antibiotics.
Conclusion
From this scoping review, it was found that most of study in the form of cohort, either prospective or retrospective. Patients with diabetes mellitus (DM) and heart and blood vessels, male, overweight (obese), have a higher risk of developing SSI. Cefazolin is the most used antibiotic prophylaxis with SSI incident from 0,20–16,05%, followed by vancomycin monotherapy (SSI incident 0,27–3,88%), combination of cefazolin and vancomycin (SSI incident 0,29–10,59%), and clindamycin monotherapy (SSI incident 0,31–2,56%). The correct antibiotic prophylactic dose has a lower percentage of the SSI than the wrong antibiotic dose. Meanwhile, administration of prophylactic antibiotics within single dose or <24 h had a lower SSI percentage than administration of prophylactic antibiotics >24 h. Prophylactic antibiotics before incision also have a lower SSI percentage than prophylactic antibiotics after incision. There is still a need for further research related to the duration and specific timing of first dose of prophylactic antibiotics, especially regarding single dose or multiple dose antibiotics.
Supplemental Material
sj-docx-1-otr-10.1177_22104917221082313 - Supplemental material for Use of prophylactic antibiotics on surgical site infections in arthroplasty patients (Scoping Review)
Supplemental material, sj-docx-1-otr-10.1177_22104917221082313 for Use of prophylactic antibiotics on surgical site infections in arthroplasty patients (Scoping Review) by Irsan Fahmi Almuhtarihan, S Suharjono, Primadenny Ariesa Airlangga and Elfri Padolo in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank to all parties who have supported the completion of this review, especially Dean of Faculty of Pharmacy, Airlangga University and Director of Dr Soetomo General Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.