
Abstract
Background:
Majority of studies on chronic postoperative inguinal pain has described the occurrence after unilateral inguinal hernia repair. Endo-laparoscopic repair, for example, laparoscopic transabdominal preperitoneal inguinal hernia repair, has been recommended for primary bilateral symptomatic inguinal hernias, although the literature on chronic postoperative inguinal pain among this type of patients is limited. The present study analyzed chronic postoperative inguinal pain following bilateral transabdominal preperitoneal inguinal hernia repair.
Methods:
Nationwide consecutive patients who underwent bilateral transabdominal preperitoneal inguinal hernia repair (July 2012–June 2013) were recruited from the Danish Inguinal Hernia Database and cross-checked with hospital files and the National Patient Registry. A prospective follow-up was performed with a standardized postal questionnaire including questions on functional performance status assessed by a modified version of the Activity Assessment Scale. The primary outcome was incidence of chronic postoperative inguinal pain defined as moderate to severe pain-related impairment of everyday activities. Pain was registered according to the two individual groin areas. Furthermore, the overall incidence of chronic postoperative inguinal pain per operated inguinal hernia was calculated. Intensity of experienced pain (Activity Assessment Scale score) was compared between patients reporting pain from one versus both groin areas.
Results:
In total, 209 patients (418 hernia repairs) were analyzed (questionnaire response rate 83%). The median follow-up time was 27 months (22–34 months). In total, 27 of 209 patients (13%) complained of chronic postoperative inguinal pain from either one (n = 17) or both (n = 10) groin areas after bilateral transabdominal preperitoneal inguinal hernia repair. The incidence of chronic inguinal pain per operated hernia was 9%. The intensity of impairment due to pain (Activity Assessment Scale score) did not differ significantly between patients with chronic postoperative inguinal pain in one (19%) versus both sides (30%), p = 0.056.
Conclusion:
Bilateral transabdominal preperitoneal inguinal hernia repair for symptomatic inguinal hernias was related to a high incidence (13%) of chronic postoperative inguinal pain and decreased functional performance status.
Keywords
Introduction
Since the introduction of the inguinal hernia mesh repair, the outcome focus has shifted from recurrence to chronic pain (1–4). The incidence of chronic pain depends on the definition of pain, design, and quality of the study. Although findings are not uniform, the incidence of moderate to severe chronic postoperative inguinal pain during rest has been reported in 6% of patients (per operated hernia) after unilateral laparoscopic inguinal hernia repair (5).
Bilateral symptomatic inguinal hernias requiring repair are common (6) and reported in up to one-third of patients (7). Male patients previously operated for a direct unilateral inguinal hernia seem especially at risk of a subsequent contralateral repair within few years after index surgery (8). In this context, the clinical dilemma is that bilateral repair is cost-effective but may be unnecessary with a possible increase in risk of inducing chronic pain compared with unilateral repair. Therefore, due to the risk of overtreatment and chronic pain, a prophylactic bilateral transabdominal preperitoneal inguinal hernia repair (TAPP) for a contralateral asymptomatic inguinal hernia in patients scheduled for a unilateral repair is controversial. None of the strategies are supported by high qualitative evidence. It is of uttermost importance that knowledge is obtained on major outcomes after bilateral TAPP. The long-term incidence of chronic postoperative pain following bilateral TAPP has previous only been reported as major outcome in one study with few patients (4).
The present study was primarily undertaken to provide evidence for the incidence of activity-related chronic postoperative inguinal pain following bilateral TAPP in an all-male Danish setting. Impaired sexual activity and sleep disturbance due to pain was also recorded.
Hypothesis: The hypothesis for the present study is that bilateral TAPP is associated with higher incidence of chronic postoperative pain due to the extended surgery while repairing two inguinal hernias versus one during unilateral repair.
Methods
The explorative study was based on nationwide consecutive prospective patients’ data identified in the Danish National Patient Registry and cross-checked with the Danish Inguinal Hernia Database (DHDB; 90% coverage of all inguinal hernia repairs in Denmark) (9–12). Furthermore, data were cross-checked between retrospective hospital patient files, the DHDB, and the National Patient Registry for subsequent repair for recurrence.
Setting
The study period was from 1 July 2012 to 30 June 2013. Patients fulfilling the inclusion criteria were invited to participate by questionnaire 2 years after surgery. Follow-up was defined as time from surgery (bilateral TAPP) until questionnaires were signed. The questionnaire was posted by regular mail 2 years after index surgery. A reminder was sent out once (maximum two postal questionnaires) to non-responders, and if a response was still not received, patients were contacted by phone.
Participants, Inclusion And Exclusion
Danish male patients, age ⩾18 years, who had bilateral TAPP due to symptomatic primary inguinal hernias during the study period were included. Before repair, none of the patients were asymptomatic (information from medical patient charts). Written informed consent was obtained from all the participants.
Patients who had a psychiatric diagnosis, non-Danish-speaking patients, and patients who had either died or emigrated were excluded. Furthermore, patients for whom the surgical code had been misclassified (e.g. unilateral repair in the same side registered twice or femoral hernia repair registered as inguinal hernia repair) were also excluded.
Danish Inguinal Hernia Database
The DHDB covers >90% of all inguinal hernia repairs in Denmark since 1998. The DHDB is a national administrative database, and registration is mandatory. Each individual inguinal hernia repair is logged by the surgeon. Each side (left/right) is reported separately. The database contains information about inguinal hernia anatomy as well as intraoperative technique and materials used. Registration is based on diagnosis and procedure-related code classifications (the NOMESCO Classification of Surgical Procedures codes as well as the International Statistical Classification of Diseases and Related Health Problems, 10th Revision diagnosis codes). Due to the unique Danish social security number system, it is possible to cross track each individual patient through the database as well as hospital records to control for correct surgical codes.
Assessment Scale Questionnaire
A prospective follow-up was obtained by a standardized postal questionnaire concerning inguinal pain, sexual activity, sleep, and recurrence.
The primary outcome was chronic postoperative inguinal pain defined as moderate to severe pain-related impairment of everyday activities, assessed by a modified version of the Activity Assessment Scale (AAS) questionnaire (13, 14). The AAS may be used for evaluation of pain-related impairment of everyday physical activities after surgery. A modified version of the AAS was used in the current study. The present version of the AAS was shortened to eight questions since the original AAS questionnaire implicates several duplicate situations. Moreover, in the original questionnaire, sexual activity was included. In the present study, we specifically asked patients about sexual activity. The modified AAS questionnaire consists of eight questions regarding physical activity, where each is scored from 1 to 5 points (1 point = no physical impairment, 5 points = unable to perform the activity due to pain), resulting in a summed AAS score from 8 to 40 points. The AAS score can be transformed to a percentage (0%–100%). A score of 0% equals no pain-related physical impairment, 100% equals maximum impairment of daily activities (14). A score of 12.5% is equivalent of being unable to perform an activity (5 points) or having less than maximum impairment in several activities. Patients were instructed to score the pain as perceived on average during the previous 24 h. Pain was registered according to the two individual groin areas. In patients who reported pain from both groin areas, the maximum pain score was chosen in the analysis. We defined chronic postoperative inguinal pain as moderate to severe functional impairment of daily activities due to pain (AAS score ⩾ 12.5%). Furthermore, intensity of impairment due to pain (AAS score) was compared between patients reporting pain from one versus both groin areas. The overall incidence of chronic postoperative inguinal pain per operated inguinal hernia was also analyzed.
Also, a lateral versus medial hernia and young versus old patients (below or above median age) were analyzed according to the moderate/severe versus no/little pain AAS score (maximum AAS score in one of the two groins). Patients with pantaloon hernias were excluded (n = 24).
Secondary Outcome
All patients were asked about sleep disturbance and/or disturbance of sexual activity during the preceding 3 months due to chronic postoperative inguinal pain. Patients with no sexual activity before operation were excluded from this analysis. These questions were not part of the modified AAS. Finally, patients noted suspicion of hernia recurrence in the left and/or right side repair during follow-up. No clinical follow-up was performed by a physician.
Bias
Data were cross-checked between the DHDB, retrospective hospital patient files, and the Danish National Patient Registry for accuracy (e.g. correct surgical code) and subsequent repair for recurrence. Furthermore, we intended to include all male Danish patients who had bilateral TAPP during the study period to minimize selection bias.
Study Size
The study was explorative in nature and not based on a pre-study power calculation for sample size.
Statistical Methods
Descriptive values are expressed as frequencies or percentages or median with ranges. Mann–Whitney and chi-square tests were used as appropriate. A value of p < 0.05 was considered statistically significant. Follow-up time was calculated as the period from index repair until patients signed the questionnaire (months). Statistical analyses were performed using SPSS® 23.0 for Windows (SPSS Inc, Chicago, Illinois, USA).
Results
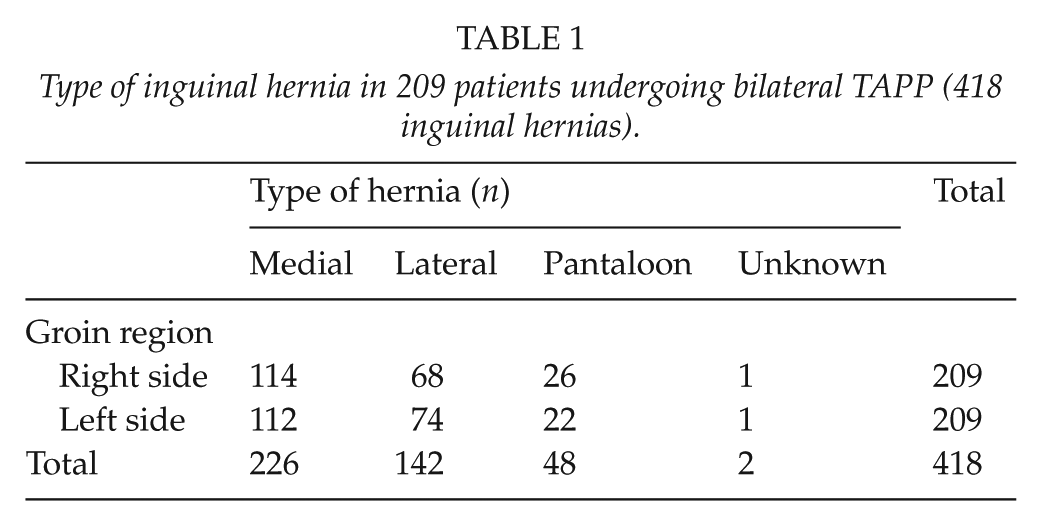
The study profile is shown in Fig. 1. In total, 329 patients with a bilateral TAPP were identified in the Danish National Patient Registry and the Danish Inguinal Hernia Database (DHDB). Since 77 patients failed to meet the inclusion criteria, 252 patients were sent a follow-up questionnaire. As 43 patients did not respond to the questionnaire, the study analysis was based on data from 209 patients (418 inguinal hernias; response rate 83%; Table 1). Median follow-up times were 27 months (22–34 months). Follow-up for repair of recurrence in the DHDB was 100%. Median age at index surgery was 66 years (31–90 years).
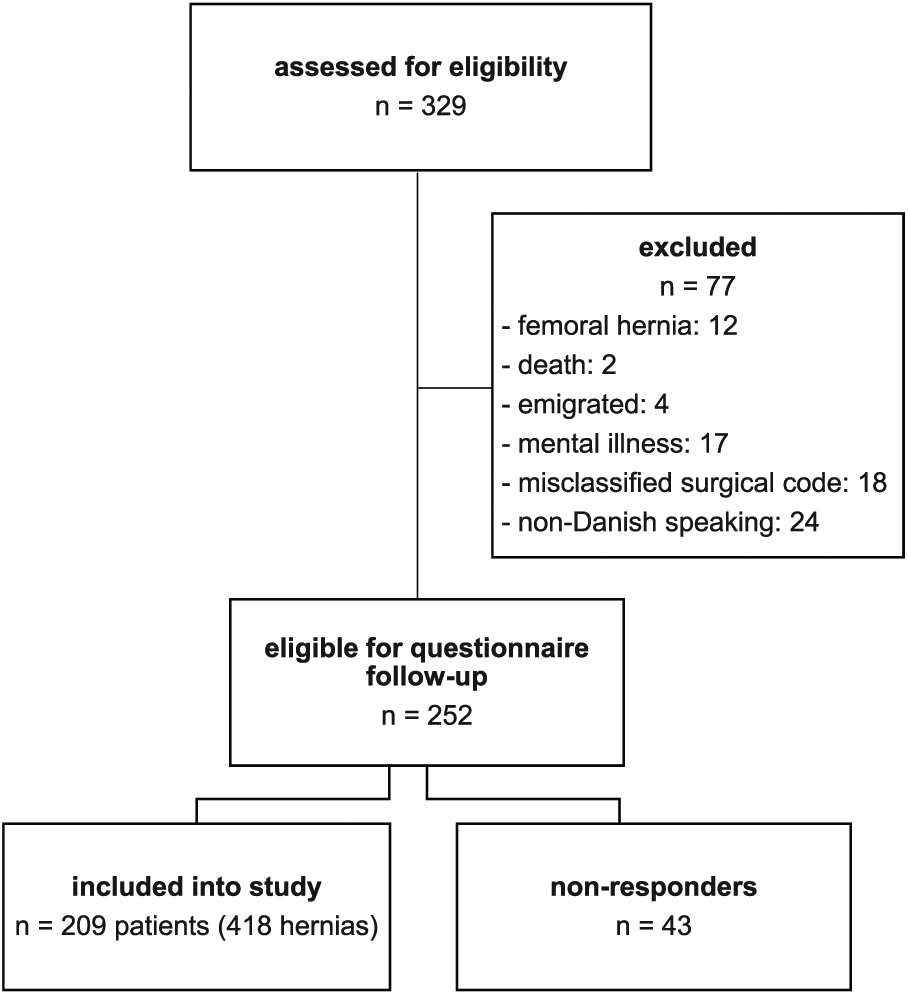
Study flowchart according to the CONSORT statement (15).
Type of inguinal hernia in 209 patients undergoing bilateral TAPP (418 inguinal hernias).
Data on non-responders were not available due to a lack of informed consent from this group.
A total of 27 patients (13%) complained of chronic postoperative inguinal pain from either one (n = 17) or both (n = 10) groin areas after bilateral TAPP.
The incidence of chronic postoperative inguinal pain per operated hernia was 9% (n = 37 of 418 hernias, see Fig. 2). The intensity of impairment due to pain (AAS score) did not differ significantly between patients with chronic postoperative inguinal pain in one versus both sides, 19% versus 30%, respectively, p = 0.056. No difference was seen regarding intensity of impairment due to pain between patients who suspected a recurrent hernia and those who did not (p > 0.05). The number of patients with moderate/severe pain (vs no/little pain) did not significantly differ according to repair for a lateral versus medial hernia (p > 0.05). Furthermore, pain intensity among young versus old did not significantly differ (p > 0.05).
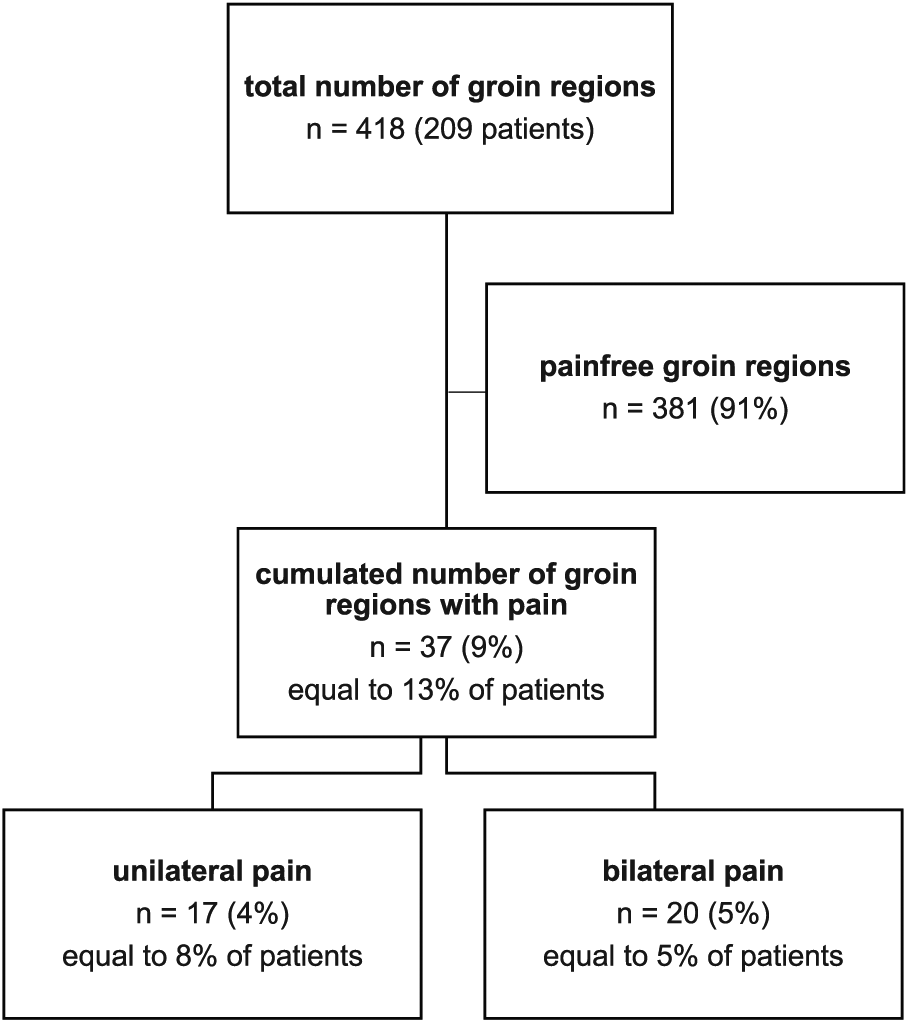
Flowchart showing distribution of chronic pain among patients.
The most common pain-related impairment of activities was “moderate physical work” (Fig. 3).
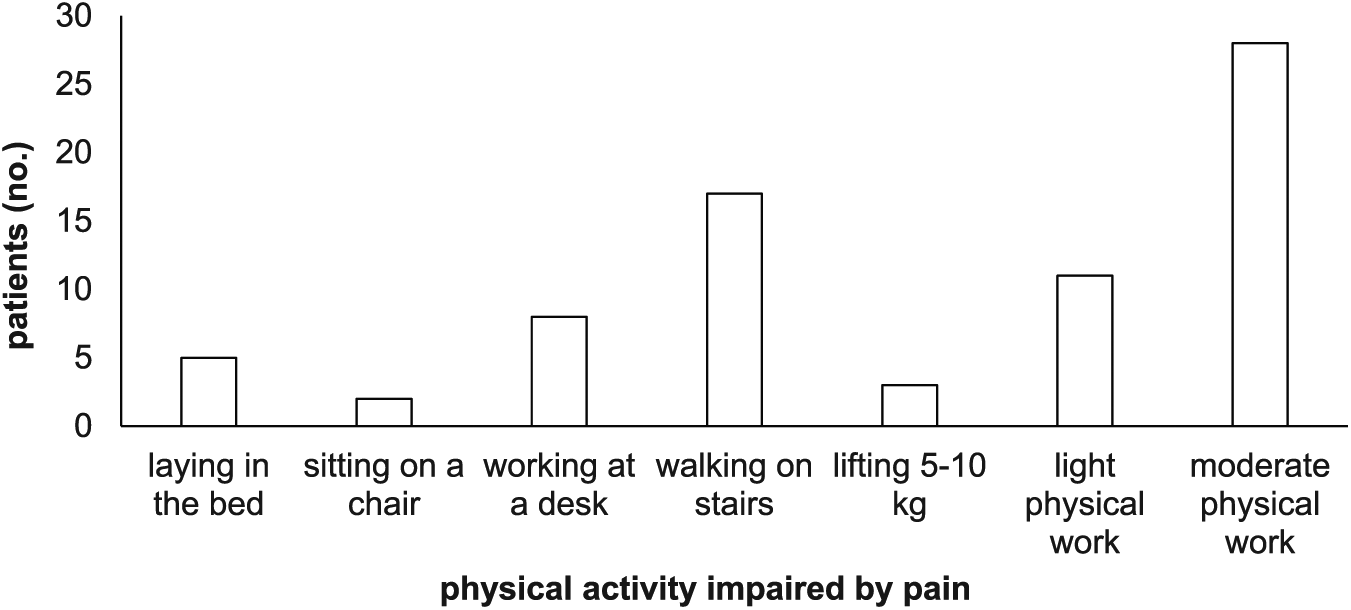
Number of patients with pain-related physical impairment of daily activities according to the Activity Assessment Scale (AAS) registrations.
Chronic postoperative inguinal pain-induced sleep disturbance was reported by three (1%) patients with unilateral pain and two (1%) with bilateral pain.
A total of 178 patients were sexually active before the surgery. Seven (4%) sexually active patients reported sexual impairment due to unilateral pain and five (3%) due to bilateral pain. Two patients experienced a complete compromised sexual life due to pain.
During the 2-year follow-up period, two patients (1%) were operated due to recurrence, whereas 49 patients (23%) noted suspicion of hernia recurrence (unilateral 30 and bilateral 19)). No patients underwent more than one repair for recurrence.
Discussion
The main finding of this study was that chronic postoperative inguinal pain after bilateral TAPP was present among 13% of Danish male patients 2 years after surgery.
A high incidence of chronic postoperative inguinal pain and decreased functional performance status was seen among patients in the present study: Thirteen percent experienced moderate to severe physical impairment of daily activities due to chronic postoperative inguinal pain. Furthermore, 8% experienced impaired sexual life due to chronic pain as well as 2% who reported pain-induced sleep disturbance. The risk related to bilateral TAPP, for example, chronic postoperative inguinal pain and sexual dysfunction, is an important factor to discuss with patients prior to inguinal hernia surgery as it may severely impact the life of those affected and as current methods of treatment have not been effective (16). The incidence of chronic pain after inguinal hernia repair is associated with the type of repair, definition of chronic pain, period of follow-up, and method of measurement (AAS, PIQ-6 (Pain Impact Questionnaire), VAS (Visual analog scale), and so on). The 13% incidence of pain described in our study on bilateral TAPP correlates well with studies on unilateral TAPP where a 6% incidence of chronic postoperative inguinal pain has been described (5). Only few studies on chronic pain after laparoscopic bilateral inguinal hernia repair exist. Bignell et al. (4) described chronic postoperative inguinal pain based on the pain severity score (scored from 0 to 5, 0 = none, 5 = very severe) within the last 4 weeks. In this study, the authors randomized (n = 120) to either bilateral TAPP (n = 60) or bilateral Lichtenstein repair (n = 60), reporting chronic pain 10 years after index surgery. Chronic pain was present in 15% of patients after bilateral TAPP (4). Unfortunately, the definition of pain and the assessment tools used (SF12v2 and PIQ-6) makes a direct comparison with our and other Danish studies (14), using modified versions of the AAS, difficult. The AAS measures a full spectrum of daily activities, from leisure to hard physical labor, and has previously been both validated in patients undergoing surgery (13) and proven useful in studies on chronic pain after inguinal hernia repair (17). Due to this, we chose to use a modified version of the AAS questionnaire for the present study.
In the present study, 23% of all patients reported suspicion of recurrence, but according to the DHDB, only 2% had an operation for recurrence during follow-up. The discrepancy using reoperation as a proxy for recurrence versus clinical recurrence is documented in a study on patients undergoing ventral hernia repair (18). Suspected recurrence was based on patients’ suspicion on recurrence when physical examination was performed. For these uncertainty reasons, we did not analyze suspicion on recurrence to incidence of chronic pain.
There are several limitations to the present study. First, systematic data from preoperative pain and other well-defined risk factors (mental vulnerability, preoperative low pain threshold, and so on) were not available from the patients’ records. Second, in the present study, a modified version of the original AAS was used. Therefore, the validity of the questionnaire can be questioned. Furthermore, medical patient charts were heterogenic, and no standardized data on baseline characteristics of the included patients were available (body mass index (BMI), smoking, preoperative chronic pain). Third, although based on a national cohort of all males who underwent bilateral TAPP in Denmark, the study includes relatively few patients and may be criticized for its retrospective nature, despite the prospective perioperative data and follow-up questionnaire using pre-study defined variables. This may partly explain the risk of statistical type II errors in the statistical comparison of pain intensity from the one-sided versus bilateral pain origin, which did not reach statistical significance (p = 0.056). Finally, physical examination was not performed to confirm patients’ suspicions of recurrence but may suggest that the reoperation rate may severely underestimate the factual recurrence (clinical and reoperation for recurrence) in patients’ TAPP. Also, the discrepancy between suspected recurrence and the reoperation rate after index surgery may be due to patient’s reluctance to undergo surgery again. Finally, it was not possible (Danish laws regarding data privacy) to analyze data on responders versus non-responders. Therefore, an analysis of responder bias according to incidence on chronic pain was not possible.
Regarding future aspects, the incidence of chronic postoperative inguinal pain after bilateral TAPP is of interest when discussing the strategy for surgical treatment of occult inguinal hernias. The current International Guidelines for Groin Hernia Management (6) recommends immediate repair of occult inguinal hernias encountered during TAPP, although the evidence is weak. One of the drawbacks in the current recommendation is the lack of knowledge on chronic postoperative inguinal pain when extending a planned unilateral TAPP to a bilateral repair. To determine whether bilateral repair should be performed when encountering occult inguinal hernias during unilateral TAPP, future large-scale studies are needed. Also, a future study should analyze chronic postoperative inguinal pain in patients undergoing unilateral endo-laparoscopic repair versus patients with a symptomatic unilateral inguinal hernia and a contralateral occult inguinal hernia undergoing bilateral repair. Also, future large-scaled studies on postoperative chronic pain should be supplemented with preoperative risk factors, as mentioned above. Patients may be recruited through international collaborations between clinical hernia databases with a proven high inclusion rate and a valid long-term follow-up (19, 20).
In conclusion, bilateral TAPP for symptomatic inguinal hernias was related to a high incidence (13%) of chronic postoperative inguinal pain and decreased functional performance status 2 years after surgery. This is higher than in studies on chronic postoperative inguinal pain after unilateral TAPP and should be taken into account when encountering asymptomatic occult hernias during planned unilateral TAPP. Thus, patients should be informed about cost-effectiveness to operate an occult hernia versus the potential risk of chronic pain.
Footnotes
Acknowledgements
We thank all participating public surgical centers in Denmark, the private hospital Aleris-Hamlet Denmark, and the Danish Hernia Database for their help in providing us with data for this study. Clinicaltrials.gov identification: NCT03155230.
Author Contributions
N.J., C.D.V., and T.B. contributed to study conception, design, and critical revision of the manuscript. N.J. and C.D.V. helped in acquisition of data. N.J. and T.B. analyzed and interpreted the data and drafted the manuscript.
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Danish Health Authority (Sundhedsstyrelsen) approved this study: SST 3-3013-783/1. The Danish Data Protection Agency and the Danish Ethics Committee (case no.: h-1-2014-113) endorsed this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all individual participants included in the study.