
Abstract
Background and Aims:
Endoscopic retrograde cholangiopancreatography followed by laparoscopic cholecystectomy is often used as definitive treatment for common bile duct stones. The aim of this study was to investigate the optimal time interval between endoscopic retrograde cholangiopancreatography and laparoscopic cholecystectomy.
Materials and Methods:
PubMed and Embase were searched for studies comparing different time delays between endoscopic retrograde cholangiopancreatography and laparoscopic cholecystectomy. Observational studies and randomized controlled trials were included. Primary outcome was conversion rate from laparoscopic to open cholecystectomy and secondary outcomes were complications, mortality, operating time, and length of stay.
Results:
A total of 14 studies with a total of 1930 patients were included. The pooled estimate revealed an increase from a 4.2% conversion rate when laparoscopic cholecystectomy was performed within 24 h of endoscopic retrograde cholangiopancreatography to 7.6% for 24–72 h delay to 12.3% when performed within 2 weeks, to 12.3% for 2–6 weeks, and to a 14% conversion rate when operation was delayed more than 6 weeks.
Conclusion:
According to this systematic review, it is preferable to perform cholecystectomy within 24 h of endoscopic retrograde cholangiopancreatography to reduce conversion rate. Early laparoscopic cholecystectomy does not increase mortality, perioperative complications, or length of stay and on the contrary it reduces the risk of reoccurrence and progression of disease in the delay between endoscopic retrograde cholangiopancreatography and laparoscopic cholecystectomy.
Keywords
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is considered standard treatment for patients presenting with common bile duct stones (1) and is successful in more than 90% of patients (2). However, ERCP can induce complications including pancreatitis and cholecystitis (1, 3, 4). These complications may affect a subsequent laparoscopic cholecystectomy (LC) leading to conversion to open cholecystectomy, perioperative complications, and longer operating time (5–8). It is not yet known whether or not the time interval between ERCP and LC plays a part in increasing conversion rates, complications, and operating time.
The purpose of this systematic review was to investigate whether or not the time interval between ERCP and LC affects the rate of conversion to open surgery and risk of operative complications.
Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline (9). Prior to data extraction and analysis, a protocol for the review was registered in the PROSPERO database with the registration number CRD42015029322 (10).
Eligibility Criteria
Observational (cohort and register-based) studies and randomized controlled trials (RCTs) written in English or Danish were included. The population included adults who had pre- or intraoperative ERCP, which was followed by LC. A comparison of time frames between each study was made. Patients within the different time frames were compared according to outcomes. The primary outcome was the rate of conversion from laparoscopic to open cholecystectomy, and secondary outcomes were 30-day mortality, length of stay (LOS), perioperative complications, and duration of surgery.
Information Sources and Search Strategy
The literature search was conducted in PubMed and Embase on 24 November 2016. The following search strategy was developed in PubMed, and thereafter adjusted to fit Embase: (((laparoscopic cholecystectomy or laparoscopic cholecystectomies or celioscopic cholecystectomy or celioscopic cholecystectomies) and (endoscopic retrograde cholangiopancreatography or endoscopic retrograde cholangiopancreatographies or ERCP) and (gallstone or gall stones or biliary calculi or gall stone or common bile duct calculi or common bile duct gallstones or common bile duct gallstones or common bile duct biliary calculi or cholelithiasis)) not children not infants).
The review tool Covidence (11) was used to screen the results from the literature search. After import of the results, duplicates occurring in both databases were removed prior to the first screening. Two authors (C.F., J.P.R.) independently screened titles and abstracts for relevant publications. Any disagreements were solved by discussion.
Data Collection Process
The extracted data included demographics, methods used in the study such as aim of study, inclusion and exclusion criteria, and study design. Details of interventions used in each group, time between ERCP and LC, and outcomes such as conversions, mortality, LOS, perioperative complications, operating time, and complications in delay between ERCP and LC were also collected.
Risk of Bias
As the systematic review includes both cohort studies and RCTs, two different risk of bias tools were used. Risk of bias within cohort studies was assessed using the Newcastle Ottawa Scale (NOS) (12). The scale judges each study in three areas: selection process, comparability of groups, and outcome assessment. Each area rewards a number of stars depending on bias in the study and a study can receive a maximum of nine stars. A high amount of stars represents a study with low risk of bias.
Risk of bias within RCTs was assessed using The Cochrane Collaboration’s Risk of Bias Assessment Tool (13). This tool examines six different domains in each study: sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. In each domain, a “yes,” “no,” or “unclear” can be obtained for each individual study. Receiving a “yes” corresponds to a low risk of bias while a “no” equals the opposite. If a study receives an “unclear” judgment, there is an uncertain risk of bias in the belonging domain.
Statistics
The studies were heterogeneous to an extent that we chose not to perform a meta-analysis (14). Due to low sample size, many of the studies did not reach a level of significance but only showed tendencies. In order to get clinically relevant results, data concerning the primary outcome were pooled. A chi-square test was performed on the overall results despite the weak scientific value of the pooled estimate. Data were pooled if the time frame between ERCP and LC was stated clearly in the text or tables.
Results
The literature search produced 1911 publications. After duplicates were removed, 1652 publications were screened on title and abstract. Of these, 41 publications were potentially relevant, and further assessment revealed 14 publications eligible for this review (Fig. 1).
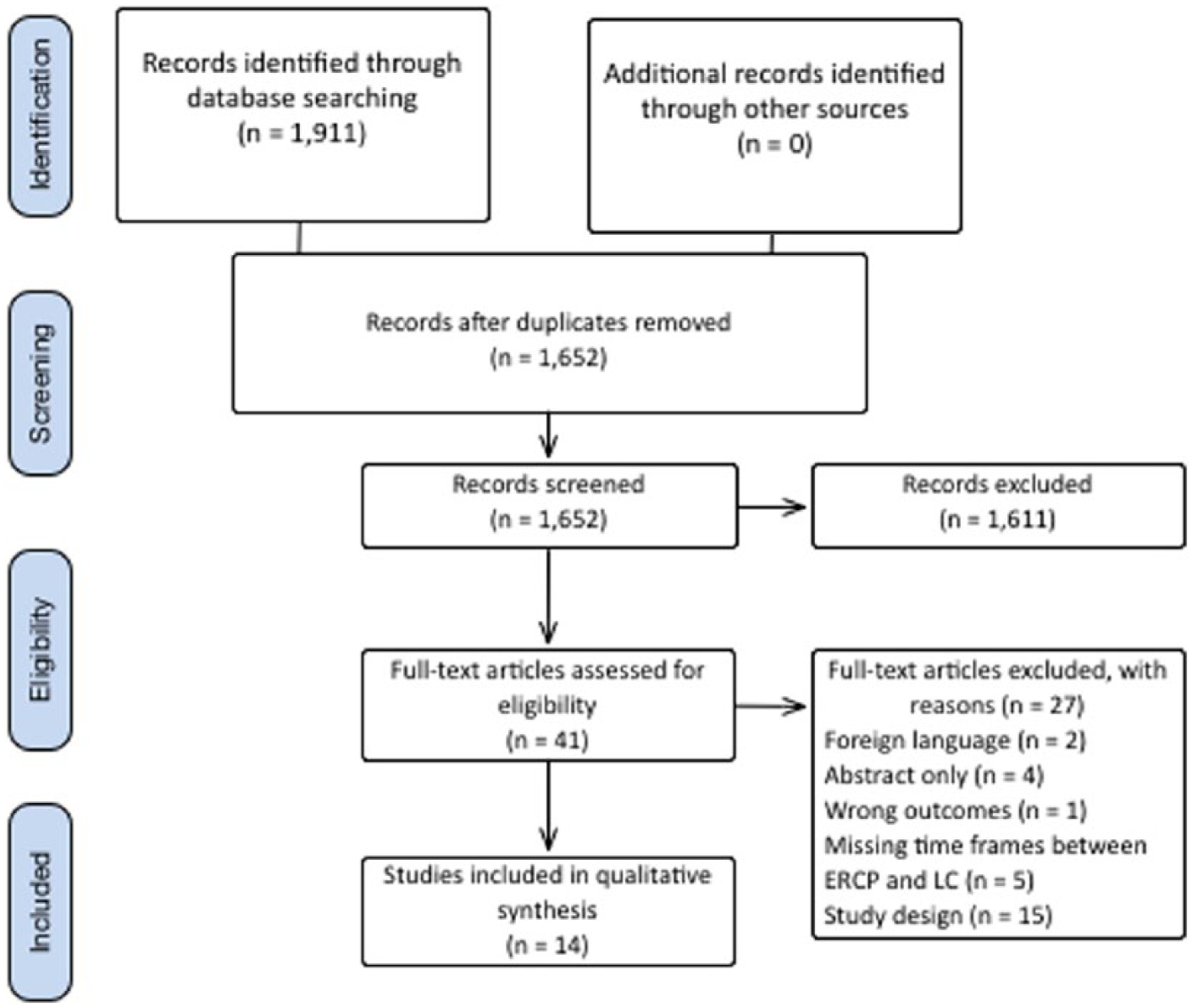
Flow diagram of identification, screening, and eligibility process.
The eligible studies included eight retrospective cohort studies, two prospective cohort studies, and four RCTs, evaluating a total of 1913 patients (6, 15–27). Table 1 summarizes the characteristics of each study, including the time delay between ERCP and LC.
Study characteristics of included cohorts and randomized controlled trials.
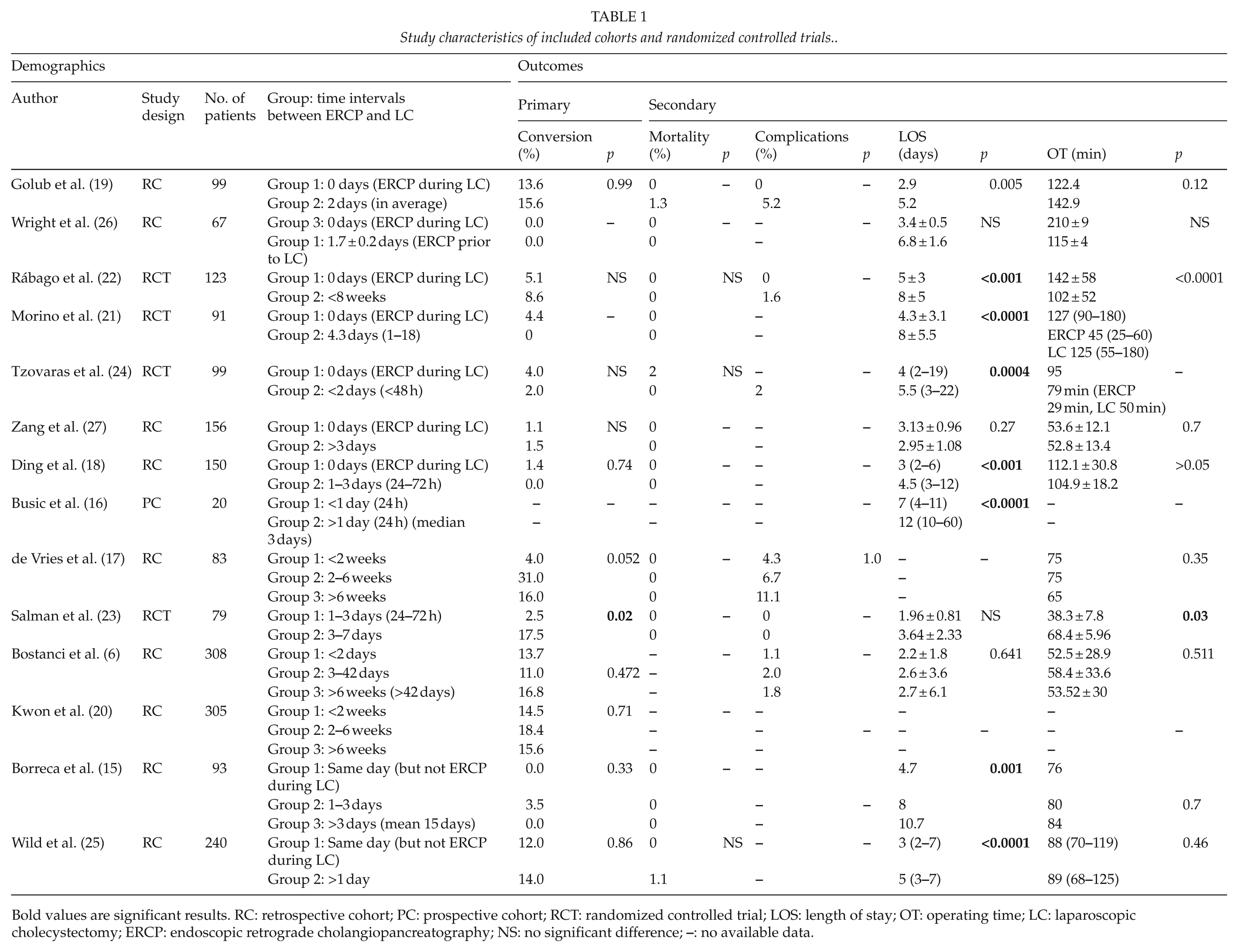
Bold values are significant results. RC: retrospective cohort; PC: prospective cohort; RCT: randomized controlled trial; LOS: length of stay; OT: operating time; LC: laparoscopic cholecystectomy; ERCP: endoscopic retrograde cholangiopancreatography; NS: no significant difference;
Risk of Bias
The median score of the observational studies assessed with NOS score was 7 (range, 5
Risk of bias table according to the Newcastle Ottawa Scale (12).
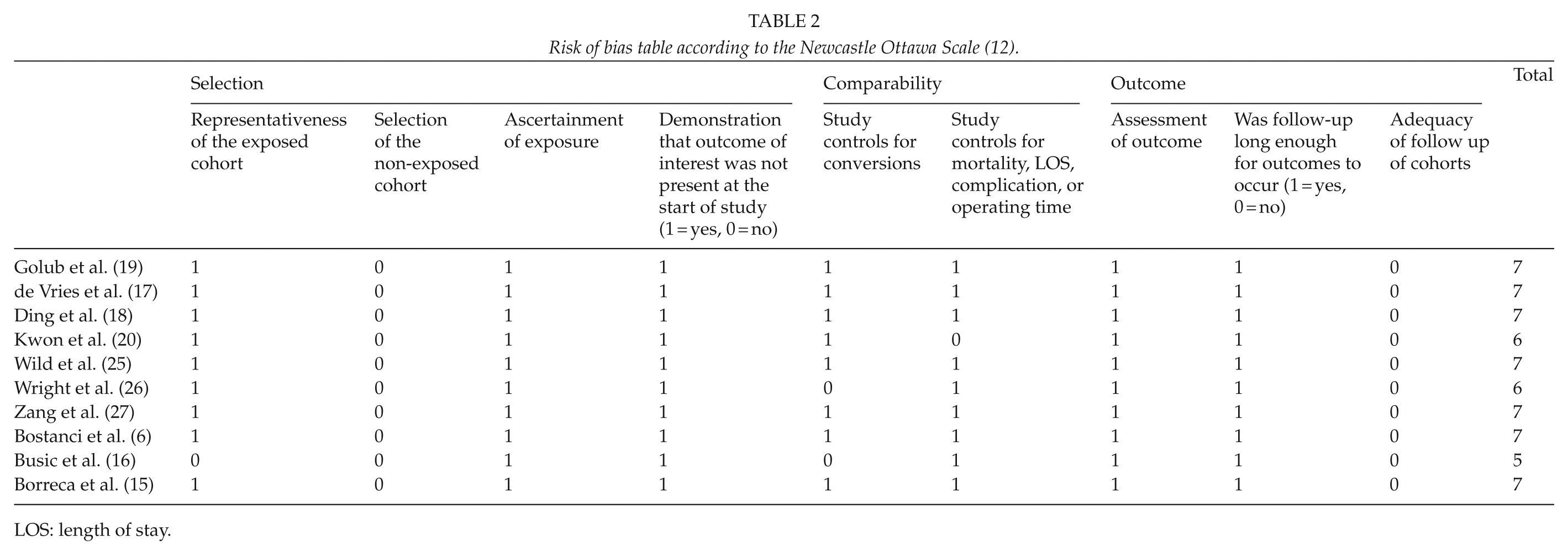
LOS: length of stay.
Risk of bias in the RCTs varied between studies (Fig. 2). It was not possible to evaluate risk of bias in three domains: blinding of participants, personnel and outcome assessors, and other sources of bias. In three (22–24) of the four RCTs, there was high risk of bias in selective outcome reporting.
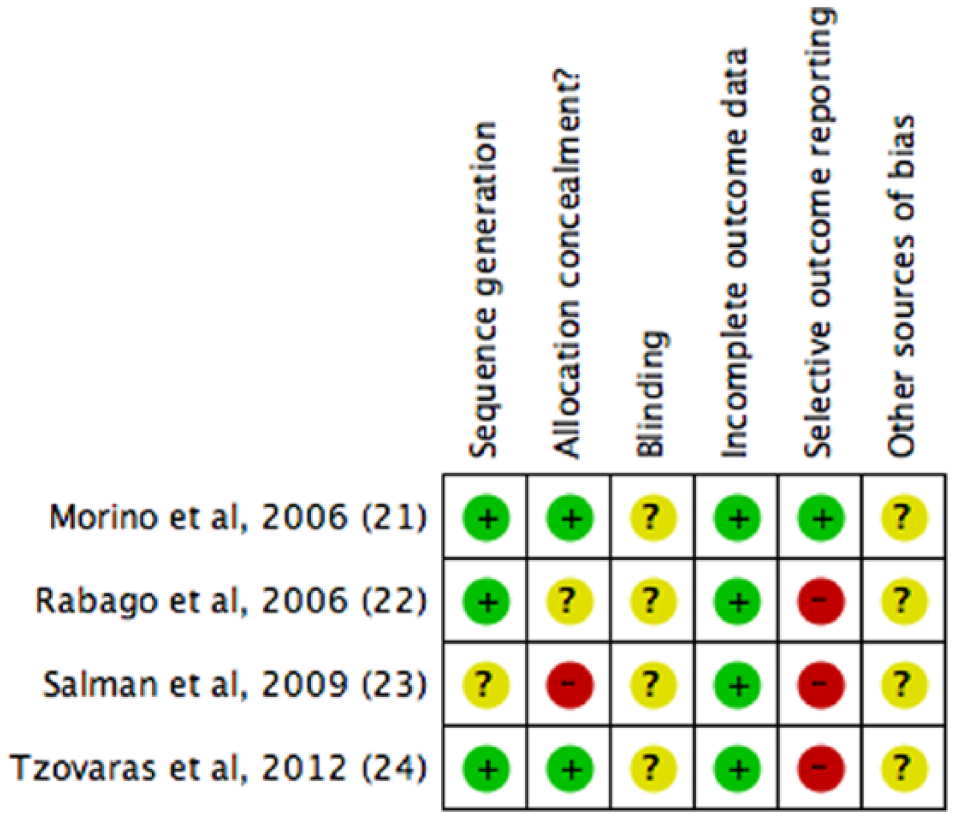
Risk of bias table according to the Cochrane Collaboration’s tool (13).
Baseline Characteristics
The baseline characteristics, including age (6, 15, 17–27), gender (6, 15, 17, 18, 20–27), American Society of Anesthesiologists (ASA) score (18–20, 23, 24, 27), body mass index (BMI) (23, 24), size of common bile duct stone (20, 21, 23, 24, 27), and level of bilirubin (15, 18, 21, 23, 27), were not significantly different in the studies that registered the characteristics. Only in two studies (6, 22) there was a significant different between groups on two parameters, bilirubin and BMI.
The severity of the gallbladder disease was registered in some of the studies (Table 3). Four studies excluded patients with acute cholecystitis, cholangitis, and gallstone pancreatitis (15, 18, 21, 23). In one study, significantly more patients in the delayed group had acute cholecystitis (20), and four other studies found no difference between groups (17, 19, 22, 25). Another study (26) had significantly more patients with either cholangitis or gallstone pancreatitis in the delayed group, and in five studies there was no difference (17, 19, 20, 22, 25).
Gallbladder disease severity.
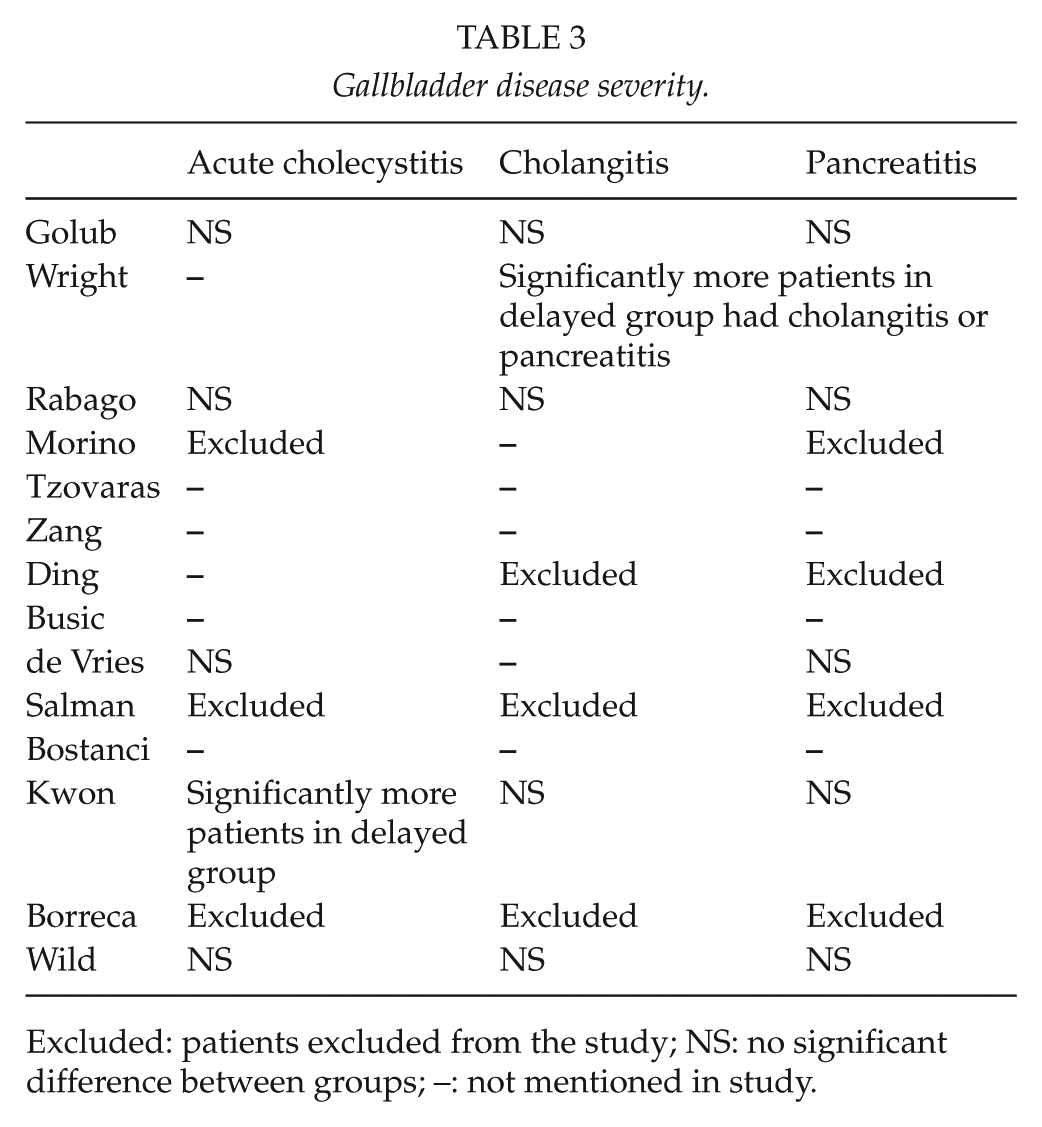
Excluded: patients excluded from the study; NS: no significant difference between groups; –: not mentioned in study.
Conversion Rate
Conversion rate was an outcome in 13 studies (6, 15, 17–27). In the results from the individual studies, there was no significant difference in conversion rate when ERCP and LC during the same session or within 24 h were compared to a delay between ERCP and LC of less than 2 weeks (15, 18, 19, 21, 24–27). However, when results from the studies were combined, the pooled estimate showed an increase in conversion rate as time increased between ERCP and LC, from 4.2% when operated within 24 h to 14% when operated more than 6 weeks after ERCP (p < 0.0005) (Fig. 3). In two studies a group was excluded, as the time frame between ERCP and LC was too wide (22) or unclear (27). Conversion rate was lowest when LC was performed within 24 h of ERCP and increased significantly to 7.6% with a 24
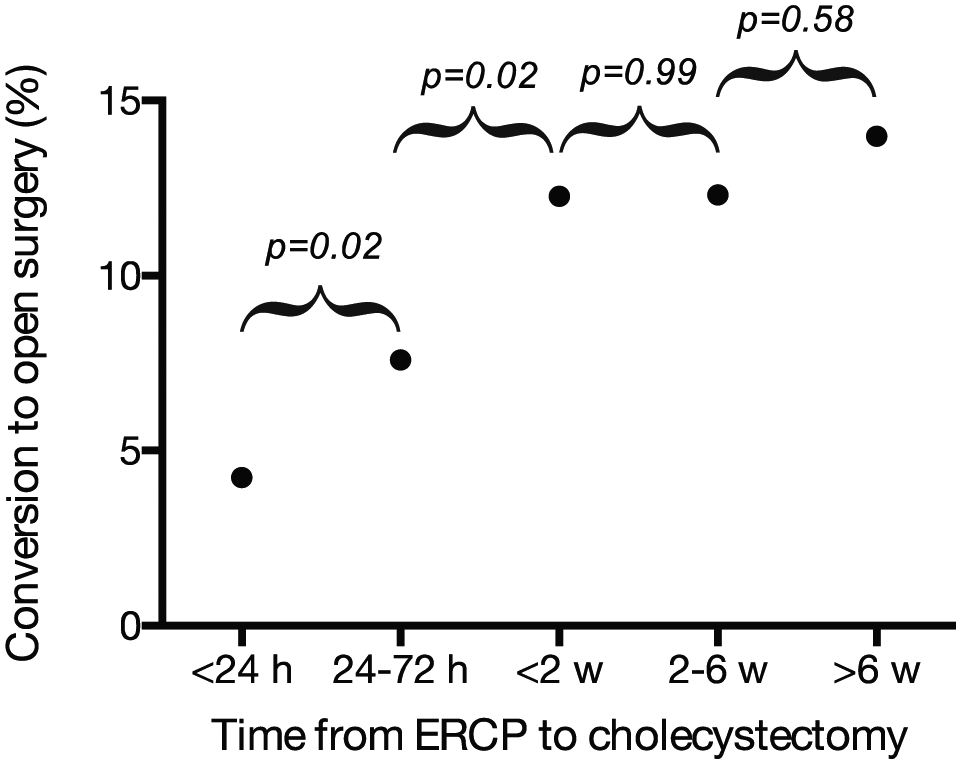
Pooled data demonstrating how delay between ERCP and cholecystectomy affects the rate of conversion from laparoscopic to open cholecystectomy. Overall chi-square test: p < 0.0005.
Considering the individual studies, two small studies with 83 and 79 patients, respectively, showed a significant difference in the conversion rate when there was a longer delay between ERCP and LC (17, 23). The first study (17) revealed a time-wise development. The lowest conversion rate (4%) was seen in the group with a delayed surgery of less than 2 weeks, and then the conversion rate peaked (31%) in the group delayed 2
Mortality
In all, 11 of 14 studies included mortality in their results (15, 17–19, 21–27). Of these, three studies reported deaths among patients (19, 24, 25). Mortality was very low; one study (24) reported mortality of 2% in a group receiving ERCP and LC in the same session, but no mortality in the group with a delay of 48 h to LC, whereas two other studies (19, 25) had no mortality in the group with LC within 24 h, but respectively 1.3% and 1.1% mortality in the groups with a delay of more than 2 days. Thus, because of the very low mortality rates, it was not possible to conclude anything regarding this secondary outcome parameter.
Complications In Waiting Time Between Ercp And LC
Three studies registered complications in the period between ERCP and LC (15, 17, 20). One study reported a risk of recurrence (defined as upper right quadrant pain combined with common bile duct stones on imaging and laboratory tests) of 15% at 15 days and 20% at 1 month (15). Two studies reported that 3.6% and 8.5% developed acute cholecystitis in the delay between ERCP and LC (17, 20).
Perioperative Complications
Six studies reported perioperative complications (6, 17, 19, 22–24). None of the studies that compared groups where ERCP and LC occurred within the first 2 weeks showed any significant results (6, 19, 22, 23, 26). Perioperative complications such as common bile duct injury and bile leak were seen in both the same-session groups and the groups with delay between ERCP and LC. In two studies, the consequence of a longer delay between ERCP and LC was explored in relation to perioperative complications (6, 17). One of these studies (17) showed a significant difference in the rate of perioperative complications. The group with the longest delay between LC and ERCP (6 weeks) had the highest rate of perioperative complications (11.1%). This was compared with groups delayed 2 weeks and 2
LOS
A total of 12 studies reported LOS (6, 15, 16, 18, 19, 21–27). Across all studies except one (6), there was a tendency for a longer LOS as the delay from ERCP to cholecystectomy increased. One study (23) defining LOS as the postoperative LOS found LOS to be longest (median 4 days) in the group delayed 3
Duration of Surgery
A total of 12 studies reported duration of surgery (6, 15, 17–19, 21–27). Seven studies included a group with same-session ERCP and LC (18, 19, 21, 22, 24, 26, 27). Of these, three studies showed a significant difference with a longer operating time in the same-session group (22, 24, 26). The difference in mean operating time was 40, 16, and 95 min, respectively. In the study with only 16-min difference in operating time, both ERCP and operating time was included, and this was not specified in the remaining two studies. In the remaining five studies, all groups had a delay between ERCP and LC (6, 15, 17, 23, 25). In these, only one of the studies showed a significant difference (23). Operating time was longest (68 min) in the group with the longest delay between ERCP and LC (3
Discussion
This systematic review concerning the optimal timing for LC after ERCP showed a tendency for a lower conversion rate when LC was performed within 24 h of ERCP. The conversion rate increased when the delay between ERCP and LC increased but leveled off when the delay was longer than 2 weeks. LOS also supported a short delay between ERCP and LC, however, when studied carefully it became clear that the increase in LOS was due to the intentional delay between ERCP and LC. The review also showed a high risk of reoccurrence of bile duct stones or acute cholecystitis as delay between ERCP and LC increased.
The most noticeable finding in this systematic review was the conversion rate when all data were pooled (Fig. 3). It was clear that patients should preferably be operated within 24 h of ERCP or at least within the first few days. This is supported by one of the bigger RCTs (22) with a significant lower conversion rate when operated within 72 h than 3
The strength of this review is that it, to our knowledge, is the first review regarding this subject. This review aimed for a high transparency, as it followed PRISMA guidelines as well as the registration of a protocol in the PROSPERO database. However, a limitation comes from the available studies with low comparability caused by the high variety of time frames between the subdivided groups. Between the studies there was also a variety in inclusion and exclusion criteria based on gallbladder disease severity; however, the baseline characteristics show that there was only little variety between groups in the individual studies. Another limitation was that this review did not only include RCTs but also cohort studies. More than 190 different tools exist for risk of bias evaluation within studies (14), and the recommended tool NOS was used for observational studies. It is, however, difficult to deduce each individual study’s weaknesses from a score on a scale. Therefore, risk of bias assessment is a considerable limitation when observational studies are used in systematic reviews. Studies in this review were all relatively small, the biggest study including 308 patients. Due to the small sample sizes and heterogeneity between studies, a meta-analysis was not relevant. Instead, data were pooled and a chi-square test was performed. This may also be regarded as a limitation but was the only possible solution to reach a clinically relevant outcome.
In conclusion, LC should optimally be performed within the first 24 h of ERCP, and at least within 3 days, in order to decrease risk of conversion to laparotomy as well as perioperative complications. If local logistics permit same-session ERCP and LC, this could be a good option with low rates of conversions and complications. A routine of postponing LC to a period of 2
Footnotes
Acknowledgements
C.F. and J.P.R. shared first authorship as both authors contributed equally to the study.
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.