
Abstract
Background and Aims:
Abdominal aortic aneurysm is a degenerative vascular pathology with high mortality due to its rupture, which is why timely treatment is crucial. The current single-center retrospective study was undertaken to analyze short- and long-term all-cause mortality after operative treatment of abdominal aortic aneurysm and to examine the factors that influence outcome.
Material and Methods:
The data of all abdominal aortic aneurysm patients treated with open repair or endovascular aneurysm repair in 2004–2015 were retrospectively retrieved from the clinical database of Tartu University Hospital. The primary endpoint was 30-day, 90-day, and 5-year all-cause mortality. The secondary endpoint was determination of the risk factors for mortality.
Results and Conclusion:
Elective abdominal aortic aneurysm repair was performed on 228 patients (mean age 71.8 years), of whom 178 (78%) were treated with open repair and 50 (22%) with endovascular aneurysm repair. A total of 48 patients with ruptured abdominal aortic aneurysm were treated with open repair (mean age 73.8 years) at the Department of Vascular Surgery, Tartu University Hospital, Estonia. Mean follow-up period was 4.2 ± 3.3 years. In patients with elective abdominal aortic aneurysm, 30-day, 90-day, and 5-year all-cause mortality rates were 0.9%, 2.6%, and 32%, respectively. In multivariate analysis, the main predictors for 5-year mortality were preoperative creatinine value and age (p < 0.05). In patients with ruptured abdominal aortic aneurysm, 30-day, 90-day, and 5-year all-cause mortality rates were 22.9%, 33.3%, and 55.1%, respectively. In multivariate analysis, the risk factors for 30-day mortality in ruptured abdominal aortic aneurysm were perioperative hemoglobin and lactate levels (p < 0.05). According to this study, the all-cause mortality rates of elective abdominal aortic aneurysm and ruptured abdominal aortic aneurysm at our hospital were comparable to those at other centers worldwide. Even though some variables were identified as potential predictors of survival, the mortality rates after ruptured abdominal aortic aneurysm remain high. Early diagnosis, timely treatment, and detection of the risk factors for abdominal aortic aneurysm progression would improve survival in patients with abdominal aortic aneurysm.
Introduction
Abdominal aortic aneurysm (AAA) is a complex pathology with a high mortality rate (around 80%) (1) due to its complication, AAA rupture, which is why timely treatment is crucial. Owing to the amelioration of intensive care units and introduction of endovascular aneurysm repair (EVAR), in-hospital mortality in elective abdominal aortic aneurysm (eAAA) patients has declined greatly over time and has been reported to be around 1%–3% (1,2). Despite remarkable improvements in short-term survival rates after surgical repair of both eAAA and ruptured abdominal aortic aneurysm (rAAA) during the last 50 years, the long-term survival rates remain relatively constant: the 5-year crude survival rate after eAAA repair is around 70% (2–4) and after rAAA repair around 40% (4). However, the launching of an AAA screening program has been associated with a significant reduction in AAA-specific mortality in Sweden (5).
Current treatment guidelines recommend definite treatment by EVAR or open repair (OR) for AAAs with a maximum diameter larger than 5.5 cm for men and larger than 5.2 cm for women, or rapidly growing (>10 mm/year) or symptomatic AAAs (6). Patients should undergo eAAA repair only if the risk of rupture outweights the risks from surgery. However, management of small AAA remains controversial (7). Non-surgical treatment of AAA includes quitting smoking, appropriate management of comorbidities affecting the cardiovascular system, and moderate physical activity, which could limit the expansion rate of AAA (6).
The availability of less invasive methods (EVAR) has made it possible to treat patients who are older and/or have more comorbidities. This might explain why there has been a lack of improvement in long-term survival rates (3). Studies have shown that in patients undergoing both eAAA (1,8–10) and rAAA (8,11,12) repair, EVAR yields lower 30-day mortality rates than OR. The OR procedure is more strenuous and has quite high operative mortality (4%–10%) (1). Therefore, older (2) patients with more comorbidities (8,11,13) are recommended to undergo EVAR if anatomically feasible. However, EVAR has not shown better results in long-term survival rates and is associated with a higher number of late ruptures (9) aneurysm-related mortality (14), and reinterventions (1,9).
Smoking (9,15), comorbidities (2,13), and older age at surgery (2,3,9,13,15) have been found to decrease both in-hospital and 5-year survival rates. Reduced 5-year survival is also associated with the maximal diameter of AAA at the time of repair (3). Improvements in long-term mortality have been linked with preoperative administration of certain drugs such as statins and aspirin (2,13) and with perioperative administration of β-blockers. This can be related to the cardioprotective effect of these drugs and hence a decrease in myocardial complications (2,11,13,15).
We have carried out the first single-center-based study on short- and long-term mortality rates and mortality predictors in patients undergoing eAAA and rAAA surgical repair at Tartu University Hospital, Estonia.
Patients and Methods
Subjects and Study Design
The medical records of the AAA patients undergoing OR or EVAR between 1 January 2004 and 31 December 2015 were retrospectively reviewed. We collected and analyzed patient demographics, comorbidities, medications, imaging studies, and pre-, peri-, and postoperative data from archived hospital records on paper and from records stored with the hospital’s online system of patients; 30-day, 90-day, 1-year, 2-year, 3-year, 4-year, and 5-year survival data were documented from the national registry. This study was carried out in accordance with the Declaration of Helsinki of the World Medical Association and the Ethics Committee on Human Research of the University of Tartu (Licence No. 262/T-8).
All operations were performed at a single institution by fellowship-trained vascular surgeons; the EVAR procedures were performed by interventional teams consisting of a fellowship-trained vascular surgeon and an interventional radiologist. Patients were considered to meet the criteria for surgical treatment if the maximum AAA diameter was ≥5.5 cm for men and ≥5.2 cm for women; if AAA had grown ≥0.5 cm during the last 6 months or the patient had symptomatic or rAAA.
The primary outcome measure of the study was all-cause mortality rates (30-day, 90-day, and 5-year) after OR and EVAR in patients with eAAA and rAAA. The secondary outcome measure was establishment of the factors related to mortality.
Statistical Analysis
Data were collected and analyzed using the software R, version 3.3.1 for Windows. All continuous variables were compared with the Mann–Whitney U test except for age where an unpaired t-test was performed to compare the eAAA and rAAA patient groups. Continuous variables are described by medians (interquartile range (IQR)) except for age, which is expressed as mean (standard deviation). Categorical data are presented as the number (%) of patients and was analyzed using the chi-square test. The Kaplan–Meier estimate was used to assess the difference in short- and long-term postoperative mortality between the eAAA and rAAA patients using the log-rank test. Univariate Cox proportional hazard models were used to determine the potential risk factors related to the prognosis of AAA repair. Joint impacts of factors were estimated using the multivariate Cox model, adjusted for gender, and presented as hazard ratios (HRs) with 95% confidence intervals (CIs); p < 0.05 was considered statistically significant.
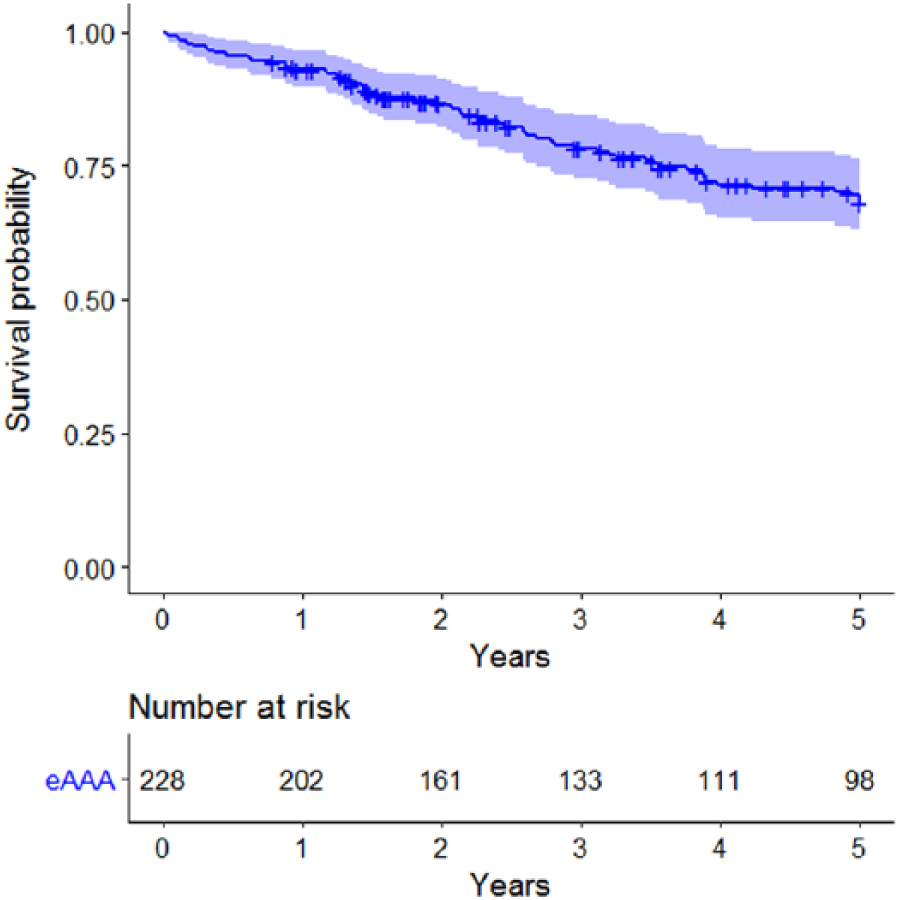
Kaplan–Meier plots showing the survival after eAAA repair.
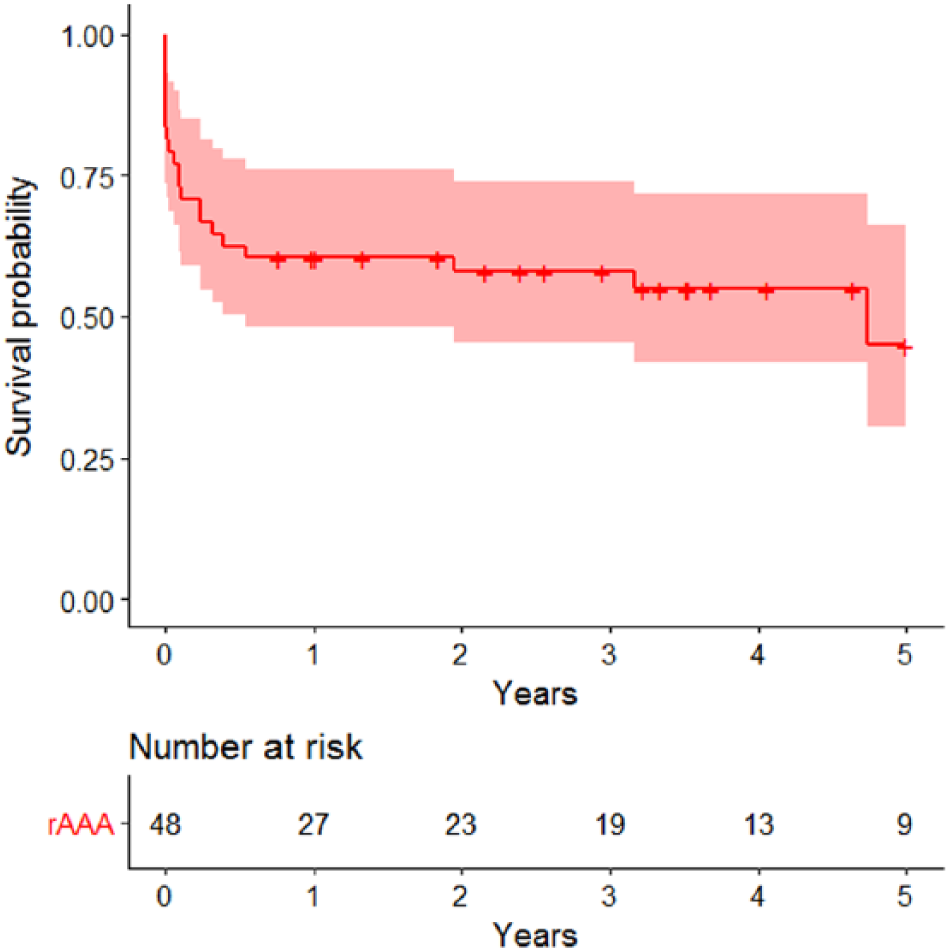
Kaplan–Meier plots showing the survival after rAAA repair.
Results
The eAAA surgical repair (including 50 EVAR procedures) was performed on 228 patients. EVAR was performed since November 2011. All 48 patients with rAAA were treated with OR. The follow-up period ended 22 September 2016 (mean follow-up: 4.2 ± 3.3 years). The baseline characteristics of the eAAA and rAAA patients are presented in Tables 1 and 2.
Baseline characteristics of the study population.

SD: standard deviation; IQR: interquartile range; eAAA: elective abdominal aortic aneurysm; rAAA: ruptured abdominal aortic aneurysm.
Pre- and perioperative markers of the study population.
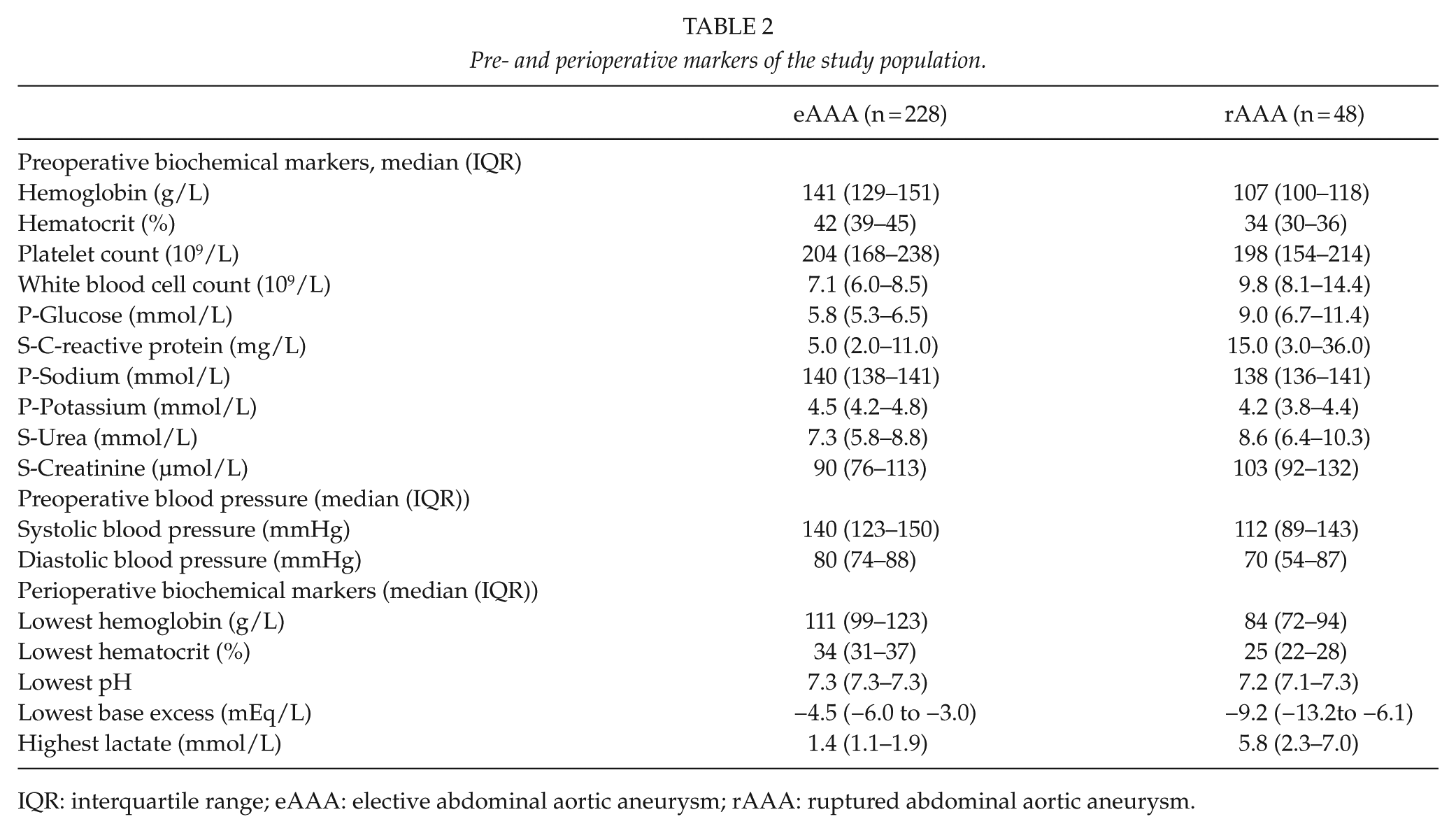
IQR: interquartile range; eAAA: elective abdominal aortic aneurysm; rAAA: ruptured abdominal aortic aneurysm.
For the eAAA patients, the 30-day, 90-day, and 5-year mortality rates were 0.9%, 2.6%, and 32%, respectively (Fig 1). The 30-day, 90-day, and 5-year mortality rates of the rAAA patients were 22.9%, 33.3%, and 55.1%, respectively (Fig 2). For all observed follow-up periods (overall; 30 days; 90 days; and 1, 2, 3, 4, and 5 years), the eAAA patients showed a better survival rate (all p values <0.002). Comparison of the eAAA patients undergoing OR and those undergoing EVAR revealed no difference (data not shown, all p values >0.2).
Multiple regression analysis showed that higher preoperative creatinine levels and older age were independently positively associated with higher 5-year mortality rates in patients with eAAA (Table 3). Because only two deaths occurred during 30 days after eAAA repair, it was not reasonable to estimate predictors of short-term mortality.
Multiple regression analysis of variables associated with 5-year mortality of eAAA.
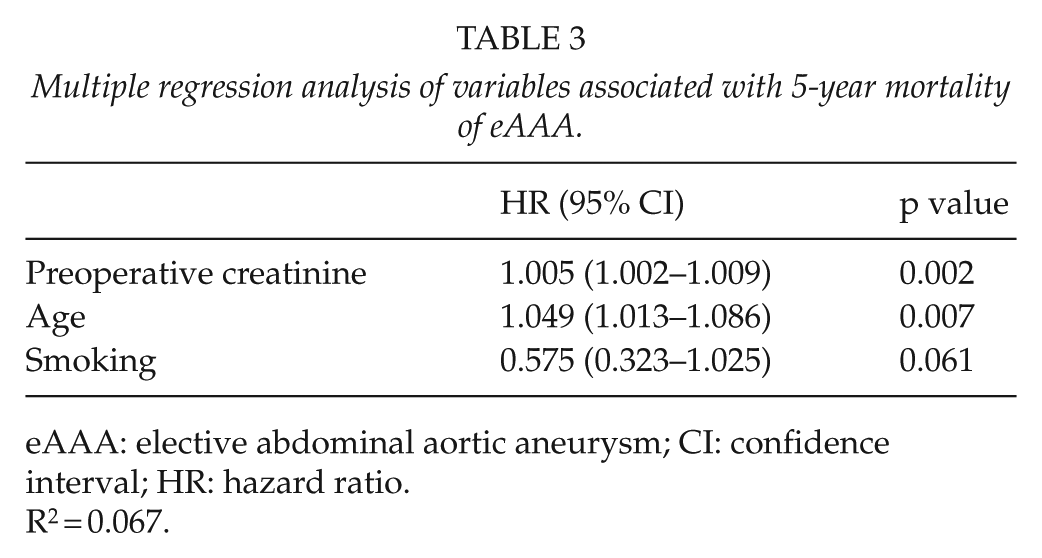
eAAA: elective abdominal aortic aneurysm; CI: confidence interval; HR: hazard ratio.
R2 = 0.067.
For the rAAA patients, independent risk factors of all-cause 30-day mortality were perioperative lowest hemoglobin and highest lactate levels (Table 4), but 5-year mortality risk factors were not detected.
Multiple regression analysis of variables associated with 30-day mortality of rAAA.
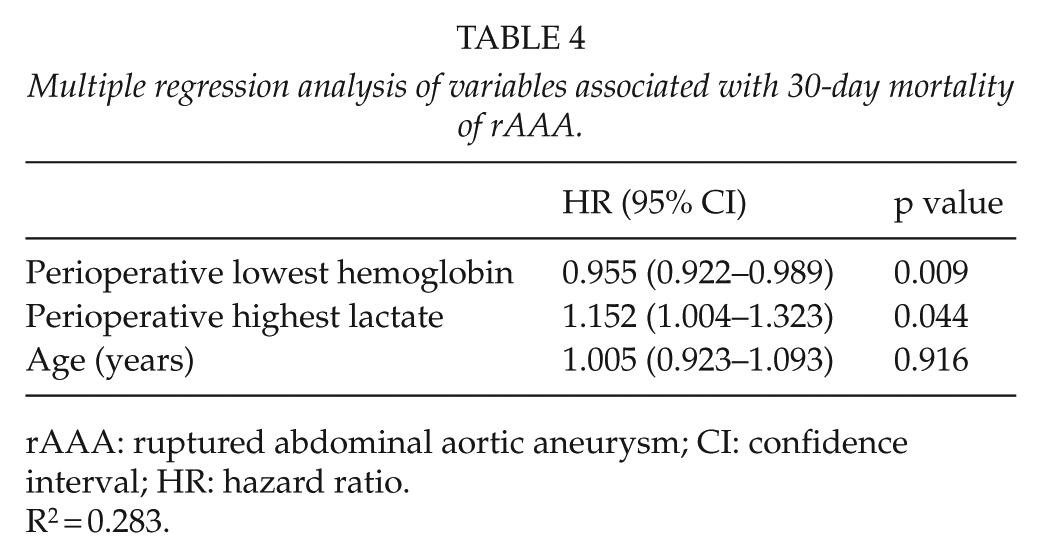
rAAA: ruptured abdominal aortic aneurysm; CI: confidence interval; HR: hazard ratio.
R2 = 0.283.
Discussion
This study is the first to evaluate short- and long-term all-cause mortality and the factors that may influence prognosis after surgical repair of eAAA and rAAA in Estonia. All patients operated at Tartu University Hospital accounting for more than half of the AAA operations performed nationally. With some limitations, the results could be generalized for the entire country.
Our short- and long-term results are in good agreement with previous data from different countries. Reports from Sweden, England, and the United States show 30-day or in-hospital mortality of 0.9%–2.6% after eAAA repair (5,16). Short-term (30-day or in-hospital) mortality rate in the range of 25%–65.9% after rAAA were reported in several countries from Europe, the United States, Canada, and Asia (17–20). However, different discharge policies between hospitals and countries may be the cause of variations in in-hospital mortality rates. Several studies from Europe, the United States, Australia, and Asia have demonstrated 3- to 5-year survival rates of 70%–80% in eAAA (2–4,16) and 38.6%–46.3% in rAAA (4,17). Timely repair of the abdominal aorta prevents its rupture and will hence reduce aneurysm-related mortality. Less-invasive EVAR is associated with lower short- and long-term mortality in AAA patients (21). Yet previous studies did not find improvement in long-term outcomes in rAAA (22) or eAAA (14) patients treated with EVAR. With the improvement in intensive care, many patients with rAAA do survive the early postoperative period but fail to fully recover. This is shown by the fact that for these patients, mortality is high already 90 days after surgery (4,17).
In our study, rAAA mortality after 90 days and after 5 years was 33.3% and 55.1%, respectively. Similar results were obtained in Sweden where the 90-day mortality of rAAA was 33.4% and 5-year mortality was 53.7% (17). These results are significantly better than those obtained in England (44% and 61.4%, respectively). Poor outcome in England versus Sweden is partially related to the more extensive use of EVAR and the larger proportion of patients managed in teaching hospitals in Sweden. In both countries, EVAR resulted in better outcomes than OR. Still, all rAAA patients in our study were treated by OR and the case load of our hospital as a teaching hospital is small.
Our study demonstrated that higher long-term mortality for eAAA patients was associated with preoperative higher creatinine value and older age, whereas smoking was an almost significant factor. Older age has been associated with poorer survival rates (2,3,13,23) and smokers have been found to have a significantly higher risk of AAA (24,25) and ruptures (26). Higher prevalence of acute kidney injury after rAAA repair has previously been demonstrated in patients with elevated preoperative serum creatinine value (27).
AAA is more prevalent among men than women but women have a higher risk of ruptures. In our study, 12 (25%) of the 48 patients who had a rAAA were women. Our results showed a trend (data not shown) for the female gender to be a risk factor in the eAAA patients undergoing OR. Previous research also shows that 5-year survival rates are lower for women compared with men in both eAAA and rAAA patient groups (4) Women are also more sensitive to the risk effects caused by smoking (24)
The finding of this study that perioperative lower hemoglobin level and higher lactate level were independent determinants of rAAA mortality was quite expected, as hemorrhagic shock is a significant contributor to prognosis. Patients of vascular surgery often experience cardiovascular problems during surgery. The fact that beta-blockers have been found to reduce the cardiac mortality of vascular patients casts doubt on catecholamine use during surgery. AAA repair is related to increased perioperative plasma catecholamine levels (28) which may potentiate the negative effect of noradrenaline administered during surgery.
The limitations of this study are its retrospective nature and the bias resulting from the co-variables that can be both confounders and causal intermediates. Because it is a single-center study, the case load is relatively small. During the study period, the proportion of EVAR was very low. Regrettably, there is no available data about aneurysm-related mortality and other death causes either.
It is well known that early diagnosis and timely repair of AAA will lead to favorable outcome. Our analysis revealed the factors responsible for total mortality of eAAA and rAAA cases in Estonia. The knowledge of the mortality-related factors could be a useful pre- or perioperative indicator for identifying high-risk patients.
Footnotes
Acknowledgements
We are indebted to Ester Jaigma for the linguistic revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by Personal Research Funding (PUT No 1169) from the Estonian Ministry of Education and Research.