
Abstract
Background and Aims:
To assess the accuracy of computed tomography in diagnosing acute appendicitis with a special reference to radiologist experience.
Material and Methods:
Data were collected prospectively in our randomized controlled trial comparing surgery and antibiotic treatment for uncomplicated acute appendicitis (APPAC trial, NCT01022567). We evaluated 1065 patients who underwent computed tomography for suspected appendicitis. The on-call radiologist preoperatively analyzed these computed tomography images. In this study, the radiologists were divided into experienced (consultants) and inexperienced (residents) ones, and the comparison of interpretations was made between these two radiologist groups.
Results:
Out of the 1065 patients, 714 had acute appendicitis and 351 had other or no diagnosis on computed tomography. There were 700 true-positive, 327 true-negative, 14 false-positive, and 24 false-negative cases. The sensitivity and the specificity of computed tomography were 96.7% (95% confidence interval, 95.1–97.8) and 95.9% (95% confidence interval, 93.2–97.5), respectively. The rate of false computed tomography diagnosis was 4.2% for experienced consultant radiologists and 2.2% for inexperienced resident radiologists (p = 0.071). Thus, the experience of the radiologist had no effect on the accuracy of computed tomography diagnosis.
Conclusion:
The accuracy of computed tomography in diagnosing acute appendicitis was high. The experience of the radiologist did not improve the diagnostic accuracy. The results emphasize the role of computed tomography as an accurate modality in daily routine diagnostics for acute appendicitis in all clinical emergency settings.
Introduction
Acute appendicitis is one of the most common causes of abdominal pain in emergency departments, and it is an indication for emergency abdominal surgery. The clinical diagnosis of acute appendicitis is challenging as every patient does not have typical clinical presentation and not every typical presentation is acute appendicitis. Several scoring systems have been created to aid the clinical diagnosis of acute appendicitis (1–3), but without preoperative imaging, the diagnostic accuracy of acute appendicitis varies between 76% and 80% for combined groups of male and female patients (4). Over the past decade, clinicians have increasingly relied on preoperative imaging in order to reduce the negative appendectomy rate (NAR), thus avoiding unnecessary surgery resulting in increased morbidity and expenses (5–7). As computed tomography (CT) has high sensitivity in diagnosing acute appendicitis, it has become the golden standard in right lower quadrant abdominal pain (8). CT in acute appendicitis can result in improved patient care and cost savings (5, 6, 9, 10).
The increased use of CT has been shown to decrease the NAR without increase in delayed or false-positive diagnosis (7, 11–13). In The Netherlands, NAR decreased from 19% in 2008 to 5% in 2011 after the implementation of the Dutch guideline for mandatory preoperative imaging for all suspected appendicitis patients (13, 14).
Appendectomy has been the standard treatment for acute appendicitis for over a century. The treatment paradigm of uncomplicated acute appendicitis may be changing as operative treatment may be unnecessary for the majority of uncomplicated appendicitis patients (15). To optimize and tailor the treatment for acute appendicitis, precise and accurate diagnostic tools such as CT are required.
As a part of our larger randomized controlled trial (RCT), we conducted a prospective study to investigate the capability and accuracy of the radiologist on call in diagnosing acute appendicitis using intravenous contrast-enhanced abdominal CT. We aimed to assess the accuracy of CT in emergency setting for the diagnosis of acute appendicitis and to clarify, particularly, the effect of the experience of the radiologist on the diagnostic accuracy.
Material and Methods
The present data were prospectively collected from our randomized APPAC trial comparing surgery with antibiotic therapy in the treatment of uncomplicated acute appendicitis.(15, 16) Six Finnish hospitals participated in the study, and the patients were enrolled from November 2009 to June 2012. Patients with clinical suspicion of acute appendicitis (clinical history, laboratory tests, and physical examination) were invited to participate in the APPAC trial and informed of the study protocol. After signed informed consent was obtained, a CT scan was performed to confirm the diagnosis. APPAC trial was approved by Turku University Hospital ethical committee (clinicaltrials.gov, NCT01022567).
The APPAC trial evaluated altogether 1379 patients for enrollment. Out of these, a total of 1065 patients were evaluated in this study. First, we included uncomplicated acute appendicitis patients enrolled in the APPAC trial and randomized to appendectomy (n = 273). Second, we included patients excluded from the APPAC trial based on either their age (under 18 years and over 60 years, n = 13) or a CT finding of a complicated acute appendicitis patients (n = 337). Third, we included also patients who declined to participate in the APPAC trial randomization after a CT scan finding of uncomplicated acute appendicitis (n = 91) and those with a normal CT finding or some other diagnosis on the CT scan (n = 351). APPAC patients randomized to antibiotic treatment (n = 257) were excluded from this study.
All abdominal CT scans were performed from diaphragm to the symphysis pubis using multi-detector row helical CT scanners (MDCT) with intravenous contrast medium. The radiation dose was evaluated to be approximately 5–7 mSv depending on the size of the patient. A number of different CT scanners were used, and axial section thickness evolved from 0.625 to 2.5 mm.
The CT images were preoperatively analyzed by the radiologist on call. A structured reporting template was used for identifying uncomplicated and complicated acute appendicitis, but otherwise no structured imaging reporting criteria were used. In this emergency setting, the radiologists on call were divided into experienced radiologists (consultants, at least 6 years of training) and inexperienced ones (residents, less than 6 years of training). The primary CT findings assessed as false-negative and false-positive were blindly reassessed by one body imaging radiologist (16 years of dedicated abdominal imaging experience) and one resident in radiology (3 years of experience in radiology). They were aware of the primarily false CT diagnosis, but were unaware of final surgical and histological diagnosis and also CT referral text. The reviewers evaluated both axial reconstructions and coronal reformatted images, as in primary situation. The preoperative and reassessed CT findings were compared with surgical and histopathological findings. As for the patients who had a normal CT finding or some other diagnosis on the CT scan, the final diagnosis was determined reviewing the medical records.
Uncomplicated acute appendicitis was considered present when the appendiceal diameter exceeded 6 mm with wall thickening and at least one of the following findings: abnormal contrast enhancement of the appendiceal wall, inflammatory edema, or fluid collections around the appendix. CT finding of complicated acute appendicitis included the presence of an appendicolith, possible free air around the appendix indicating perforation, or a periappendiceal abscess or suspicion of a tumor.
Statistical Analysis
Summary measurements are presented as mean with standard deviation (SD) unless other stated. Sensitivity, specificity, and positive and negative predictive values with 95% confidence intervals (95% CI) were calculated to assess diagnostic accuracy. Student’s t-test was used in between-group comparisons for continuous variables. Pearson χ2-test was used when comparing categorical data. We assumed experienced radiologists to have superior accuracy in establishing the correct diagnosis, and, therefore, one-sided p-value is presented when comparing the impact of experience, otherwise two-sided p-values are presented. Analyses were performed using SPSS for windows (IBM SPSS Statistics for Windows, Version 21.0, IBM Corp., Armonk, NY, USA; released 2012).
Results
Out of the 1065 patients, 714 had acute appendicitis and 351 had other diagnosis or a normal CT finding. The patients were 17- to 65-years old (mean 36.2, SD 12.7 years), 44.1% (n = 470) were female. Overall, there were 65.7% (n = 700) true-positive, 30.7% (n = 327) true-negative, 1.3% (n = 14) false-positive, and 2.3% (n = 24) false-negative cases. The sensitivity and the specificity of CT were 96.7% (95% CI, 95.1–97.8) and 95.9% (95% CI, 93.2–97.5), respectively. The rate of false CT diagnosis was 4.2% for experienced consultant radiologists and 2.2% for inexperienced resident radiologists (p = 0.071), as presented in Table 1. The age of the patients with a false and correct CT diagnosis was 35.0 and 36.9 years (p = 0.014), respectively; 5.5% of female patients and 2.0% of male patients had false CT diagnosis (p = 0.002).
The accuracy of the CT diagnosis in suspected acute appendicitis in emergency setting (n = 1065).
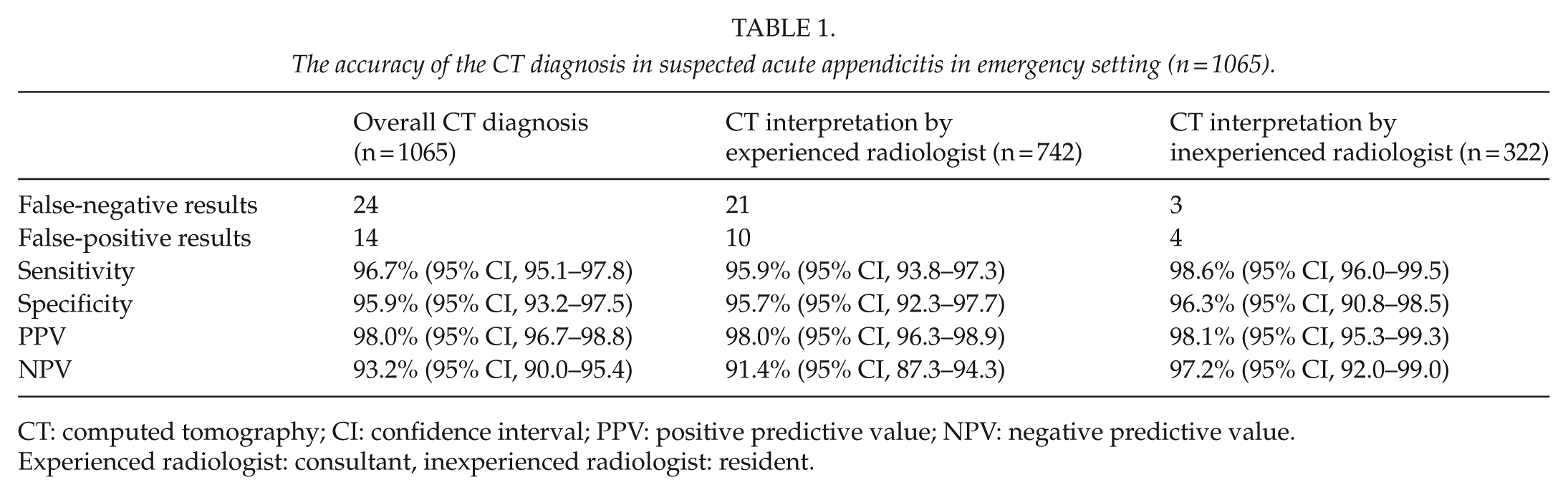
CT: computed tomography; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
Experienced radiologist: consultant, inexperienced radiologist: resident.
The reassessments of the primarily false-negative and false-positive CT findings (n = 38) by one body imaging radiologist and one radiology resident are shown in Table 2. Out of these 38 re-evaluated CT scans, 21 were correctly interpreted by both radiologists. In eight of the cases, the CT diagnosis was incorrect after all three interpretations. Six of these were false-positive and two were false-negative cases. In nine cases, one radiologist had accurate and the other inaccurate interpretation.
The primary CT analysis in suspected acute appendicitis (n = 1065) and the reassessed CT analyses of false-positive (n = 14) and false-negative (n = 24) cases by body imaging radiologist and resident.
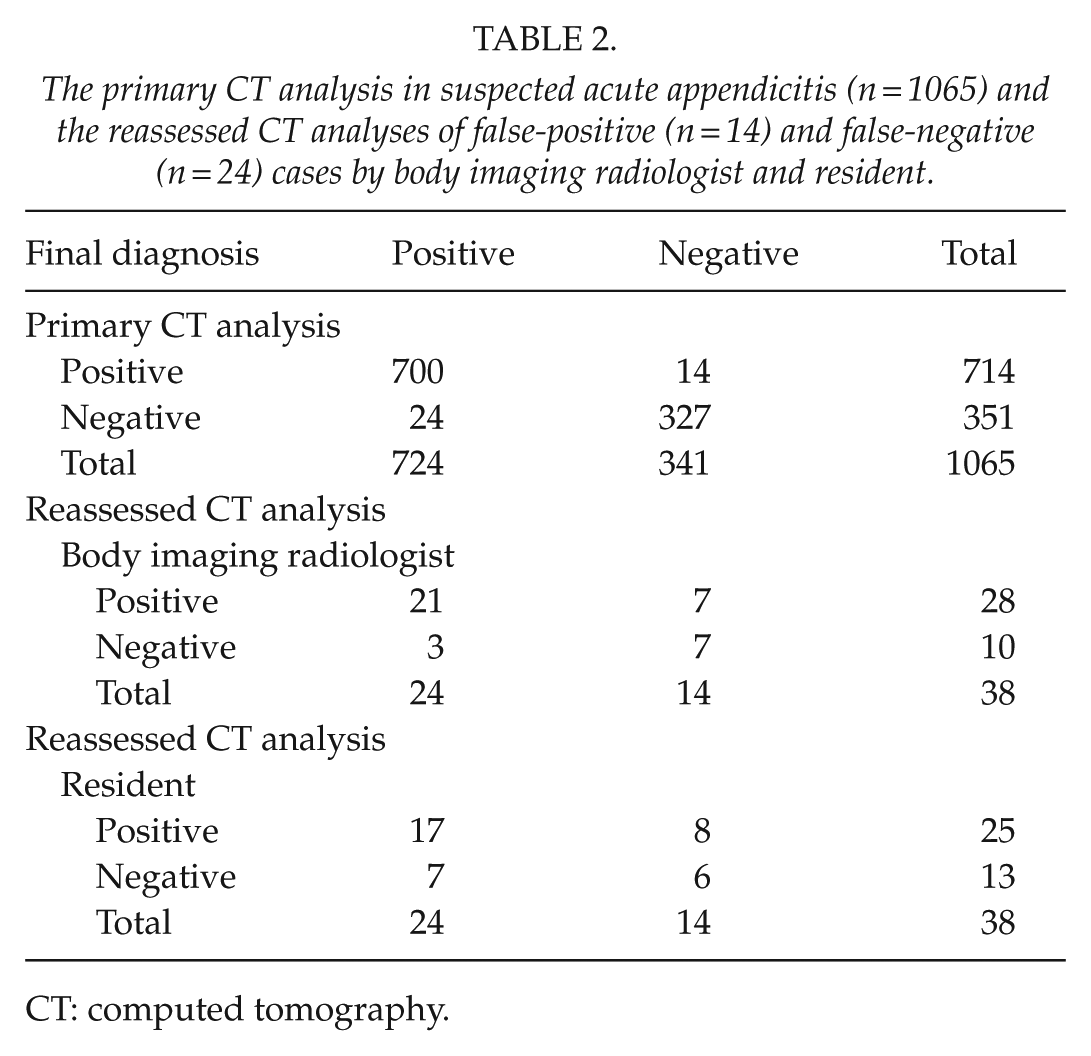
CT: computed tomography.
Discussion
Acute appendicitis requires around-the-clock diagnostics. Our study showed high sensitivity and specificity (96.7% and 95.9%, respectively) in a clinical emergency setting, and the experience of the radiologist did not affect the diagnostic accuracy. Although the interpretation of abdominal CT during regular office hours is routinely performed by specialist in radiology or at least their consultation is at hand, in an emergency setting, the expertise of the radiologist on call is versatile. There are studies that have shown remarkable influence of expertise on the interpretation of CT images for acute appendicitis (17–19). There are also contradictory results, where no significant difference in the accuracy of CT diagnosis has been shown between inexperienced and experienced radiologists (20). In our study, the primary CT analysis by the on-call radiology staff resulted in as few as 24 false-negative and 14 false-positive CT interpretations out of the 1065 CT examinations. The reassessment of these 38 challenging cases by the body imaging radiologist resulted in three false-negative and seven false-positive CT analysis, and, respectively, seven and eight for resident reassessment. Based on our study results, routine reassessment is not necessary, but the somewhat smaller number of mistakes by the body imaging radiologist in the reassessment analysis may support the reassessment of possible unclear cases during working hours by the body imaging radiologist. The limitations in our study include the retrospective reassessment of CT scans and the fact that despite the blinded reassessment, the body imaging radiologist and the resident knew they were evaluating false-positive or false-negative CT interpretations.
The results of this study indicated that the accuracy of CT in the diagnosis of acute appendicitis was high in clinical emergency setting, and the experience of the radiologist did not improve the diagnostic accuracy, emphasizing the role and feasibility of CT in daily routine diagnostics for acute appendicitis in all clinical emergency settings. The optimal method for the diagnosis and treatment of acute appendicitis remains a challenge. Several studies have shown that the majority of patients with uncomplicated acute appendicitis can be safely and effectively treated with antibiotics alone (15, 21, 22). At the same time, there is growing need to reduce NAR as although appendectomy is generally well tolerated, it is still a surgical intervention and can be associated with postoperative morbidity (23, 24). Balancing the NAR and the perforated appendicitis rate is the goal of good patient treatment. In complicated acute appendicitis, perforation in most cases happens before admission and can seldom be prevented during hospital stay (25). CT has been criticized of causing a possible delay in diagnosis, but it has been shown that CT does not increase the time spent in the emergency department and CT is not associated with an increased appendiceal perforation rate (26).
As the use of CT does not impair the prognosis combined with the desired low NAR, the need for differential diagnosis within appendicitis for treatment optimization all together account for and support the increased use of imaging modalities. CT with its high specificity and sensitivity has become the golden standard imaging modality for suspected acute appendicitis since it has been shown to decrease the NAR to even as low as 1.7% compared with 10%–20% NAR in patients without preoperative imaging (7, 13, 27). The concern regarding CT imaging is the radiation exposure (14, 28, 29). Although the issue is debatable, the incidence of acute appendicitis is high in adolescents and young adults, emphasizing the need for reducing the radiation dose (30, 31). Two Asian low-dose CT studies regarding the diagnosis of acute appendicitis have shown promising results (32, 33); in these recent studies, contrast-enhanced low-dose CT was not inferior to contrast-enhanced standard-dose CT in suspected acute appendicitis (32, 33). The radiation dose for CT in the diagnosis of appendicitis should be optimized following the “as low as reasonably achievable” principle. Kim et al. (33) showed that the low-dose and standard-dose CT techniques did not differ in the radiologists’ diagnostic confidence in the diagnosis of acute appendicitis, appendiceal visualization, or sensitivity for suggesting an alternative diagnosis. Future studies will show whether low-dose radiation CT has a role as the first-line imaging test for acute appendicitis.
Out of the CT criteria for acute appendicitis, the appendicular enlargement (>6 mm in diameter) has been shown to be the most specific CT finding of acute appendicitis with the highest sensitivity and negative predictive value (34, 35). In most cases, identification of an enlarged appendix with contrast enhancement of the wall and periappendicular fat stranding allowed for the definitive diagnosis of acute appendicitis, and other signs were additional findings (35). In our study, 38 patients out of 1065 had false CT diagnosis, and in 65.9% of these cases, the diameter of the appendix was not identified or registered preoperatively. At the same time, none of the acute appendicitis diagnosis was missed in cases with appendiceal diameter exceeding 15 mm. Optimization of CT interpretation is necessary to further enhance diagnostic accuracy of CT diagnosis with suspected acute appendicitis. Although appendiceal enlargement is of utmost importance, relying on the appendix size alone may lead to misdiagnosis and mismanagement, emphasizing the role of all criteria combined. In our study, prospective collection of these other parameters was, unfortunately, not adequate enough to make further analysis.
In conclusion, the accuracy of CT in the diagnosis of acute appendicitis in our study was high. The experience of the radiologist did not improve the diagnostic accuracy. These results emphasize the role of CT as the golden standard in daily routine diagnostics for acute appendicitis in practice in all clinical emergency settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Written consent was obtained from all the participants and trial was approved by Turku University Hospital ethical committee.
Funding
This study was supported by a Turku University Hospital Government Research Grant (TYKS EVO Foundation). Dr Salminen has received personal fees for lectures from Merck and Roche.