
Abstract
Background and Aims:
To evaluate simple tumor characteristics (renal tumor diameter and parenchymal invasion depth) compared with more complex classifications, that is, Renal Tumor Invasion Index (RTII) and Preoperative Aspects and Dimensions Used for an Anatomical classification, in predicting the type of nephrectomy (radical vs partial) performed.
Material and Methods:
A total of 915 patients who had undergone either partial nephrectomy (n = 388, 42%) or radical nephrectomy (n = 527, 58%) were identified from the Helsinki University Hospital kidney tumor database between 1 January 2006 and 31 December 2014. Tumor maximum diameter and depth of invasion into the parenchyma were estimated from computed tomography or magnetic resonance imaging images and compared with Preoperative Aspects and Dimensions Used for an Anatomical and Renal Tumor Invasion Index. Logistic regression and receiver operating curves were used to compare the parameters at predicting the type of nephrectomy.
Results and conclusion:
All the anatomical variables of receiver operating curve/area under the curve analyses were significant predictors for the type of nephrectomy. Parenchymal invasion (area under the curve 0.91; 95% confidence interval, 0.89–0.93), RTII (area under the curve 0.91; 95% confidence interval, 0.89–0.93), and diameter (area under the curve 0.91; 95% confidence interval, 0.89–0.93) performed significantly better than Preoperative Aspects and Dimensions Used for an Anatomical classification (area under the curve 0.88; 95% confidence interval, 0.85–0.89). In multivariable analysis, invasion depth was the best predictor of nephrectomy type (percentage correct, 85.6%). Addition of one anatomic parameter into the model of non-anatomical cofactors improved the accuracy of the model significantly, but the addition of more parameters did not. Parenchymal invasion depth and tumor diameter are the most accurate anatomical features for predicting the nephrectomy type. All potential anatomical classification systems should be tested against these two simple characteristics.
Keywords
Introduction
Oncological outcomes of partial nephrectomy (PN) and radical nephrectomy (RN) are similar, but PN preserves kidney function better (1) and may reduce overall mortality compared to RN (2, 3). The European Association of Urology guidelines recommend nephron sparing surgery for patients with T1a tumors, and this should, therefore, be the preferred option for T1b tumors whenever feasible (4). The pattern of practice for nephrectomies has changed dramatically over recent years and now favors PN (5). Active surveillance and renal tumor ablation have also emerged as alternative treatment options, but these currently lack long-term evidence for oncological safety (6).
In addition to the characteristics of the renal tumor and vascular anatomy, patient comorbidity, renal function, and surgeon’s pattern of practice, alone or in any combination, may have an impact on the choice of PN versus RN (7). A total of 10 anatomic scoring indices have been introduced since 2009 to classify kidney tumors in relation to the surgical complexity, perioperative complications, or renal function. Renal nephrometry (RENAL) (8) and Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) classification (9) are regarded as the current standard reference classifications. These classifications have been externally validated to some extent and were used in several studies (10). The zonal NePhRO scoring system (11) and the surgical approach renal ranking (SARR) (12) may be regarded as modifications of RENAL and PADUA.
In contrast to RENAL and PADUA, anatomic descriptions of renal tumors, such as the Centrality Index (13) and the Renal Tumor Invasion Index (RTII) (14), focus on tumor invasion as the primary determinant of complexity. Diameter-axial-polar (DAP) nephrometry is a refined and integrated version of the RENAL and the Centrality Index scoring systems (15). The renal tumor contact surface area (CSA) takes into account the invasion extent and diameter and uses computed tomography (CT) image rendering software to estimate the area of the tumor surface in contact with the normal parenchyma (16). Similarly, resected and ischemic volume (RAIV) was recently launched as a novel mathematical model to predict the severity of functional reduction after PN (17). Finally, the number of renal columns invaded (NRC) was introduced to predict the perioperative outcome of PN (18).
Only a few comparative studies on anatomic classifications exist and no single classification index has become accepted as the gold standard for clinical use or for scientific stratification (19, 20). The aim of this study was to evaluate how the two simple tumor characteristics of diameter and parenchymal invasion depth compared with more complex classifications of RTII and PADUA in predicting the type of nephrectomy performed. Furthermore, if PADUA and RTII provide no additional advantage over the simple diameter and invasion depth classifications, then the use of such complex measures could be questioned.
Material and methods
Cohort
The Ethics Committee of the Department of Surgery, Helsinki University Central Hospital, approved the following protocol for this study (DNRO176/13/03/02/2011). The Helsinki University Hospital kidney tumor database was searched to identify all consecutive patients (n = 1284) who had undergone either a partial or a RN because of a radiologically identified renal tumor from 1 January 2006 to 31 December 2014. A total of 369 (28%) out of 1284 patients were excluded from the cohort for the various reasons shown in Fig. 1. Conversions from PN to RN (n = 10) were included as radical nephrectomies in the study.
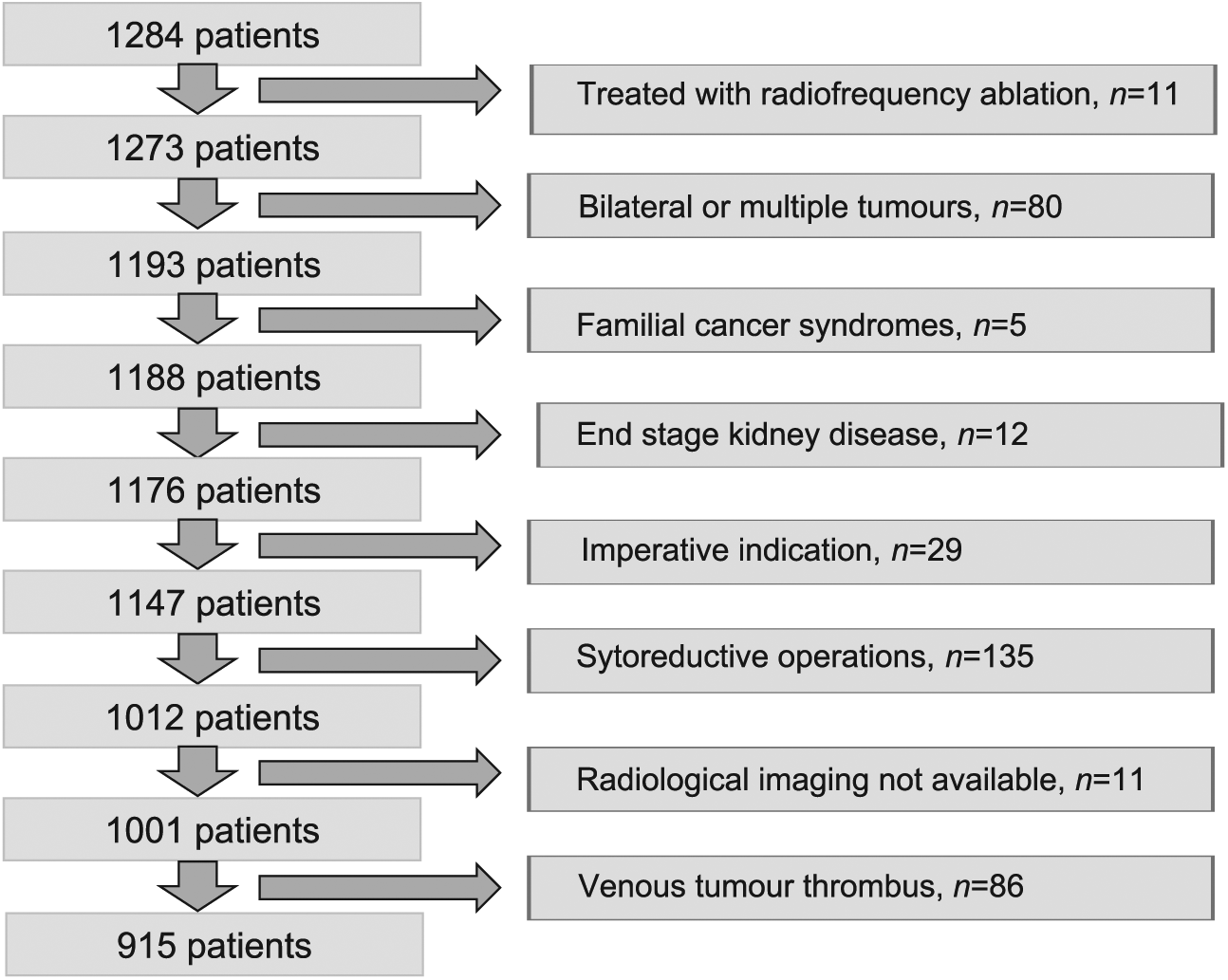
Flowchart of patient exclusions.
Preoperative Decision-Making
The type of nephrectomy and approach were ultimately decided upon by the primary surgeon by taking into account the anatomic features of tumor, renal functions, patient comorbidities and surgeons’ practice pattern. European Association of Urology Guidelines were used to guide the decision-making. Clinical multidisciplinary conferences were held weekly to mediate the decisions. CT or magnetic resonance imaging (MRI) images were nearly always available preoperatively. 3D reconstructions have occasionally been done since 2010, especially to clarify the vascular anatomy and the extent of the depth of invasion of tumors. No anatomic classifications were routinely used in clinical practice during the study period.
Surgery
Operations were performed or assisted by 26 consultant urologists. The treatment options in our institution during the study period were open PN, hand-assisted laparoscopic PN, robot-assisted PN, open RN, laparoscopic RN and hand-assisted laparoscopic RN. The two approaches that were considered for this analysis were laparoscopy (pure laparoscopy, robot-assisted laparoscopy, hand-assisted laparoscopy) or open surgery.
Demographic and Clinical Data
Clinical data were retrospectively obtained from the prospective tumor database and included: age, gender, non-age adjusted Charlson Comorbidity Index (CCI), presence of diabetes, presence of arteriosclerosis, presence of hypertension, American Society of Anesthesiologists (ASA) score, body mass index (BMI) and the year of the kidney surgery.
Tumor Anatomic Characteristics
The maximal diameter of tumor and the depth of parenchymal invasion from the renal cortex into the parenchyma toward the medulla of the kidney were measured by CT or MRI images taken in axial, coronal or sagittal planes, depending on the position of the tumor. PADUA and RTII classifications were assigned by one urologist (H.N.) to each tumor according to the original published methods (9, 14).
Analysis and Statistical Methods
Parametric continuous variables were expressed as means ± standard deviation (SD) and categorical variables as ratios (%). Comparisons between groups were made by the Student’s t-test for continuous variables and the Chi-square test was used for analyzing the categorical variables. Receiver operating curves (ROC) with areas under the curve (AUC) and 95% confidence intervals (CI) were calculated to compare the extent to which anatomic parameters were able to predict the type of nephrectomy. Multivariable regression analyses for PN were done using a backward stepwise likelihood ratio test. Only those variables that were significant (p < 0.01) in the univariable analysis were analyzed. Correlations between the various anatomic variables were assessed using Pearson’s correlation coefficient. All the anatomic variables were tested with a constant group of independent non-anatomic factors to see better the real impact of the models. The goodness of fit of the model was determined by expressing the observed results as a percentage of the expected results. A two-sided p < 0.05 was considered as statistically significant. The data were analyzed using SPSS software version 23 (IBM Corp., Armonk, NY, USA).
Results
The study group comprised 915 patients of whom 527 (58%) underwent RN and 388 (42%) underwent PN. The use of PN increased significantly from 25% in 2006–2008 to 50% in 2012–2014 (p < 0.001). The rate of PN for tumors of <40 mm in maximal diameter (T1a) increased significantly from 59% (49/83) in 2006–2008 to 87% (149/172) in 2012–2014 (p < 0.001). Similarly, the rate of PN for tumors <25 mm in invasion depth increased from 54% to 93%.
The univariable analysis revealed there was a significant association between the performance of PN and younger age, CCI ≥ 2, no presence of hypertension, higher baseline glomerular filtration rate (GFR), later year of surgery (Table 1). Similarly, lower diameter, lower invasion depth, lower PADUA score, and lower RTII were significantly associated with PN (Table 1). The ROC/AUC analysis found that invasion depth, diameter, and RTII predicted the type of operations significantly better than the PADUA classification (Fig. 2). Fig. 3 illustrates how tumor complexity is associated with nephrectomy type.
Preoperative clinical characteristics of patients undergoing partial or radical nephrectomy.
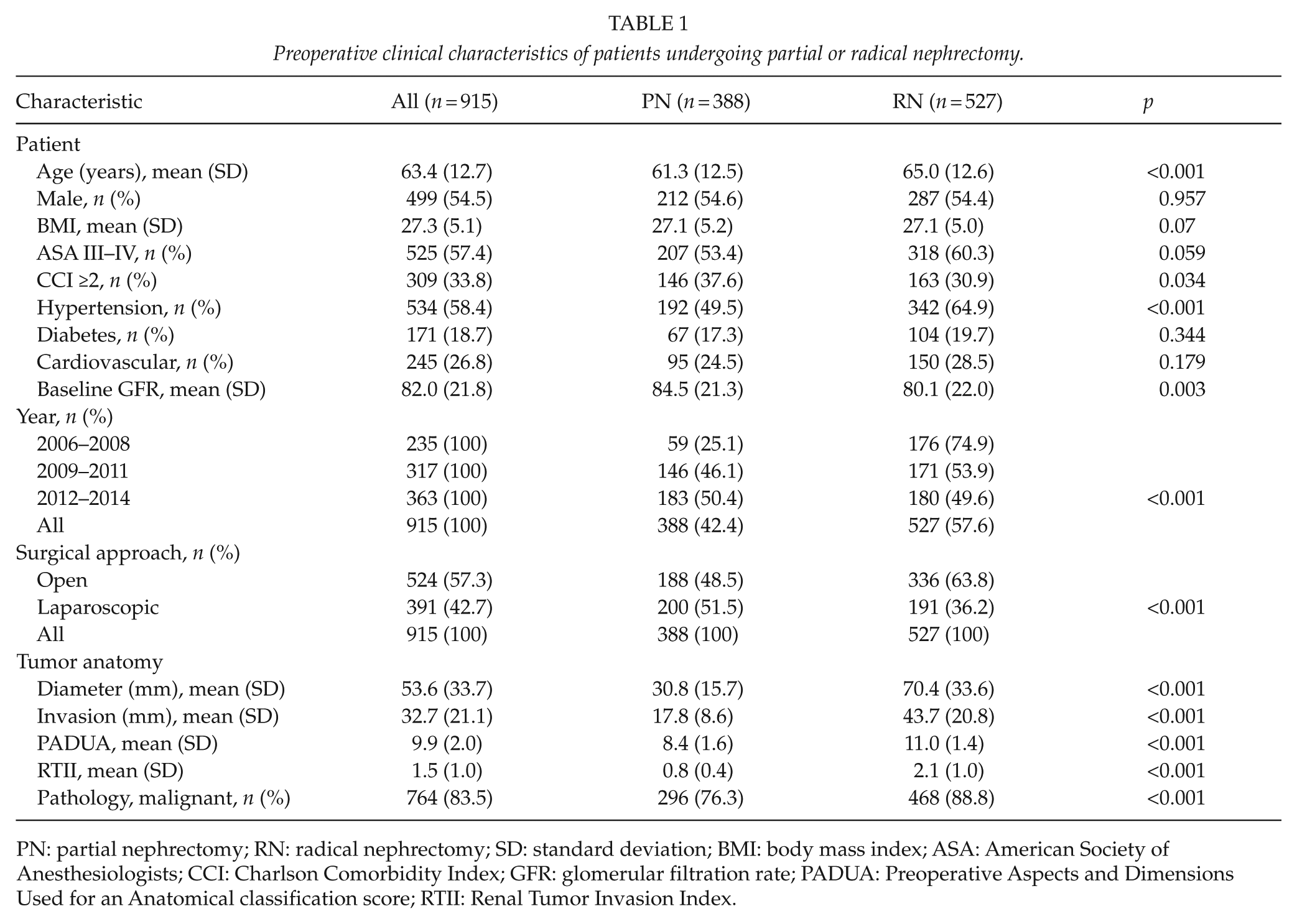
PN: partial nephrectomy; RN: radical nephrectomy; SD: standard deviation; BMI: body mass index; ASA: American Society of Anesthesiologists; CCI: Charlson Comorbidity Index; GFR: glomerular filtration rate; PADUA: Preoperative Aspects and Dimensions Used for an Anatomical classification score; RTII: Renal Tumor Invasion Index.
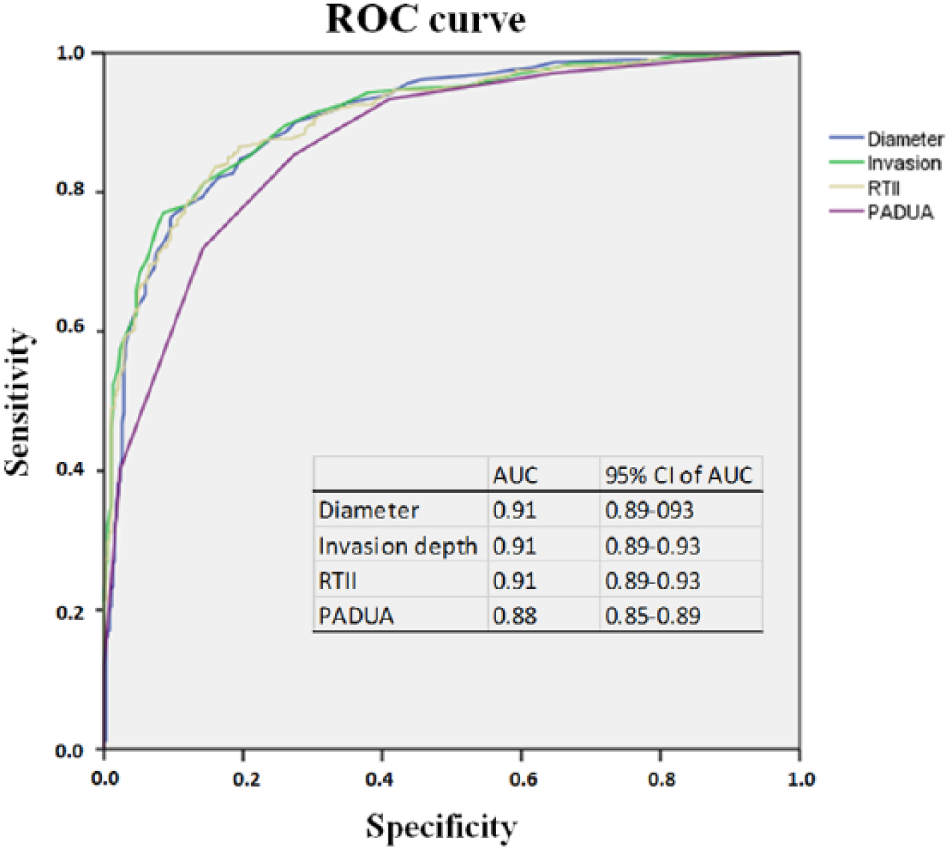
Receiver operating curves of anatomic variables that predict the type of nephrectomy.
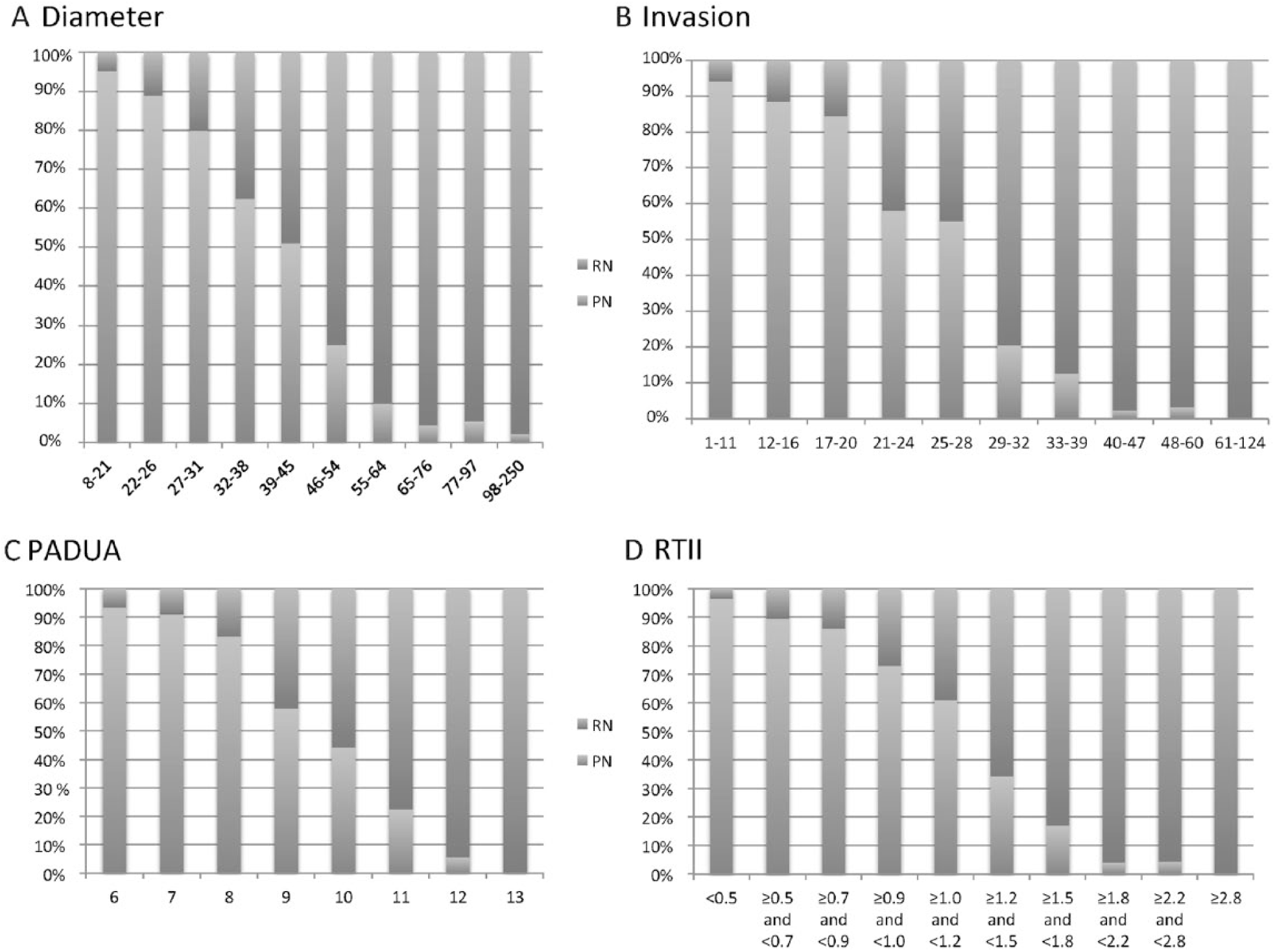
The type of nephrectomy by percentiles of anatomic variables of renal tumors.
The multivariable logistic regression model found that patients with lower age, no hypertension, later year of surgery, lower tumor invasion, smaller diameter, and lower PADUA score were more likely to undergo PN (Table 2). All anatomic variables correlated significantly when assessed with Pearson’s correlation coefficient: 0.81 for diameter and invasion, 0.76 for diameter and RTII, 0.62 for diameter and PADUA, 0.95 for invasion and RTII, 0.73 for invasion and PADUA, and 0.73 for RTII and PADUA. All correlations were significant (two-tailed p = 0.01). The strong correlations between the anatomic variables required that these variables were tested separately in various combinations with a constant group of independent non-anatomic cofactors (age, year of surgery, and hypertension) to understand better the real impact of the various anatomic factors (Table 3). The addition of “invasion” as a factor reinforced the model from 62.0% correct to 85.6% correct (+22.6%), which was significantly better compared to the addition of PADUA (+18.8%, p = 0.02), but similar to the addition of RTII (+21.4%) and diameter (+21.0%). In general, the addition of one anatomic parameter into the model was useful, but the addition of more parameters did not significantly improve the model.
Multivariable logistic regression analysis for performing partial nephrectomy.
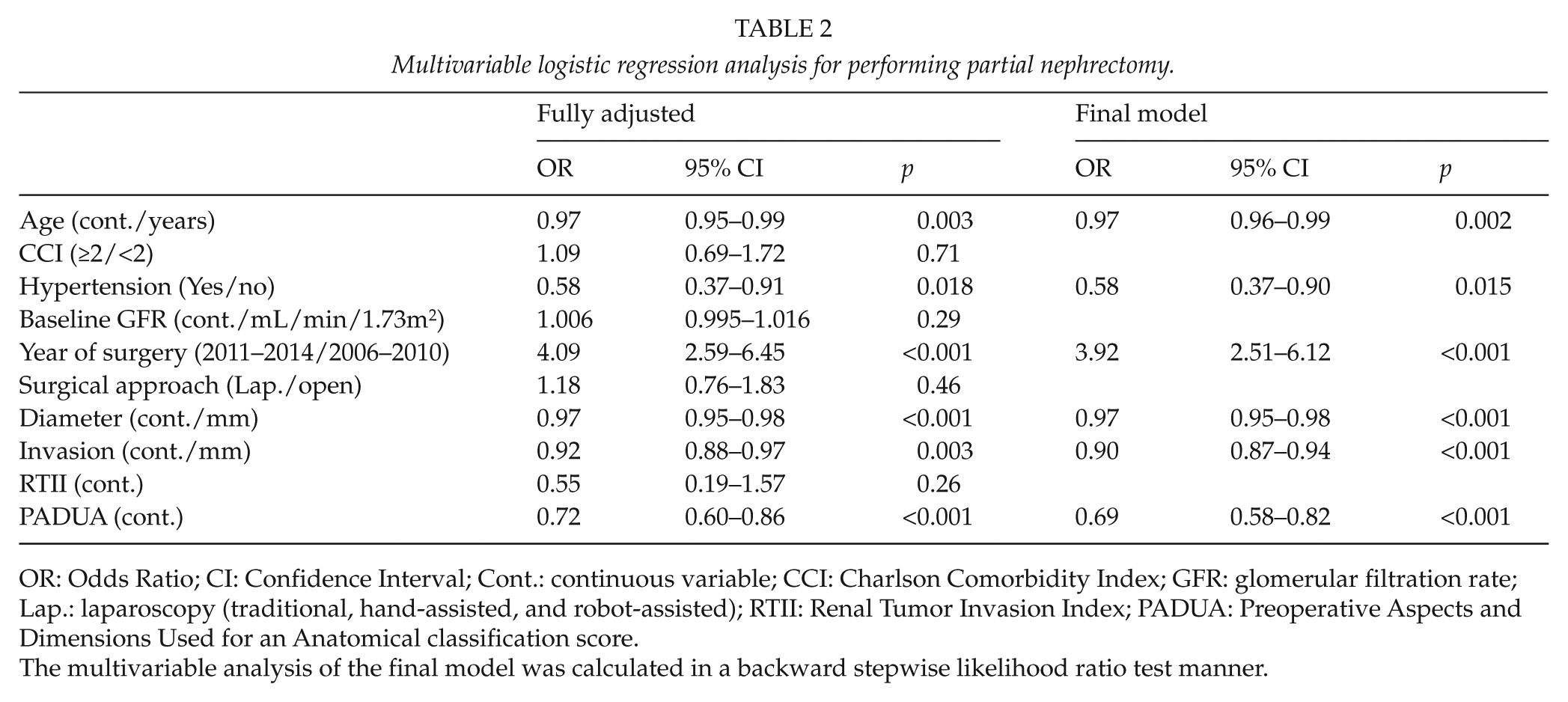
OR: Odds Ratio; CI: Confidence Interval; Cont.: continuous variable; CCI: Charlson Comorbidity Index; GFR: glomerular filtration rate; Lap.: laparoscopy (traditional, hand-assisted, and robot-assisted); RTII: Renal Tumor Invasion Index; PADUA: Preoperative Aspects and Dimensions Used for an Anatomical classification score.
The multivariable analysis of the final model was calculated in a backward stepwise likelihood ratio test manner.
Comparison of different multivariable regression models for the performance of partial nephrectomy.
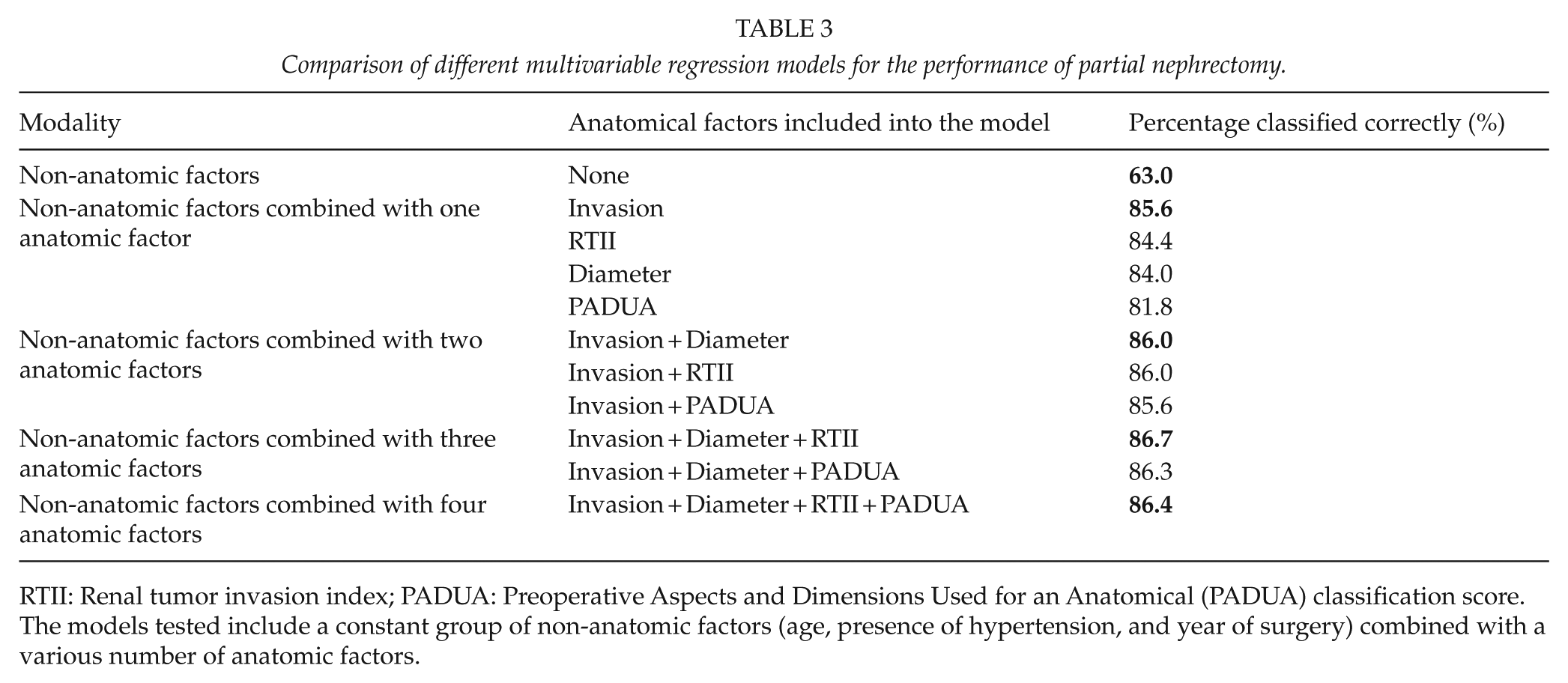
RTII: Renal tumor invasion index; PADUA: Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) classification score.
The models tested include a constant group of non-anatomic factors (age, presence of hypertension, and year of surgery) combined with a various number of anatomic factors.
Discussion
An abundance of complex anatomic classifications for assessing renal tumors has been proposed in recent years, but none have gained more widespread use in clinical practice than others. We show in this study that two simple characteristics of a renal tumor, invasion depth and its diameter, outperform the more complex classification PADUA score in the prediction of the type of nephrectomy in modern urological practice.
Renal tumor invasion depth has been regarded as an essential measure when planning kidney surgery for a long time. During the early years of elective PN, invasion depth was recognized as an important characteristic associated with surgical complexity (21). The extent of invasion of the tumor as a quantitative scaled parameter was also used before the era of modern anatomic classification scores. Simmons and Gill (22) in 2007 evaluated a cohort of 200 patients who were undergoing laparoscopic PN and reported a mean depth of parenchymal invasion to be 1.8 cm. Interestingly, the mean invasion depth in the present larger cohort was also 1.8 cm.
Variations of invasion depth are included in and form an essential part of all modern anatomic classification systems. Proximity of and relation to sinus fat or the collecting system are included in RENAL (8), PADUA (9), and NePhRO (11) as a classification factor. Extension of the involvement of renal parenchyma and relation with renal sinus are included in SARR (12). Similarly, invasion of renal columns is the sole criterion in NRC (18). The extent of invasion is included in RTII (14) and RAIV (17) as a scaled parameter, whereas in the Centrality Index (13), DAP (15), and CSA (16), invasion is the underlying idea behind these indices even though invasion as such is not directly measured.
Other studies have shown invasion to be associated with the choice of nephrectomy type (23), perioperative outcome including warm ischemia time (WIT) (24), operative time (24), postoperative complications (10, 24), urological complications (14), and postoperative renal function (17, 25). Therefore, many authors have recently emphasized the fundamental role of the parenchymal invasion depth (16, 17, 24).
We used the most elementary measurement of tumor invasion depth to predict practice pattern and showed that this simple parameter is superior to PADUA and similar to RTII as a predictor of the type of nephrectomy. Moreover, RTII does not seem to give additional value compared to the measurement of pure invasion depth.
The role of PADUA as a predictor of nephrectomy type, like many other more complicated classification score systems, may be attenuated by their less important factors, for example, exophytic/endophytic properties, rim position, and longitudinal position. Notably, large tumors are rarely totally endophytic. Modern ultrasonography also helps identify small totally endophytic tumors. The polar position of the tumor used to be favored for resection earlier, but modern techniques of enucleation and enucleoresections (26) may have changed the strategy.
Anatomic parameters of renal tumors that are associated with tumor location may function better in cohorts where only a single operative approach is applied (27, 28), but they may lose their predictive power in real life where different open, laparoscopic, and robotic approaches are used. A simple anatomic stratification, equally applicable to all surgical approaches of PN, could be useful.
The importance of tumor diameter is unquestionable: diameter is included in the TNM classification and has good prognostic value. Further still, the diameter of the tumor was the second most important anatomic characteristic to predict the type of nephrectomy in this study. Other studies have shown that the diameter of a tumor correlates with the type of nephrectomy (23, 29), WIT (27), perioperative conversions (30), estimated blood loss (24), operative time (24), postoperative complications (10), and postoperative GFR (20). In addition, tumor diameter is still the most commonly used concept in clinical communication and patient counseling.
A continuous evolution in practice patterns for renal tumor excision over time was clearly demonstrated in our cohort. Accordingly, the criteria of complex renal tumor anatomy also will change over time. Age, body habitus, comorbidity, and experience of surgeons in addition to tumor anatomy are crucial when deciding between PN and RN. At present, only diameter is included in international guidelines on renal tumor surgery. The European Association of Urology guidelines recommend nephron sparing surgery for patients with T1a tumors and this should also be the preferred option for T1b tumors whenever feasible (4). However, the implementation of these Guidelines to our clinical practice has taken some time mainly due to a large number of urologists involved in decision-making process. Since 2006, renal surgery has gradually been centralized to few specialized surgeons in our department. In our study, setting the ability to predict the nephrectomy type was tested in a real-life situation and therefore reflects current international practice patterns.
An anatomic classification has to be user-friendly and consistently reproducible to become a gold standard. In future, invasion could be used together with diameter for the main criteria to decide between the types of the nephrectomy. Our study demonstrates that practically all patients operated recently with tumor invasion depth less than 2.5 cm undergo PN, whereas most of patients with invasion depth over 3.0 cm will undergo RN.
Our study is retrospective in nature, but practice patterns can only be analyzed retrospectively. The imaging accuracy has continually improved, and the images obtained in the early years do not have the same quality that we are used to today. Invasion depth of renal tumor is ideally measured by CT/MRI in free 3D planes instead of fixed axial, coronal, and sagittal planes (25), but this is not possible in most institutions and obviously not for retrospective cohorts.
In conclusion, parenchymal invasion depth and diameter of tumor are the most important characteristics in relation to the type of the nephrectomy performed. All potential anatomic classification systems should be tested against these two simple characteristics.
Footnotes
Acknowledgements
The authors thank Eliisa Kekäläinen, MD, PhD, for revising the figures and Professor Harri Sintonen, PhD, for assistance with designing the tables.
Declaration of Conflicting Interests
Kilpeläinen, Nisen, and Visapää have no conflict of interest to declare. Tornberg declares reimbursement from Astellas for attending a scientific meeting and unrestricted financial grants from Finnish Urological Association. Järvinen declares reimbursement from Lilly, Sobi, and Novartis for attending scientific meetings. Taari declares consultation fees from Abbvie, lecturer fees from GSK, reimbursements from Orion and Astellas for attending a scientific meeting and other from Medivation, outside the submitted work.
Funding
This study was supported by the Competitive State Research Financing of the Expert Responsibility Area of Helsinki University Hospital.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.