
Abstract
Introduction:
This study aimed to evaluate clinical results after plaster cast fixation for 10 days versus 1 month of moderately displaced and reduced distal radius fractures.
Material and Methods:
In a prospective randomized study, 109 patients with moderately displaced and conservatively treated distal radius fractures (age ≥50 years) were randomized 10 days after reduction to either removal of the plaster cast and immediate mobilization (active group) or to continued plaster cast fixation for another 3 weeks (control group). Grip strength, pincer strength, range of motion, and pain were assessed at 1, 4, and 12 months after reduction. Clinical outcome was evaluated using three functional assessment scores at 12 months.
Results:
Treatment failed in 3/54 (6%) patients in the active group. One of these patients had the plaster cast reinstituted because of feelings of instability. The fractures in the other two patients displaced severely after mobilization and were therefore treated surgically. For the remaining 51 patients in the active group, the range of wrist motion was slightly better at 1 month compared with the controls, but there were no differences in grip or pincer strength or pain at the 1-month follow-up. There were no differences between the active and control group in any outcome at 4 or 12 months, including functional assessment scores at 12 months.
Conclusion:
Treatment with mobilization 10 days after reduction of moderately displaced distal radius fractures resulted in a few treatment failures compared with none among controls. The only functional benefit for the remaining patients was a small and transient increase in range of motion at the 1-month follow-up. Plaster cast removal 10 days after reduction in moderately displaced distal radius fractures is therefore not recommended.
Keywords
Introduction
Plaster cast fixation of an injured extremity leads to a gradual decrease in range of motion and muscle strength (1, 2). It therefore seems reasonable to assume that a shorter period of immobilization in a plaster cast of distal radius fractures will result in better functional outcome. Several studies have shown that early mobilization in undisplaced or minimally displaced distal radius fractures leads to the same radiographic results as conventional plaster cast fixation (3–5). It is also possible to treat reduced distal radius fractures with plaster cast removal at 3 weeks (6, 7) or with functional bracing (8–12), without jeopardizing the fracture position. There is some disagreement as to the effect on functional results, however. Some of the studies that compare early mobilization against conventional plaster cast fixation time have not shown any differences in functional outcome between the groups either early or late during the follow-up (4, 10, 13). While other studies have shown transient benefits in functional recovery in favor of early mobilization, but without long-standing differences in the functional end result when compared with controls (7, 9, 11, 12, 14). Only a few studies have demonstrated a persistent positive effect on the functional results following early mobilization (3, 6). In a study of 2000 Colles fractures from The New York State Workmen’s Compensation Board, no correlation was found between the duration of immobilization and the percentage of definite disability (15). A comparison between immobilization in a plaster cast for 2 versus 6 weeks after volar plate fixation of distal radius fractures did not reveal any differences between the treatment groups in range of motion, grip strength, or functional scores at 3- and 6-month follow-ups (16).
The definition of early mobilization differs in these studies. In studies on undisplaced or minimally displaced distal radius fractures that did not need reduction, early mobilization referred to either complete absence of rigid external support after the injury (3) or complete removal of rigid external support 1 week after the injury (4, 5). In one of the latter two studies (4), the active group was initially treated with immediate mobilization in an elastic bandage. However, because these patients frequently returned during the first days because of pain, the study protocol for the active group was changed to fixation in a plaster cast for 1 week after the fracture event followed by free mobilization. In studies on displaced and reduced distal radius fractures, the initial treatment was either plaster cast fixation for 1 week replaced by different kinds of orthoses (8, 10) or application of the orthoses immediately after the reduction (9, 11, 12). To our knowledge, no study has evaluated the benefits and risks of early mobilization without any kind of rigid external support following a short initial period with plaster cast fixation in reduced distal radius fractures. Although there is a potential positive effect from early mobilization after distal radius fractures on functional recovery, the risk for treatment failure caused by insufficient fracture stabilization prior to fracture healing has to be taken into account.
The aim of this study was to compare the incidence of treatment failures and the clinical results between mobilization at 10 days versus 1 month after reduction in moderately displaced distal radius fractures. We hypothesized that early mobilization does not increase the incidence of treatment failure. A second hypothesis was that early mobilization leads to faster recovery and better clinical end results compared with conventional plaster cast fixation time in moderately displaced and reduced distal radius fractures.
Materials and Methods
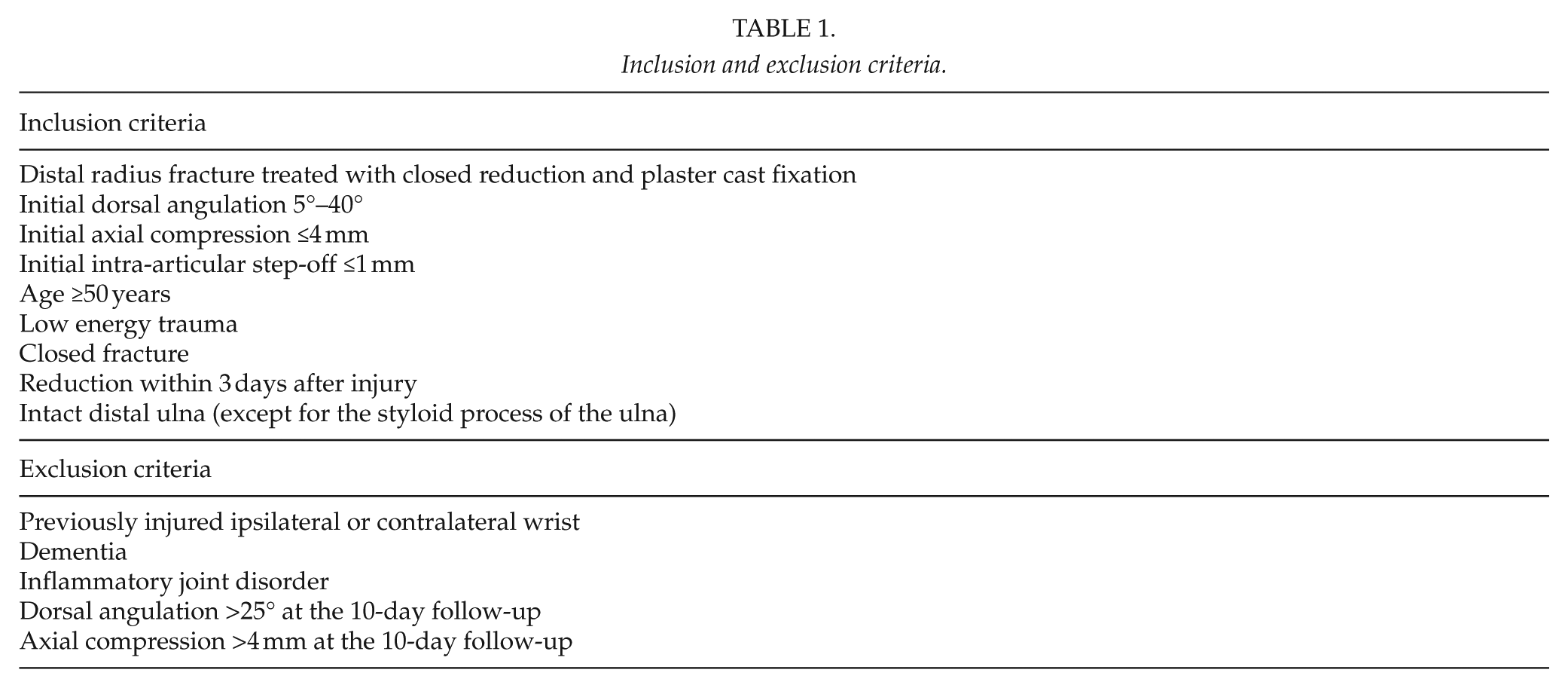
We performed a randomized prospective study from September 2002 to January 2010 at Uppsala University Hospital in which patients who underwent closed reduction and plaster cast fixation in dorsally angulated distal radius fractures (Colles fractures) were screened for inclusion (Fig. 1). Inclusion criteria were age ≥50 years, low energy trauma, closed fracture, reduction within 3 days from injury, a previously uninjured ipsilateral and contralateral wrist, primary dorsal angulation 5°–40° from a line perpendicular to the long axis of the radius, axial compression ≤4 mm, intra-articular step-off ≤1 mm, and an intact ipsilateral ulna (except for processus styloideus ulnae). According to previous studies, fractures with dorsal angulation <5° can be treated with early mobilization (3–5). These fractures were therefore not included in the study. Fractures with dorsal angulation >40°, axial compression >4 mm, or intra-articular step-off >1 were treated surgically and thus not included in the study. Patients with dementia or inflammatory joint disorders were excluded (Table 1).
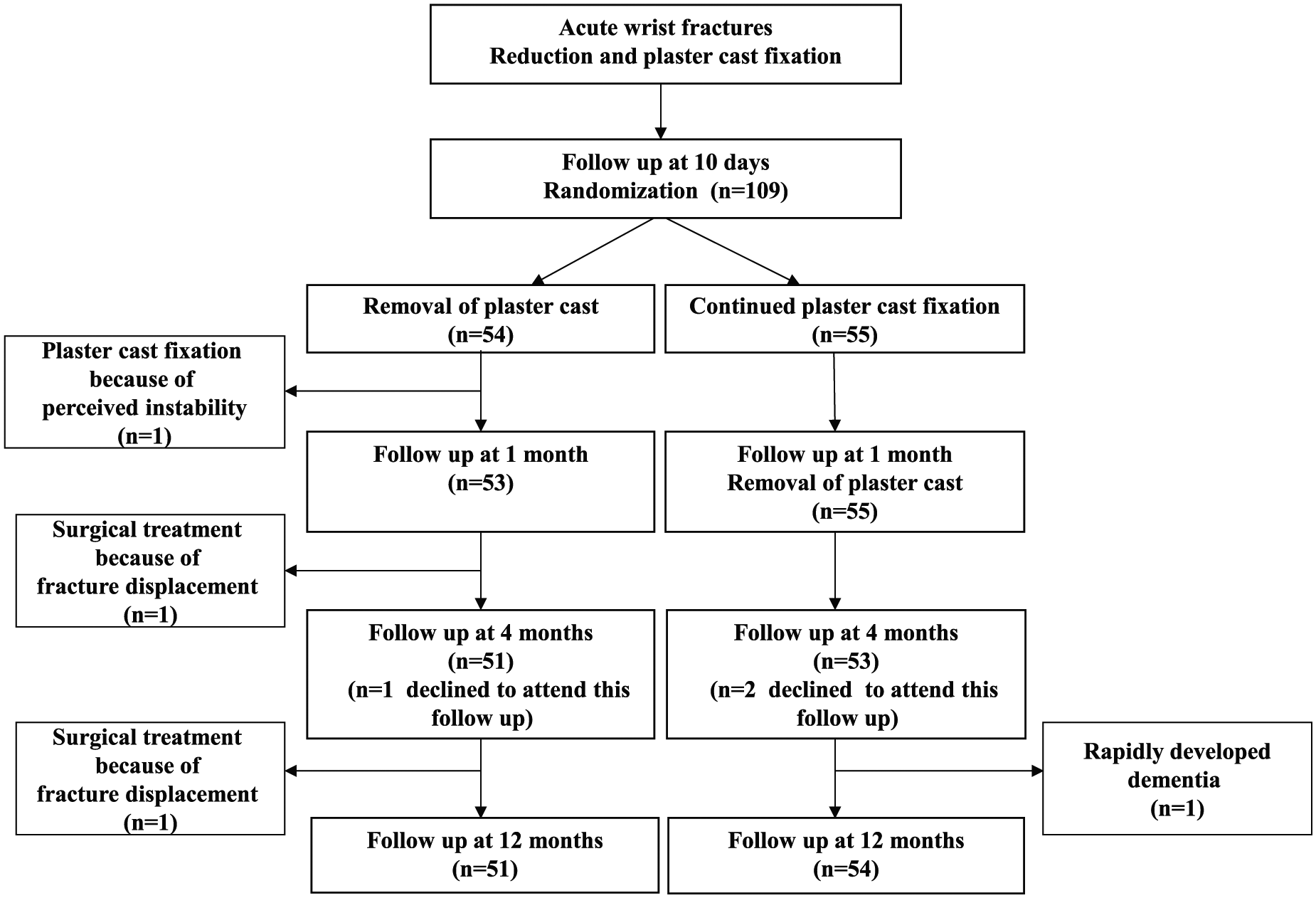
Flow diagram.
Inclusion and exclusion criteria.
The study was approved by the Ethical Committee of Uppsala University (Dnr 216-00) and informed consent was obtained from all patients according to the ethical guidelines of the Helsinki Declaration. The ordinary protocol for the acute treatment of displaced distal radius fractures at our clinic was used during the study. The fractures were manually reduced by the on-call doctor and fixed with a splint made of plaster of Paris, covering approximately two-thirds of the circumference of the dorsal aspect of the wrist and extending from below the elbow down to the metacarpophalangeal joints.
The randomization process was carried out with randomly ordered opaque and sealed envelopes. It was not possible to reveal the choice of treatment without opening the envelopes. A log was kept to ensure that the envelopes were opened sequentially. The inclusion took place at the first follow-up at about 10 days (range, 8–13 days) after reduction. A condition for inclusion was that the fracture initially had undergone reduction and that the radiograph at the 10-day follow-up showed a persistent acceptable position of the fracture defined as dorsal angulation ≤25° and axial compression ≤4 mm. A fracture with larger displacement than this can cause residual disability (17–20). These fractures, which were not included in the study, underwent operative treatment.
In total, 109 patients were included: 54 patients were randomized to immediate removal of the plaster cast (active group) and 55 patients to continued plaster cast fixation for another 3 weeks, totally 4–5 weeks after reduction (control group). The patients who were treated with removal of the plaster cast at the 10-day follow-up after reduction received an elastic bandage around their wrist and were instructed to move their wrist freely to the best of their ability, but to avoid painful activity and heavy weight lifting.
Treatment failure was defined during the first month as problems leading to abandonment of given treatment, and after the first month as poor outcome leading to surgical treatment of a malunited fracture. At 1 month, a physiotherapist, not involved in the study, gave identical instructions to the two treatment groups regarding rehabilitation.
Another physiotherapist measured grip strength with a Jamar dynamometer and pincer strength with a pinch meter in both hands at 1 month (range, 4–5 weeks), 4 months (range, 3.5–4.5 months), and 12 months (range, 11.5–12.5 months) post-reduction. The patients performed three consecutive compressions, of which the third one should not be the highest, with the Jamar dynamometer and the pinch meter at every follow-up; the average value of the three compressions for each meter instrument was recorded (21, 22). The dominant hand in a right-handed patient is considered 10% stronger than the left hand (23, 24) while the dominant hand in a left-handed patient is considered as strong as the right hand (24, 25). This seems to be valid for both men and women (24, 26). Accordingly, in a right-handed patient with a fracture in the right wrist, the value of the grip strength and the pincer strength in the left hand is therefore increased by 10% before comparing it with the fractured right side. In a right-handed patient with a fracture in the left wrist, the grip and pincer strength in the right hand is decreased by 10% before comparing it with the fractured left side. However, the 10% rule is based on studies in young adults, and it has been shown that the differences in hand strength between the right and left hand decreases with increasing age (26, 27). Since the patients in this study were over the age of 50, the differences in hand strength between the groups have been calculated both with and without using the 10% rule. The physiotherapist also measured the range of motion with a goniometer in both wrists in terms of dorsal extension and volar flexion as well as forearm pronation and supination at the 1-, 4-, and 12-month follow-ups. Pain was assessed with a visual analogue scale (VAS) at 10 days and at 1, 4, and 12 months. At each follow-up, the patients were told to set the VAS scale on a level that represented the average pain experienced during the past 24 h. At the follow-up, when the plaster cast was removed, the question about pain was asked before cast removal in both groups to avoid the possibility of registering additional pain immediately after cast removal (Fig. 1).
Differences in grip strength, pincer strength, and range of motion between the injured and uninjured side were calculated at each follow-up.
At the final follow-up at 12 months, the functional end result was estimated using three functional scores: the modified de Bruijn wrist score (28), modified by Christersson and Sandén (Supplementary File 1), the Smith and Cooney modification of the Mayo wrist scoring chart (29) (Supplementary File 2), and the Gartland and Werley Demerit wrist point system, modified by Sarmiento et al. (8) and Christersson and Sandén (Supplementary File 3).
Statistics
The results in grip strength, pincer strength, range of motion, and physician-based scoring systems were normally distributed according to the appearance on histograms and the Shapiro–Wilk’s W test (>95%). Means with 95% confidence intervals (CIs) were used for graphic presentations for each treatment group and Student’s t test was conducted to determine differences between the treatment groups at follow-ups and in baseline characteristics. Pain (as measured by the VAS) was not normally distributed and therefore the active and control groups were compared using the Mann–Whitney U test. Fisher’s exact test was used for proportions. The level of significance was set at p < 0.05 (two-tailed). The Bonferroni method was used to adjust for multiple comparisons.
Results
In all, 109 patients were included in the study (54 patients in the active group and 55 in the control group). Three patients met all inclusion criteria at 10 days but declined to participate before randomization and were therefore not included. The two treatment groups were comparable in terms of age, injured side, fracture type, and initial displacement (Table 2).
Patient characteristics at baseline.
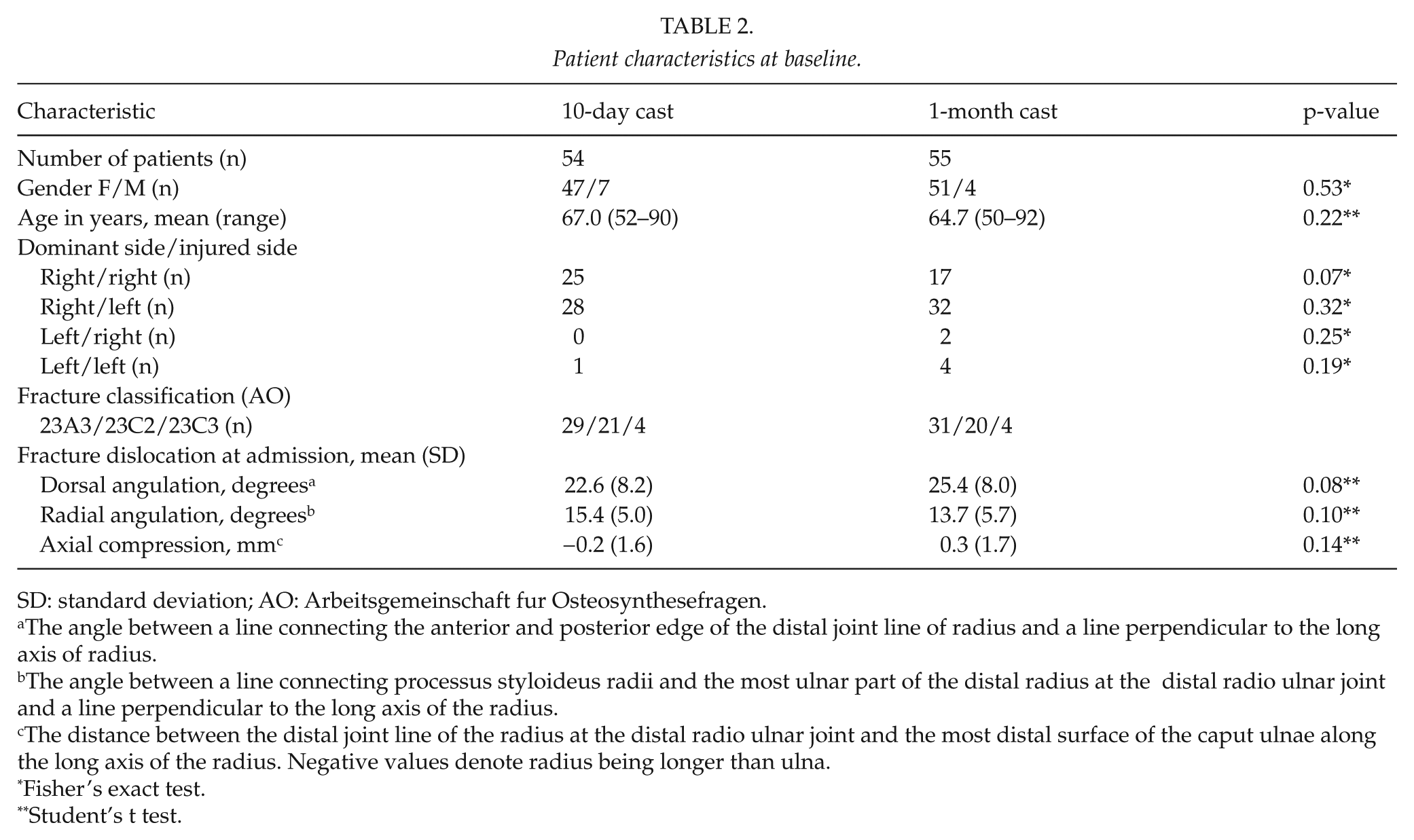
SD: standard deviation; AO: Arbeitsgemeinschaft fur Osteosynthesefragen.
The angle between a line connecting the anterior and posterior edge of the distal joint line of radius and a line perpendicular to the long axis of radius.
The angle between a line connecting processus styloideus radii and the most ulnar part of the distal radius at the distal radio ulnar joint and a line perpendicular to the long axis of the radius.
The distance between the distal joint line of the radius at the distal radio ulnar joint and the most distal surface of the caput ulnae along the long axis of the radius. Negative values denote radius being longer than ulna.
Fisher’s exact test.
Student’s t test.
Three patients (3/54, 6%) in the active group were excluded from the study because of failed treatment, whereas there were no cases of failure leading to treatment changes in the control group (Fig. 1). One of these patients in the active group was excluded after the 10-day follow-up because the patient perceived instability in the fracture and did not want to continue without a cast. The patient was treated with a plaster cast in situ for another 3 weeks followed by a favorable outcome. Concerning the two other patients with failed treatment, one was excluded at the 1-month follow-up and one at the 4-month follow-up because of large redisplacement in the fractures and because of increasing pain and disability after plaster cast removal. Both of these patients were treated surgically with osteotomy and plate fixation. One patient in the control group was excluded from the study because of rapidly developing dementia (Fig. 1). All these four patients are included in the baseline characteristics of the active group, but are not included in the results from the follow-ups. Three patients (one patient in the active group and two patients in the control group) declined to attend the follow-up at 4 months, but participated in the follow-up at 12 months (Fig. 1).
Grip Strength
There were no significant differences in grip or pincer strength at any follow-up when the two treatment groups were compared using the 10% rule (Fig. 2). At the final follow-up, both treatment groups had recovered in strength to a level that was approximately 4 kg below the grip strength of the uninjured side and approximately 0.2 kg below the pincer strength of the uninjured hand after compensation for the dominant/non-dominant hand. When the values for grip and pincer strength were compared without compensation for dominant/non-dominant hand, there were still no differences between the two treatment groups (data not shown).
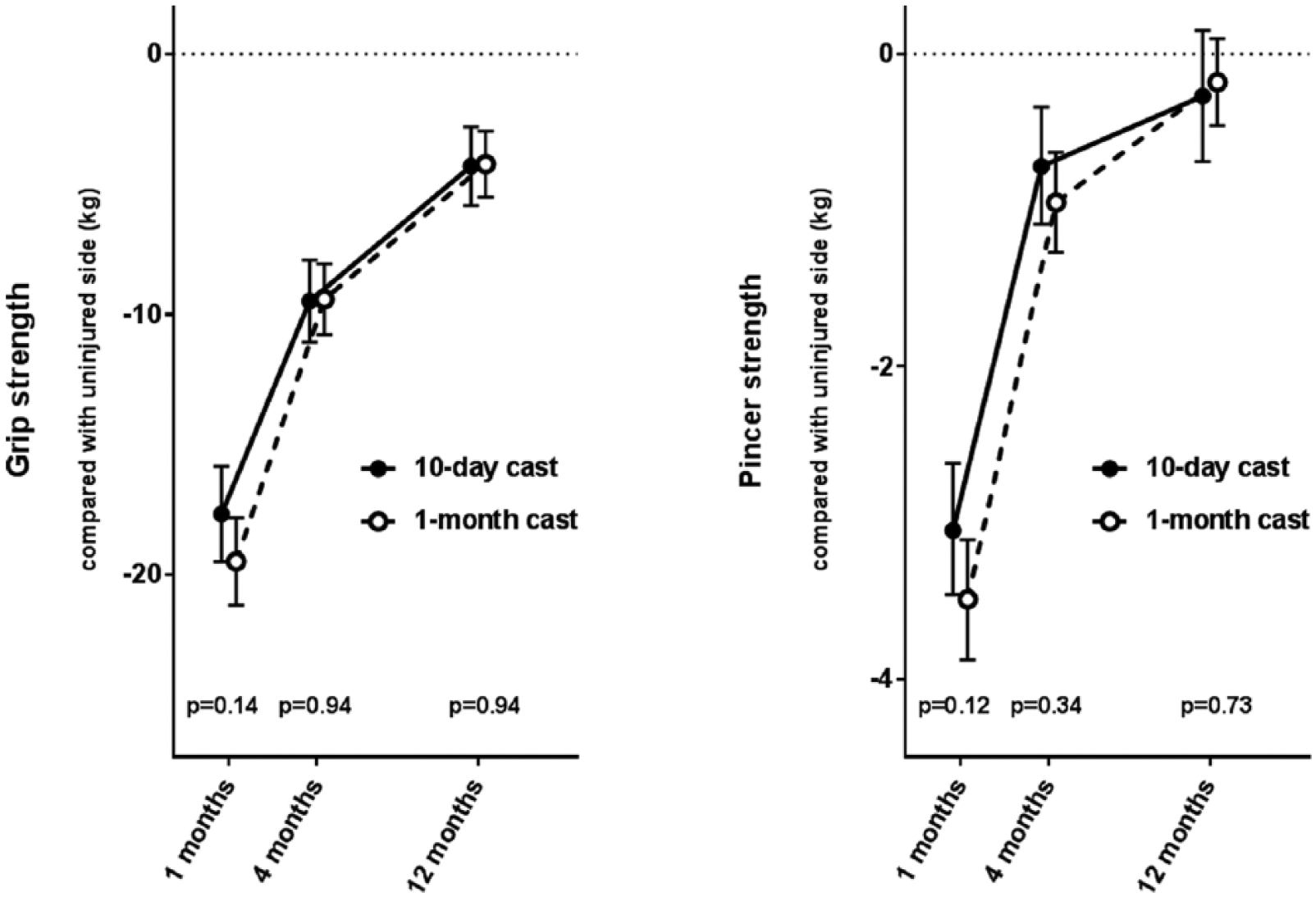
Grip strength (Jamar dynamometer) and pincer strength (pinch meter) compared with the uninjured side (mean ± 95% CI). The results are presented with a compensation for dominant/non-dominant hand (the right hand considered 10% stronger than the left hand in right-handed patients, and the left hand as strong as the right hand in left-handed patients). Three treatment failures in the 10-day cast group and one exclusion in the 1-month cast group have been omitted.
Range of Motion
At 1 month, the range of motion in dorsal extension, pronation, and supination, but not in volar flexion, was significantly better in the active group (Fig. 3): dorsal extension 14° (p < 0.001), pronation 12° (p = 0.002), and supination 8° (p = 0.03). After Bonferroni correction of 12 significance tests for range of motion (p = 0.05/12 = 0.004), the difference in supination was no longer significant.
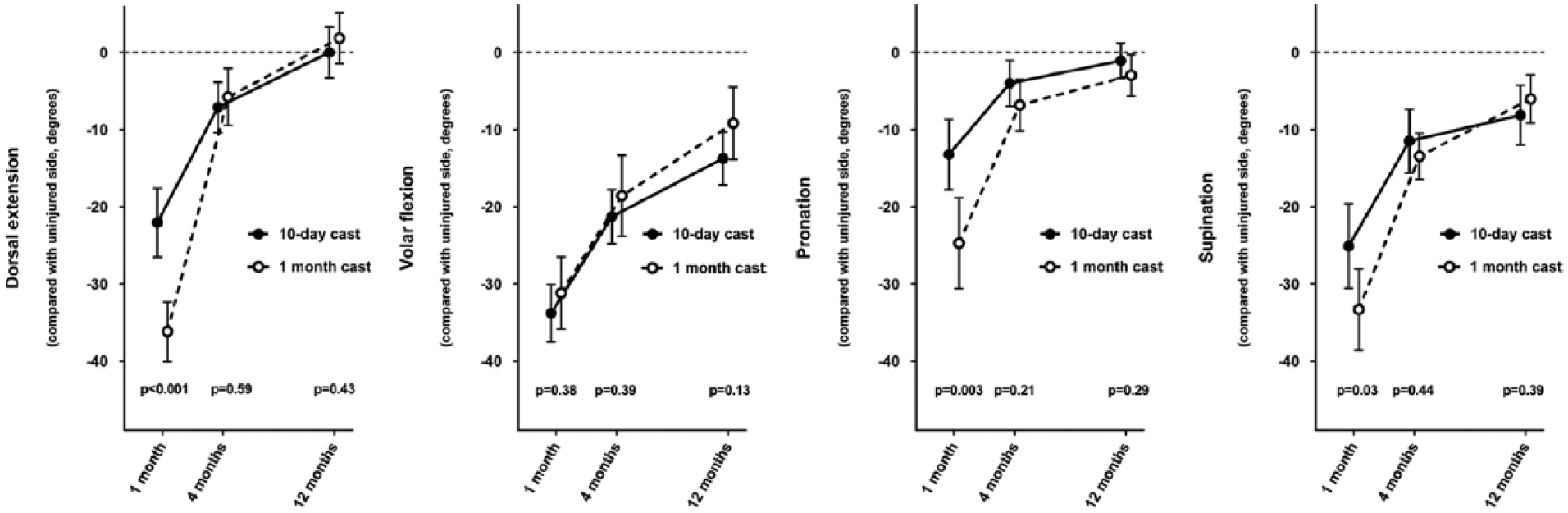
Range of motion compared with the uninjured side (mean ± 95% CI). Three treatment failures in the 10-day cast group and one exclusion in the 1-month cast group have been omitted.
The significant differences between the groups in dorsal extension and pronation found at 1 month were no longer present at subsequent data collection points (i.e. at 4 and 12 months).
Pain
The active group reported more pain than the control group at the 1-month follow-up though this difference was not significant (p = 0.06) (Fig. 4). At 4 and 12 months, no differences in pain were observed between the two treatment groups.
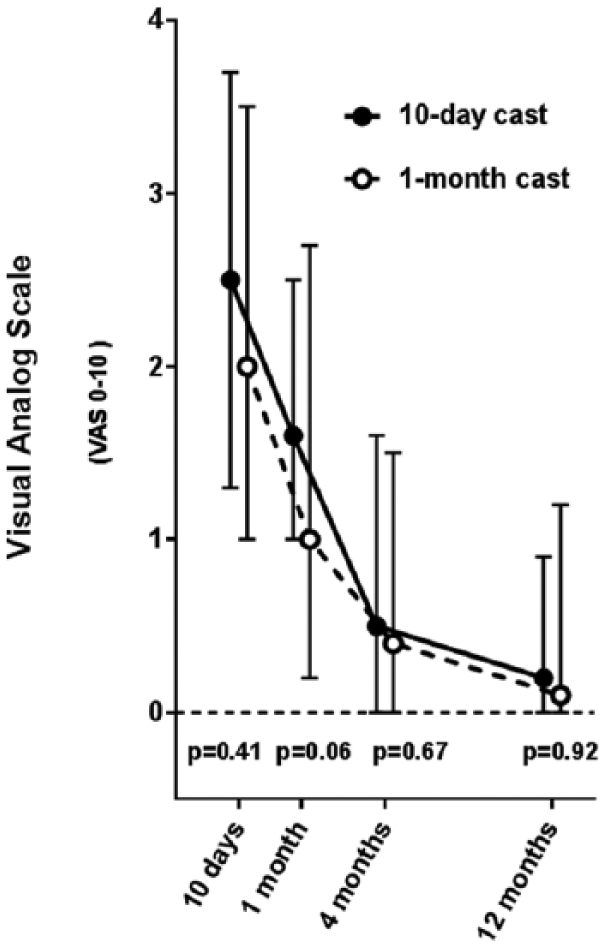
Pain (visual analogue scale) (median with 25th–75th percentiles). Three treatment failures in the 10-day cast group and one exclusion in the 1-month cast group have been omitted.
Assessment Score
At the final 12-month follow-up, the modified de Bruijn, the modified Mayo, and the modified Gartland and Werley Demerit scores showed no differences between the active and control groups (Table 3).
Final evaluation at 12 months with three functional scoring systems (mean (SD)).
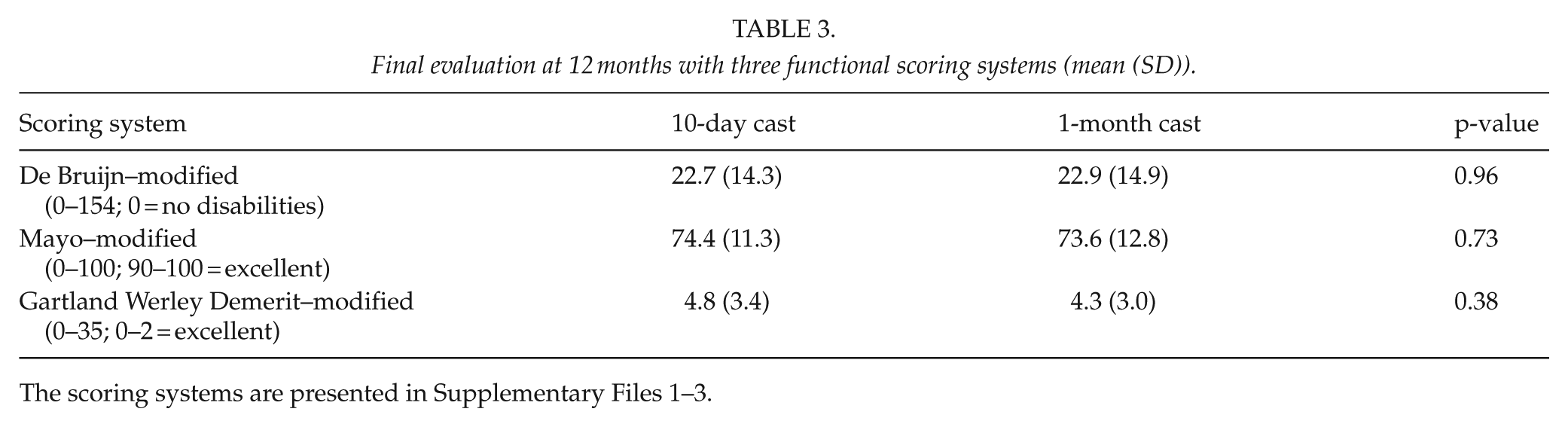
The scoring systems are presented in Supplementary Files 1–3.
Discussion
The rationale for early plaster cast removal after conservatively treated distal radius fractures has been to achieve faster functional recovery and improved clinical results. Ever since Sarmiento’s studies on functional bracing as a therapeutic modality in the 1970s, early mobilization of distal radius fractures has been regarded as preferable compared with immobilization in a plaster cast until healing. However, scientific support has been sparse. A fast recovery of grip and pincer strength is one of the most important treatment goals after a distal radius fracture. In our study, no difference in grip or pincer strength between the groups at the three follow-ups was noted. Several studies on reduced distal radius fractures have reported early improved grip strength after early mobilization (versus conventional plaster cast fixation time) but no late improvement (9, 11, 12). One study reported neither early nor late improvement in grip strength in the active group (5), whereas another study reported both early and late improvement in grip strength in the active group (6). The patients in the active group in our study were told to move their wrists as much as tolerated, but to avoid painful activity and heavy lifting after the cast removal at 10 days. The absence of a difference in grip and pinch strength between the groups at 1 month indicates that the early mobilized group did not benefit in grip or pincer strength from being able to move the injured wrist joint freely. It could be argued, however, that the instructions (given to the early mobilized group at 10 days, that is, at the time the plaster cast was removed) were overly cautious and thus prevented the patients in the active group from rehabilitating faster than the control group. However, the patients were told to use the injured arm as much as they could tolerate, and more aggressive instructions could have possibly increased the risk for treatment failure.
The only statistically significant clinical benefit from early mobilization found in this study was an increased range of motion in dorsal extension and pronation at 1 month. After Bonferroni correction, the difference in supination at 1 month was not statistically significant. The Bonferroni correction is a conservative way of compensating for multiple comparisons. However, the conclusions of this study are not dependent on the results of supination at 1 month. Still, mobilization at 10 days after reduction leads to somewhat better range of motion at 1 month compared with mobilization at 1 month, but no positive effects in the long run. At this short follow-up, that is, at 1 month, the patients in the control group had their plaster cast removed. Thus, the difference in range of motion between the two treatment groups may have been caused by a residual stiffness from the cast fixation in the control group. If that were the case, it is possible that the range of motion in the control group recovered to the level of the early mobilized group rather quickly after the removal of the plaster cast. Because there were follow-ups only at 1, 4, and 12 months, it is not possible to determine when, between 1 and 4 months, the range of motion for the two groups approached each other. A temporary gain in range of motion at 1 month can be useful for active patients, but without enhancement in grip or pincer strength one cannot be certain that it results in an improved functional capacity compared with immobilization for 1 month. Our result of a transient gain in range of wrist motion is consistent with other studies (6, 14, 30). One study reported a persistent increased range of motion over the long term, but these fractures were undisplaced (3).
No difference was noted between the two treatment groups in pain at any follow-up. A few studies have reported decreased pain in early mobilized groups during the early treatment phase (3, 6, 12), whereas other studies have shown equal levels of pain during the early treatment phase (5, 9, 14). Almost all studies reporting pain after early mobilization in distal radius fractures have observed similar pain levels between the groups over time (9, 11, 12). Only two studies have reported persistent lower pain in the active group at a 1-year follow-up: one of these studies was made on undisplaced fractures (3) and one on slightly displaced and reduced fractures (6).
The functional effect of early mobilization on the end result after distal radius fractures was evaluated in this study with three physician-based scoring systems at 12 months. The reason for using different scoring systems was that these systems are all well known and all focus on slightly different aspects of functional outcome. The modified de Bruijn score focuses primarily on the patient’s subjective evaluation of the function, the modified Mayo scoring system puts more emphasis on pain and objective measurements, and the modified Gartland and Werley Demerit point system involves complications and residual deformity. These scores showed no long-term differences between the groups, indicating that early mobilization in reduced distal radius fractures does not have any positive effect compared with fixation for 1 month. In recent years, patient-completed health status questionnaires (PROMs, patient-reported outcome measures) have increasingly come into use instead of physician-based scoring systems. When this study was planned and initiated, validated PROMs were not readily available. One limitation of our study is that the final outcome was evaluated only with physician-based scoring systems. However, the use of three scoring systems provides some compensation for this limitation, and because the results are very similar between the two treatment groups, we believe that the results would have been comparable with patient-completed health status questionnaires. The three functional scores used in this study also partly contain subjective assessment reported by the patient.
The radiographic results of this study have already been published (31). Both groups were equally reduced after admission. However, the early mobilized group displaced slightly more in radial angulation (3.2°, p = 0.002) and axial compression (0.7 mm, p = 0.02) from admission to 12 months compared with the control group.
In general, our findings are in accordance with studies showing a limited and transient positive effect of early mobilization of distal radius fractures (7, 9, 11, 12, 14), but the magnitude of the positive effects are somewhat smaller in our study, perhaps because the fractures in our study were more displaced at admission.
Three patients in the active group and one patient in the control group were excluded. The three patients in the active group were excluded because of treatment failure. The threshold for excluding patients in the active group may have been lower than in the control group because of greater sensitivity for complaints in the latter. However, the reasons for exclusion of these three patients were obvious. One patient was excluded because the patient felt movements in the fracture after plaster cast removal, which made continued treatment in an elastic bandage impossible. This fracture was located slightly more proximal than the other fractures in the study, which may have contributed to the feeling of instability. The other two patients in the active group were excluded because of more severe fracture displacement than any other fracture in the study, causing pain and disability.
A potential limitation of the study is the small sample size that could affect the statistical power of the results. However, the sample size in this study was big enough to reveal a difference between the groups at the follow-ups of 2.7–3.5 kg in grip strength, 0.7–0.8 kg in pincer strength, and 5°–11° in range of motion with a significance level of 0.05 and a power of 80%, if such differences were to exist. Therefore, we believe that the samples were of sufficient size to reveal clinically relevant differences between the groups.
Conclusion
Treatment with mobilization 10 days after reduction of moderately displaced distal radius fractures resulted in a few more treatment failures compared with the controls, and the only functional benefit for the remaining patients was a small and transient increase in range of motion at the 1-month follow-up. Plaster cast removal 10 days after reduction in moderately displaced distal radius fractures is not recommended when the limited and temporary increase in wrist motion is weighed against the increased risk for treatment failure.
Footnotes
Acknowledgements
The authors would like to thank the physiotherapist Elisabeth Belin for carrying out the clinical assessments and Lars Berglund, PhD, associate professor, Uppsala clinical research centre, UCR statistics, Uppsala University, for statistical consultation support.
Availability of Data and Materials
The dataset supporting the conclusions of this article is not publicly available due to the inclusion of potentially identifiable patient data but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Committee of Uppsala University (Dnr 216-00).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all patients according to the ethical guidelines of the Helsinki Declaration.
Trial Registration
ClinicalTrail.gov, NCT02798614. This study was initiated in 2002 and retrospectively registered on 16 June 2016.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.