
Abstract
We performed an 11–13-year prospective follow-up of patients after a distal radial fracture (DRF) to investigate the association between fracture malunion, radiocarpal osteoarthritis and clinical outcome. In total, 292 patients responded to patient-reported outcome measures; of them, 242 underwent clinical examination. Clinical outcomes improved with time. A decade after fracture, median Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score was 5, EuroQol Five-dimensions score was 1.0, and range of motion and grip strength were 96% of the contralateral side. Neither osteoarthritis (6%) nor pseudoarthrosis of the ulnar styloid (30%) affected the outcomes. Dorsal tilt, radial inclination, ulnar variance and intra-articular extension did not affect long-term clinical outcomes or the risk of osteoarthritis. Recovery after a DRF is an ongoing process that lasts years. A decade after the injury event, range of motion, grip strength and QuickDASH were recovered to population normal, regardless of radiological outcomes.
Keywords
Introduction
Distal radius fractures (DRFs) are the most common fractures in adults (Nellans et al., 2012; van Staa et al., 2001), and their short-term outcomes are well reported (Mulders et al., 2018). Few studies, however, have examined the long-term effects of the association between malunion, radiocarpal osteoarthritis and functional outcomes (Ali et al., 2018; Visser et al., 2020).
Radiological alignment (Ali et al., 2018; Raudasoja et al., 2018) and pain catastrophization (Hevonkorpi et al., 2021) have been proposed to affect long-term results. However, there is no evidence linking age (Raudasoja et al., 2018), pseudoarthrosis of the ulnar styloid (Ali et al., 2018), osteoarthritis, (Ali et al., 2018; Visser et al., 2020) or treatment method (percutaneous wires vs. plate and operative vs. non-operative) to the long-term outcome of DRFs (Costa et al., 2019; Hevonkorpi et al., 2021).
The aim of the present study was to analyse the association between clinical and radiological outcomes of DRFs over a period of 11–13 years. The hypothesis was that malunion would be associated with a worse clinical outcome.
Patients and methods
Study design and setting
Between October 2009 and September 2011, we performed a prospective multicentre cohort study of all patients with a DRF treated at the Departments of Orthopaedic Surgery in Sundsvall and Östersund, Sweden. The short-term outcomes of the study have been published (Schmidt et al., 2023; Wadsten et al., 2017, 2018). This follow-up study reports the long-term results of patient-related outcome measures (PROMs) and clinical examination. The primary outcome measure was Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH). Sundsvall and Östersund Hospitals are secondary-level hospitals serving catchment areas with populations of approximately 160,000 and 130,000 residents, respectively. The study was conducted in accordance with the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines.
Participants and data collection
All patients (age range 15–75 years) presenting with an acute DRF were screened for study enrolment. Patients with open physes were excluded, resulting in a cohort of patients aged 18–75 years. Data were collected prospectively by follow-up visits (10–14 days, 3 months, 1 year and 11–13 years after injury) at the participating orthopaedic departments. Eligible individuals (n = 324) were invited to participate 11–13 years after the fracture event. Of the 324 eligible patients, 292 (90%) responded to PROMs and 243 (75%) underwent clinical examination (Figure 1).
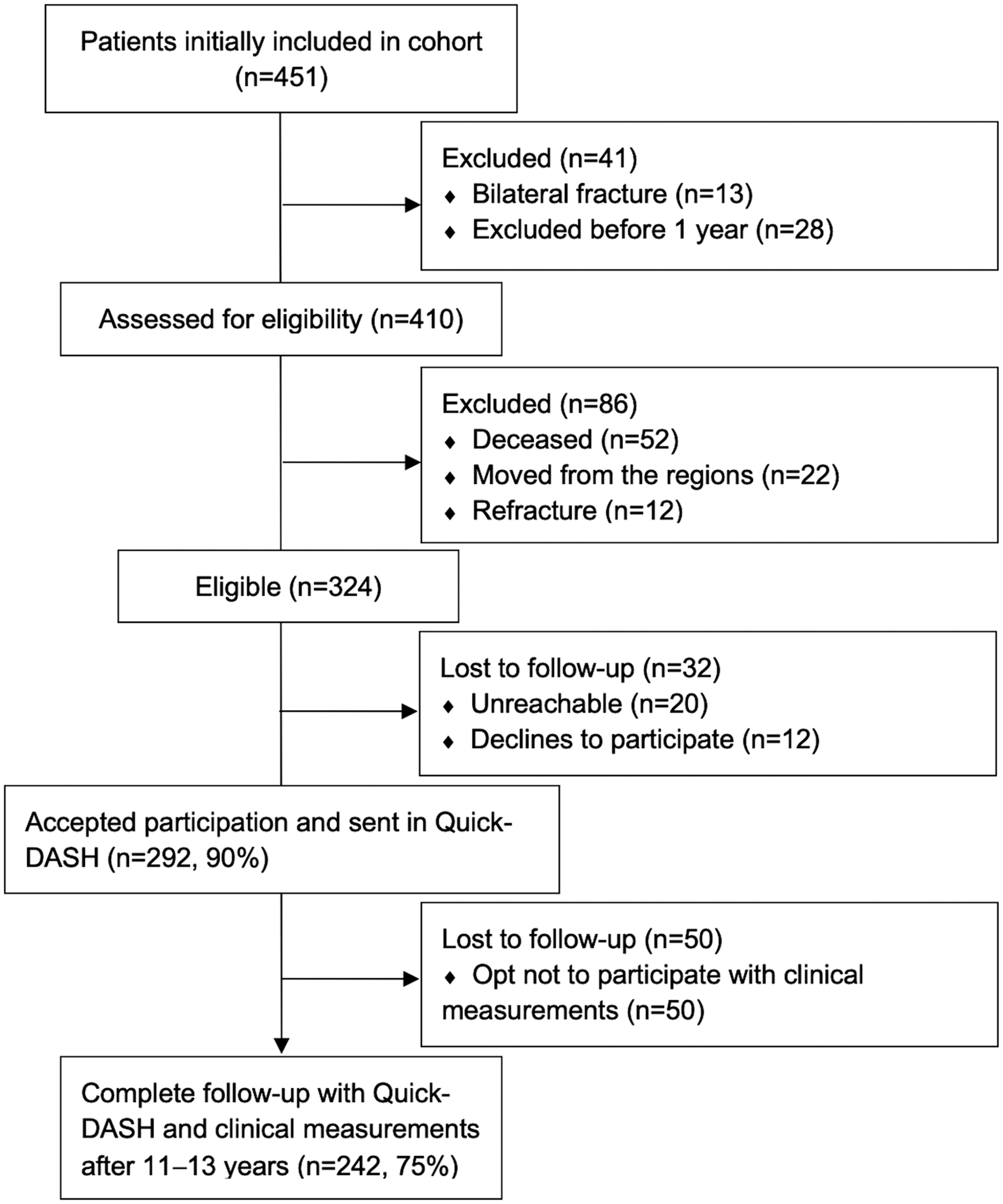
Flow chart of patients included in the study.
Clinical outcomes
QuickDASH and EQ-5D-3L were assessed (Gummesson et al., 2006; Rabin and de Charro, 2001). An independent therapist and one author (AP) measured wrist function at 1 year and at 11–13 years after the fracture. Grip strength (GS) was measured in both hands using a JAMAR dynamometer. Range of motion (ROM), including flexion, extension, radial and ulnar deviation, pronation and supination, were measured using a standard goniometer (HAKIR, 2013). The examiners were blinded to radiological outcomes.
Radiographic measurements
Anteroposterior and lateral radiographs were taken before and after reduction, at approximately 3 months and at 11–13 years. Radial inclination, dorsal tilt, ulnar variance and intra-articular step-off were measured on anteroposterior and lateral radiographs in neutral rotation. In total, 237 patients had further radiographs at 11–13 years. There were no nonunions. Osteoarthritis was graded on a scale of 0–4 (Kellgren and Lawrence, 1957). Capitate shift and pseudoarthrosis of the ulnar styloid were recorded.
All images were digitally acquired using the Sectra Picture Archiving and Communication System, and all measurements were performed by two authors (VS, AS).
Implants and surgery
A treatment algorithm was used (Wadsten et al., 2014). Patients with fractures that remained displaced after reduction or were displaced at follow-up were offered surgical treatment with percutaneous pin fixation, external fixation, open reduction internal fixation (ORIF) with anatomical plates or a combined method at the surgeon’s discretion.
Statistics
Tests for normality were conducted using the Shapiro–Wilk test. Skewed data were presented as medians with interquartile range (IQR) and proportions were presented as percentages. The t-test and Wilcoxon rank-sum test were used to analyse responders to non-responders as well as complications. The Kruskal–Wallis test was used to compare treatment methods when analysing QuickDASH. The Friedman test with Bonferroni correction was used to compare clinical outcome over time. The Pearson correlation coefficient was used to analyse the flexion-extension arc.
We used linear regression modelling with cubic splines for each outcome measure to test if the independent variables influence the outcome. The same variables (sex, age, dominant hand, surgical management, dorsal tilt, radial inclination and ulnar variance) were included in all three models (QuickDASH, GS and ROM). For QuickDASH and GS outcomes, we also included the GS of the non-injured hand as an independent variable. For ROM outcome, we used the ROM of the non-injured side instead of GS on the non-injured hand. Continuous variables were evaluated using ANOVA for non-linearity. Non-linearity is used to explain a relationship between an independent and dependent variable that is not a straight line. Non-linear relationships create a curve as opposed to linear relationships, and, as such, changes in the output do not change in direct proportion to changes in any of the inputs. If non-linearity were confirmed, the non-linearity was modelled with cubic splines. The number of knots was chosen using the minimum Akaike information criterion (AIC) from a set of 3–7 knots. Crude (unadjusted format without any of the covariates) and adjusted values are presented; the adjusted values were used to draw our conclusion. Upon application of bootstrapping, the resultant confidence intervals (CI) showed negligible differences.
A logistic regression model assessed the risk of high QuickDASH scores. Assumptions for logistic regression were met. Sex, age at injury, GS at 12 months, ROM at 12 months, QuickDASH at 12 months, dorsal tilt, ulnar variance, radial inclination and intra-articular involvement were included in the model.
The intraclass correlation coefficient (ICC) was used to test inter-rater reliability between the authors (VS, AS) regarding radiographic measurements (using a two-way mixed-effects model based on a single rating).
All analyses were performed using R (version 4.2.2), knitr (version 1.41) for reproducible research, ggplot2 (version 3.4.0) for plots, and Gmisc (version 3.0.1) with Greg (version 2.0.1) for table output.
Results
Patients and descriptive data
Of 324 eligible patients, 292 (90%) were included in the study. The non-participants did not differ from our cohort (Table 1). Radiographs at 10 years were similar to those at 3 months (Supplementary Table S1).
Baseline characteristics.
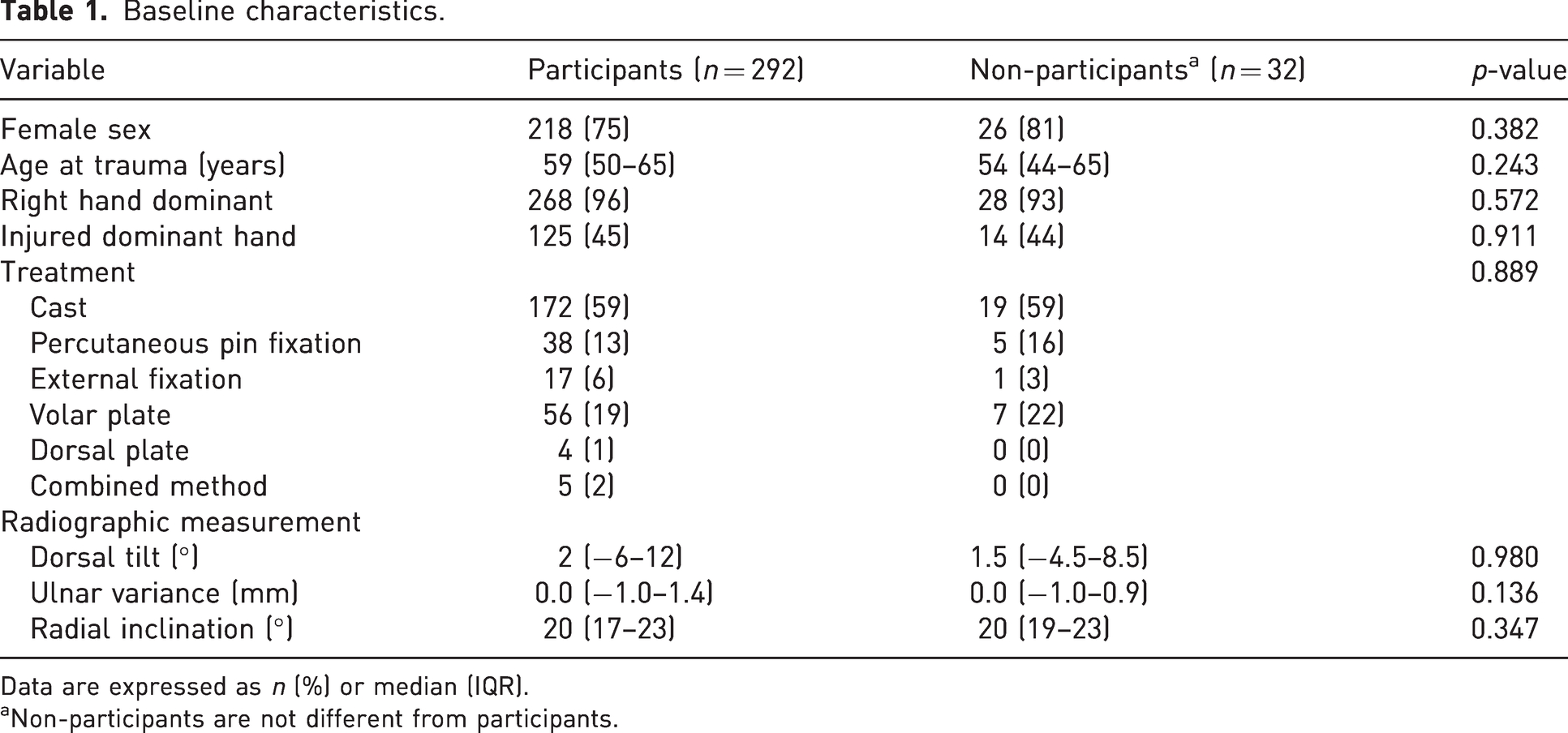
Data are expressed as n (%) or median (IQR).
Non-participants are not different from participants.
QuickDASH did not differ for ORIF, percutaneous fixation or nonoperative treatment at 1 year, with respective median scores of 10 (IQR 2–23; range 0–61), 11 (IQR 5–27; range 0–65) and 11 (IQR 2–23; range 0–61). At 11–13 years, ORIF had statistically significantly higher QuickDASH scores than percutaneous treatment (9 [IQR 2–16; range 0–50] vs. 2 [IQR 0–11; range 0–75] [p = 0.030], non-operative, 5 [IQR 0–18; range 0–68]).
Patients undergoing reoperation because of a complication fared worse (QuickDASH 14 compared to 5 [p = 0.009]) than those who did not (Supplementary Table S2).
Clinical outcome
Clinical outcomes improved over time (Table 2). There were 23 (8%) patients with a major disability after 11–13 years (QuickDASH scores >35). The corresponding number of patients was 30% at 3 months and 14% at 12 months.
Clinical outcome as a function of time.
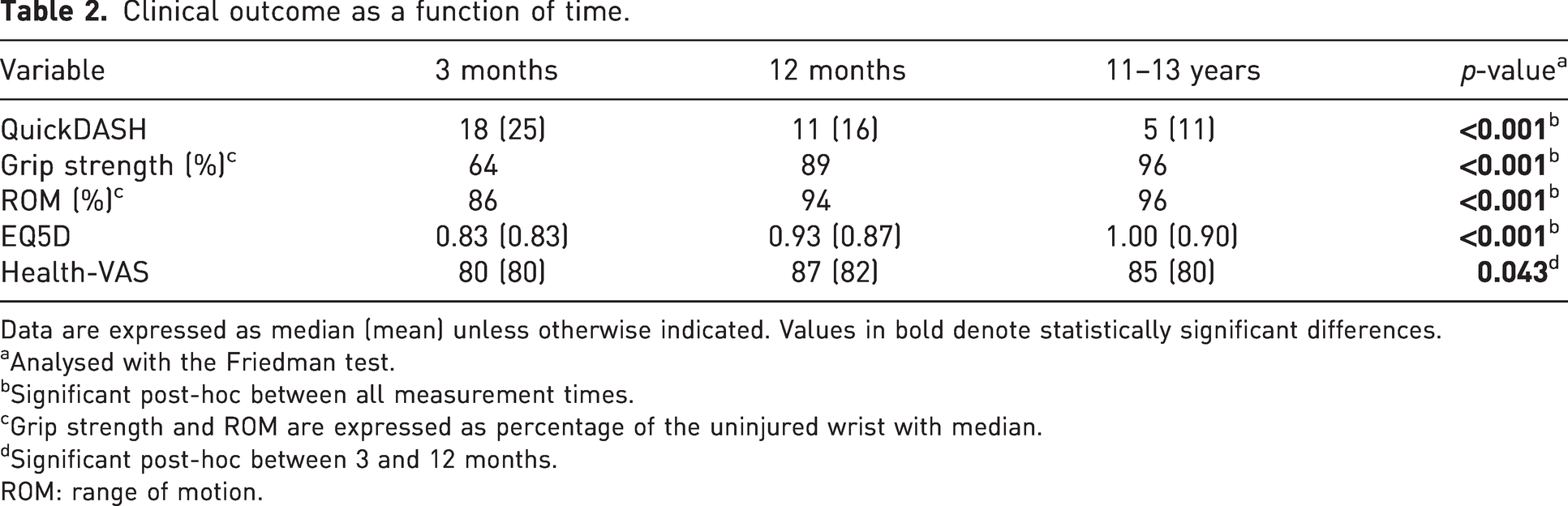
Data are expressed as median (mean) unless otherwise indicated. Values in bold denote statistically significant differences.
Analysed with the Friedman test.
Significant post-hoc between all measurement times.
Grip strength and ROM are expressed as percentage of the uninjured wrist with median.
Significant post-hoc between 3 and 12 months.
ROM: range of motion.
Radiographic analysis
After 11–13 years, 15 (6%) patients had developed osteoarthritis (Kellgren–Lawrence grade 2–4). Of them, 9 (60%) had an intra-articular fracture. Of all fractures, 40% had intra-articular extension. The difference was not statistically significant (p = 0.149). Overall, intra-articular extension was present in 95 fractures, with a median intra-articular step-off measuring 0.4 mm (IQR 0–1). In total, 70 (30%) patients had pseudoarthrosis of the ulnar styloid. Neither osteoarthritis nor pseudoarthrosis affected the outcome at 10 years (Table 3). Dorsal tilt, radial inclination, ulnar variance and intra-articular extension did not affect clinical outcome or the risk of osteoarthritis (Table 3 and Supplementary Table S3).
Variation in QuickDASH, grip strength and ROM by variable, in a linear regression model with cubic splines, without any non-linear elements (dorsal tilt).
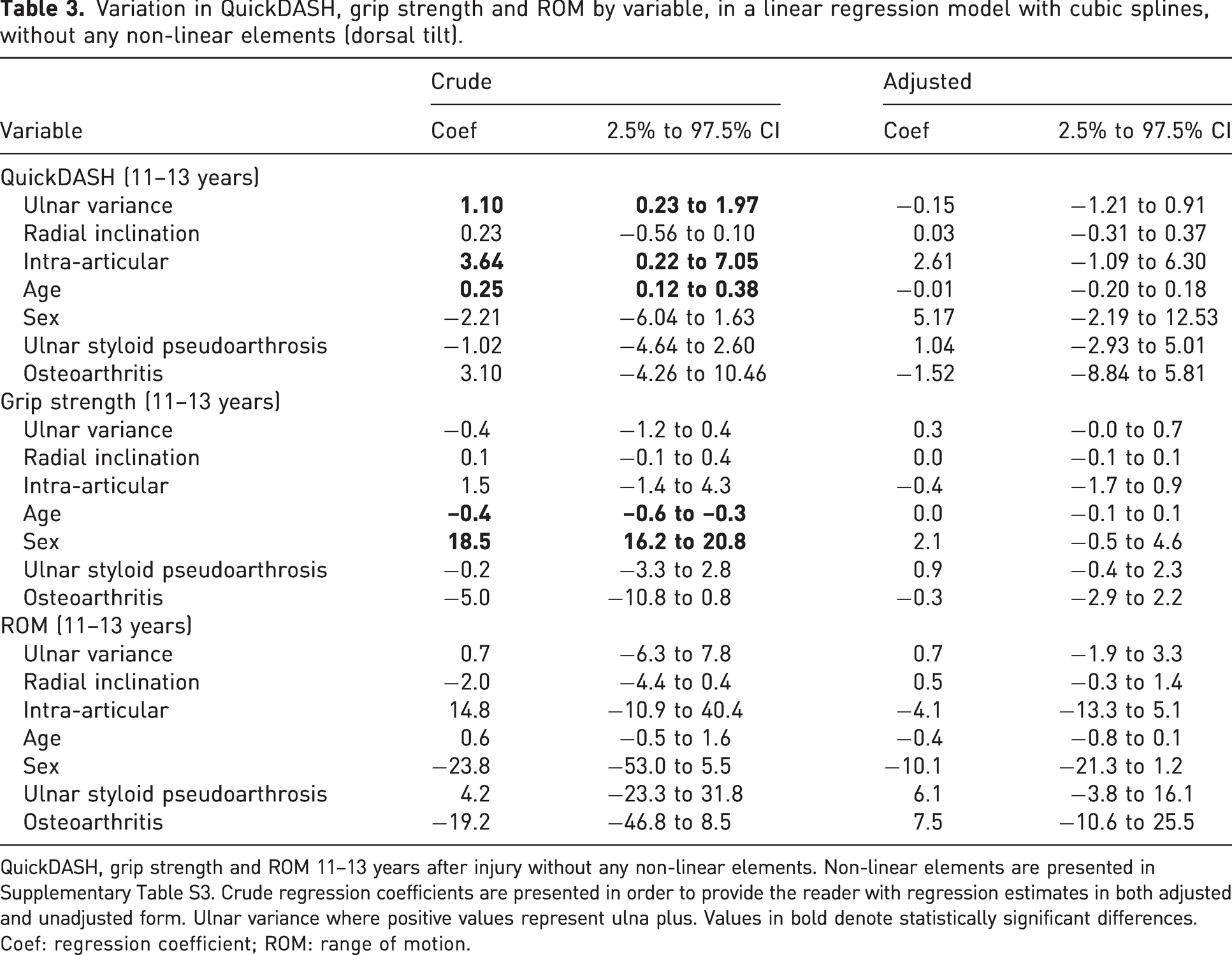
QuickDASH, grip strength and ROM 11–13 years after injury without any non-linear elements. Non-linear elements are presented in Supplementary Table S3. Crude regression coefficients are presented in order to provide the reader with regression estimates in both adjusted and unadjusted form. Ulnar variance where positive values represent ulna plus. Values in bold denote statistically significant differences.
Coef: regression coefficient; ROM: range of motion.
ROM was almost restored after 11–13 years (Table 2); however, the flexion-extension arc moved with dorsal tilt. For each degree of dorsal tilt from anatomical alignment, the flexion-extension arc moved 0.23° in the dorsal direction, with a decrease in flexion and an increase in extension, following the direction of the malalignment. The Pearson correlation coefficient was moderate (r = 0.38).
ICC was calculated for inter-rater reliability on 47 patients for dorsal tilt (0.91, 95% CI: 0.85 to 0.95) graded as excellent, radial inclination (0.89, 95% CI: 0.80 to 0.94) graded as good and ulnar variance (0.82, 95% CI: 0.70 to 0.89) graded as good.
Predictors of major disability
Older age at injury, female sex and higher QuickDASH at 12 months were all predictors of a QuickDASH score >35 at 11–13 years. No radiological parameter seems to affect the long-term risk of major disability (Supplementary Table S4). No working-age patient (<65 years) at the time of follow-up had a QuickDASH score >35.
Discussion
Recovery after a DRF is a continuous process that lasts years. This study shows that ROM, GS and QuickDASH score had improved a decade after the injury despite radiological outcomes. This finding was at odds with our initial hypothesis, and with a previous prospective study (Ali et al., 2018). The algorithm used to manage patients has achieved good long-term functional outcomes.
In this study, QuickDASH scores were at least as good as the general population for a matched age group (Aasheim and Finsen, 2014; Klum et al., 2012), demonstrating the return of what can be considered normal function in our patient cohort.
The literature presents conflicting results regarding malunion and the long-term outcome of PROMs. Five retrospective studies (total n = 517 patients) found no correlation between malunion and PROMs (Catalano et al., 1997; Forward et al., 2008; Goldfarb et al., 2006; Hevonkorpi et al., 2021; Visser et al., 2020). One well-conducted prospective study with a long-term follow-up (63 patients) reported an association between PROMs and malunion (Ali et al., 2018). Despite the large sample size and prospective design, this study did not detect an association between radiographic alignment and outcome.
Ali et al. (2018) categorized malunion as >10° of dorsal tilt, >3 mm of ulnar variance or <15° of radial inclination. Patients without malunion in this study had a similar QuickDASH score compared to our study (6 and 5, respectively). However, the QuickDASH score of patients with malunion differed considerably between the studies (19 in their study and 8 in this study). Despite differences in sample size and a slightly different treatment algorithm, the populations do not differ in age, sex, radiographic alignment, frequency of surgical treatment or loss to follow-up. As such, the large discrepancy in results is difficult to explain.
Several studies have reported an association between malunion and osteoarthritis although no correlation between osteoarthritis and PROMs was demonstrated (Catalano et al., 1997; Forward et al., 2008; Goldfarb et al., 2006; Visser et al., 2020). This study found no correlations between radiographic measures, osteoarthritis or PROMs. Most studies analysing osteoarthritis only include patients with intra-articular extension, which might explain the discrepancy with this study, where all fracture patterns were included. Furthermore, radiographic assessment of step-off can be challenging (Watson et al., 2016). It is noteworthy that the incidence of radiocarpal osteoarthritis in this study is low (Kellgren–Lawrence grade 2–4), which could contribute to the fact that our patients are restored to normal function 10 years after the fracture.
No difference in patient-rated wrist evaluation (PRWE) was noted in a retrospective study analysing operative versus non-operative treatment and malunion (Hevonkorpi et al., 2021). In their study, patients regained normal function in the long term, consistent with our findings. We found a statistically significant difference in favour of percutaneous treatment over ORIF, but the difference did not reach the minimally clinically important difference (Franchignoni et al., 2014). Moreover, because this was an observational study, treatment was not randomized, and therefore no conclusions about treatment superiority can be drawn. Still, the patients treated with ORIF seem to attain their final clinical outcome earlier than those treated with percutaneous or non-operative methods (Mulders et al., 2019).
Approximately 1 year after a DRF, function is still affected (Schmidt et al., 2023). The recovery in ROM, GS and EQ-5D continues in a similar manner to QuickDASH and is restored to population normal after a decade.
In our study, 8% of the patients presented with a major disability (QuickDASH score >35) (Abramo et al., 2010; Landgren et al., 2017). No radiological parameter seems to affect the risk of a major disability. Older age at injury, female sex and a high QuickDASH score at 12 months were associated with an increased risk of major disability. Further studies analysing patient personality factors would improve our understanding of outcomes after DRFs.
The present study has some limitations. These include using QuickDASH, which is not a wrist-specific questionnaire, even though it is an often-used and validated measurement for DRFs (Atroshi et al., 2000; Gummesson et al., 2006). In addition, PRWE and QuickDASH are not optimal tools to measure outcome after DRF due to a ceiling effect (Bell et al., 2023). We did not assess osteoarthritis of both wrists and thus cannot estimate the post-traumatic effect of the DRF. Moreover, CT scans were not obtained to assess intra-articular fracture extension or the presence of osteoarthritis. Furthermore, the observational study design does not enable us to conclude the superiority of any treatment method. We lost 10% of patients to follow-up; however, the non-responders did not differ from our cohort and thus probably do not affect our results.
Conclusion
Recovery after a DRF is a process that continues over several years. A decade after the injury, ROM, GS, EQ-5D and QuickDASH were recovered at the group level. Even though malalignment affects outcomes in the short term, patients may find comfort in knowing that their function is likely restored after over a decade, regardless of radiological alignment.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934231194682 - Supplemental material for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study
Supplemental material, sj-pdf-1-jhs-10.1177_17531934231194682 for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study by Viktor Schmidt, Max Gordon, Anna Petterson, Christian Buttazzoni, Amelia Seimersson, Arkan Sayed-Noor, Sebastian Mukka and Mats Wadsten in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934231194682 - Supplemental material for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study
Supplemental material, sj-pdf-2-jhs-10.1177_17531934231194682 for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study by Viktor Schmidt, Max Gordon, Anna Petterson, Christian Buttazzoni, Amelia Seimersson, Arkan Sayed-Noor, Sebastian Mukka and Mats Wadsten in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934231194682 - Supplemental material for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study
Supplemental material, sj-pdf-3-jhs-10.1177_17531934231194682 for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study by Viktor Schmidt, Max Gordon, Anna Petterson, Christian Buttazzoni, Amelia Seimersson, Arkan Sayed-Noor, Sebastian Mukka and Mats Wadsten in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934231194682 - Supplemental material for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study
Supplemental material, sj-pdf-4-jhs-10.1177_17531934231194682 for Functional outcomes are restored a decade after a distal radius fracture: a prospective long-term follow-up study by Viktor Schmidt, Max Gordon, Anna Petterson, Christian Buttazzoni, Amelia Seimersson, Arkan Sayed-Noor, Sebastian Mukka and Mats Wadsten in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors thank Maria Hedlund, Camilla Stålhammar and Lillemor Wågström for their aid in data gathering.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Informed consent
Written informed consent was obtained from all participants before the study.
Ethical approval
Ethical approval for this study was obtained from the regional ethical committee at Umeå University (Dnr 09-213).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.