
Abstract
Background and Aims:
Distal forearm is the most common fracture location in the growing skeleton. The aim of this article is to describe the current practice of these fractures.
Materials and Methods:
Case series accompanied by experts’ opinion.
Results and Conclusion:
Most of these injuries are benign incomplete distal metaphyseal torus fractures best treated with a dorsal below elbow splint for 2–3 weeks with no follow-up. Completely displaced metaphyseal fractures in prepubertal children can be either immobilized in bayonet position after axial alignment or fixed with K-wires after reduction. Complete fractures of distal metaphysis in adolescents should heal in near anatomic alignment because remodeling is uncertain. We advocate reduction of most greenstick and complete fractures at the distal metaphyseal diaphyseal junction and radiographic follow-up to monitor fracture alignment. Physeal fractures in adolescents and intra-articular fractures in children of all ages should be anatomically reduced. We perform most of our osteosyntheses with K-wires.
Introduction
Distal forearm fractures comprise up to 30% of all pediatric fractures. The peak incidence is at 10 years of age. Clinical findings include swelling and tenderness, and visible deformity in displaced fractures. Diagnosis is confirmed and the fracture type is determined with plain radiographs. Treatment decisions are based on patient’s age, type of the fracture, and surgeons preference. Despite the fact that distal forearm is the most common fracture location in children, there is little consensus about treatment and follow-up protocols of these injuries. We present authors’ preferred treatment in different types of pediatric distal forearm fractures.
Fractures at the Distal Metaphyseal Diaphyseal Junction
Greenstick fractures occur at diaphysis or at distal metaphyseal diaphyseal junction. A greenstick fracture extends macroscopically through the entire bone causing angular malalignment, but no shortening. Radiographs show a visible gap in the cortex at the apex of the fracture. The opposite cortex is acutely bent, but in continuity, and the periosteum is intact on this side working as a hinge. Greenstick fractures are thus unstable in one plane and the deforming forces by the surrounding musculature may worsen angular alignment in the cast (1). It is thus advisable to check the alignment of most greenstick fractures once preferably 10–14 days after casting. This is not necessary in internally fixed fractures (Fig. 1).
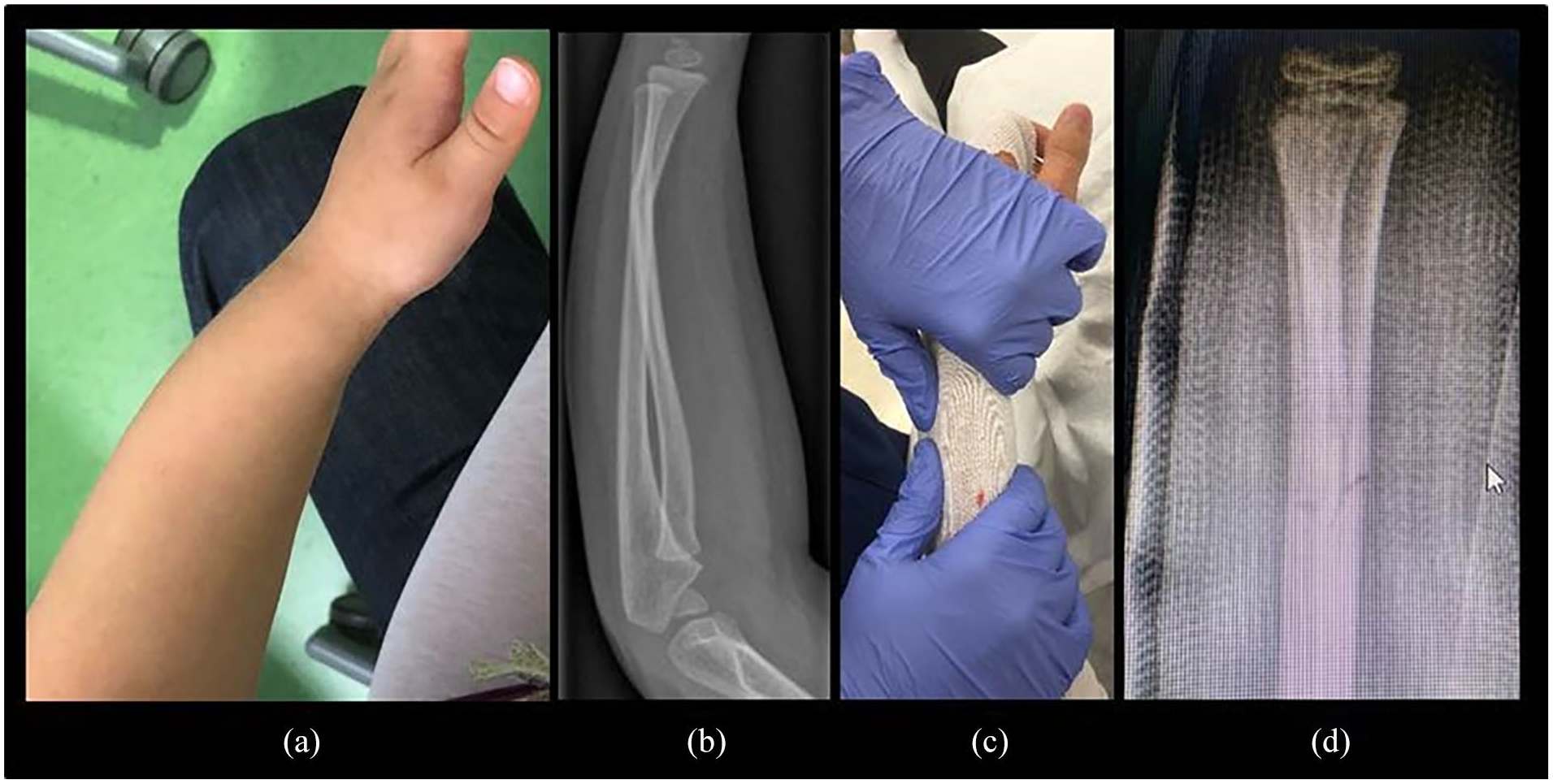
(a) Greenstick fracture at the distal diaphyseal metaphyseal junction in a 10-year-old girl. Visible apex dorsal angulation and restricted supination were clinical findings. (b) Radiographs show 20° of angulation. (c) Manipulation in local anesthesia and application of a synthetic circular cast with a three-point mold. Immobilization can also be performed with dorsal or dorsal and volar conventional or synthetic splints. (d) The authors would control the alignment with radiographs 7–10 days later. Cast can be removed in 4–5 weeks.
Distal Metaphyseal Fractures
Distal metaphysis is the most common site of forearm fractures in children. Most fractures in children at this location are incomplete torus or buckle fractures, which are characteristic to immature bone. The soft and flexible distal radius bends on the compressive side of the bone when a child breaks a fall with her hand. Buckle fractures are stable and there is no risk for displacement or increasing angulation. These fractures are best treated for a couple of weeks with a soft bandage, a manufactured universal wrist orthoses or individually molded dorsal splint, which all aim to decrease pain (1, 2). Routine follow-up is not necessary (Fig. 2).

(a) A 9-year-old boy’s buckle fracture of the distal radial metaphysis is best treated with (b) a removable custom-made synthetic orthosis for 2–3 weeks. A conventional dorsal plaster of Paris or a wooden splint is other options.
Complete fractures comprise around 20% of distal metaphyseal radius fractures in children. Fully displaced fractures leave the distal fracture fragment in an over-riding position, also called bayonet position, with shortening and angulation. Pin fixation can be used to stabilize the fracture after closed reduction. However, it has been questioned if reduction of over-riding distal radius fractures in children <11 years is necessary at all, because remodeling can correct shortening up to 10 mm and angulations up to 35° (Fig. 3). In general, remodeling can be counted as a part of definitive care, but this requires experience. There is no consensus concerning the “acceptable” alignment, treatment, and follow-up protocol of displaced distal metaphyseal forearm fractures in children (3). The authors’ preferred treatment guidelines are presented in Table 1.
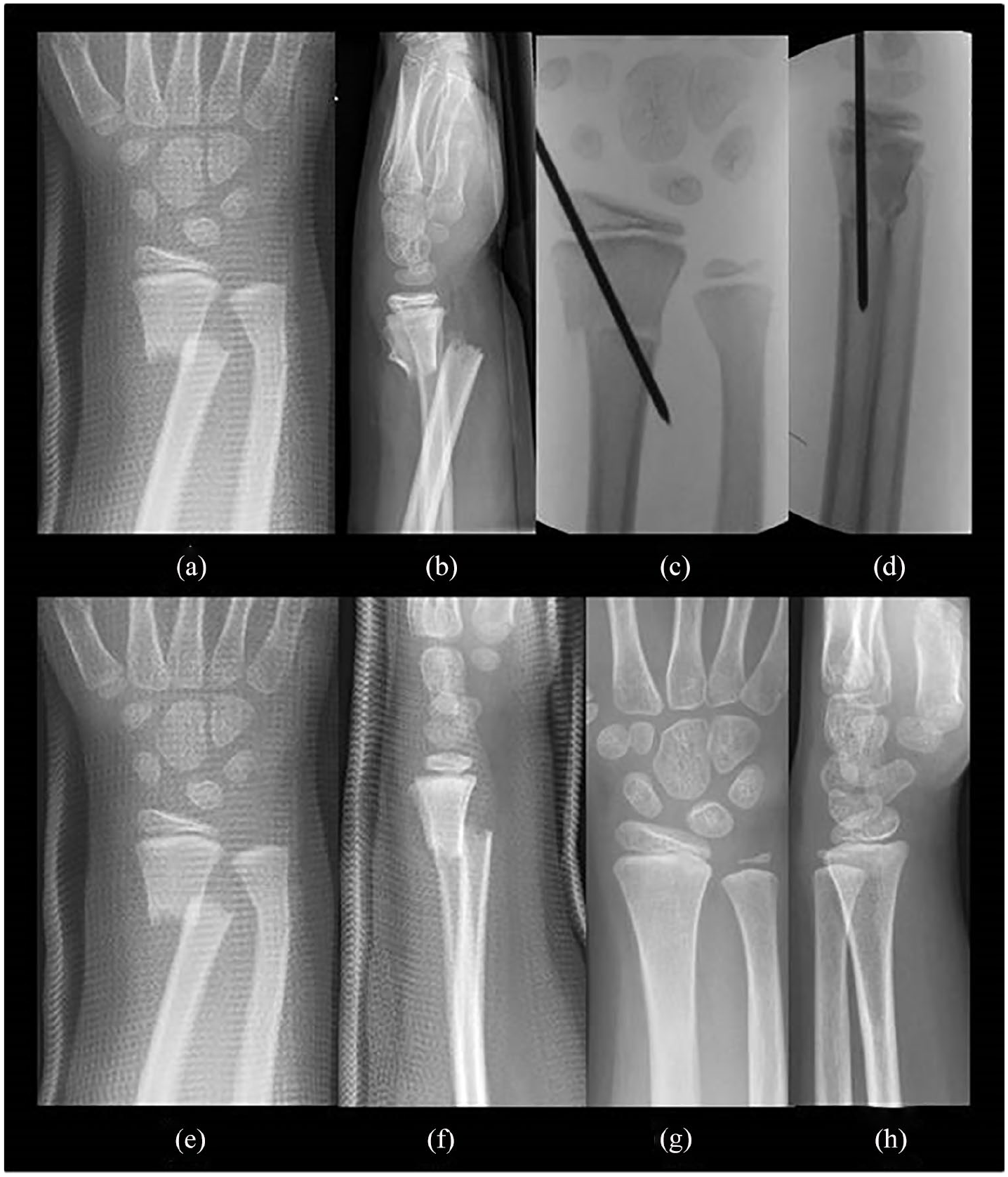
A 10-year-old boy had sustained a completely displaced distal metaphyseal radius fracture with a concomitant metaphyseal distal ulna fracture (a) and (b). His fracture was manipulated under anesthesia into anatomical alignment and stabilized percutaneously with smooth 1.8 mm pin (c) and (d). A complete displaced distal metaphyseal radius fracture with a greenstick fracture of the ulna in a 5-year-old boy has been immobilized with a cast in an over-riding position without local or general anesthesia (e) and (f). The cast was removed at 4 weeks and the boy had gained symmetrical forearm and wrist range of motion by 6 months. Radiographics 2 years later show complete remodeling of both bones (g) and (h).
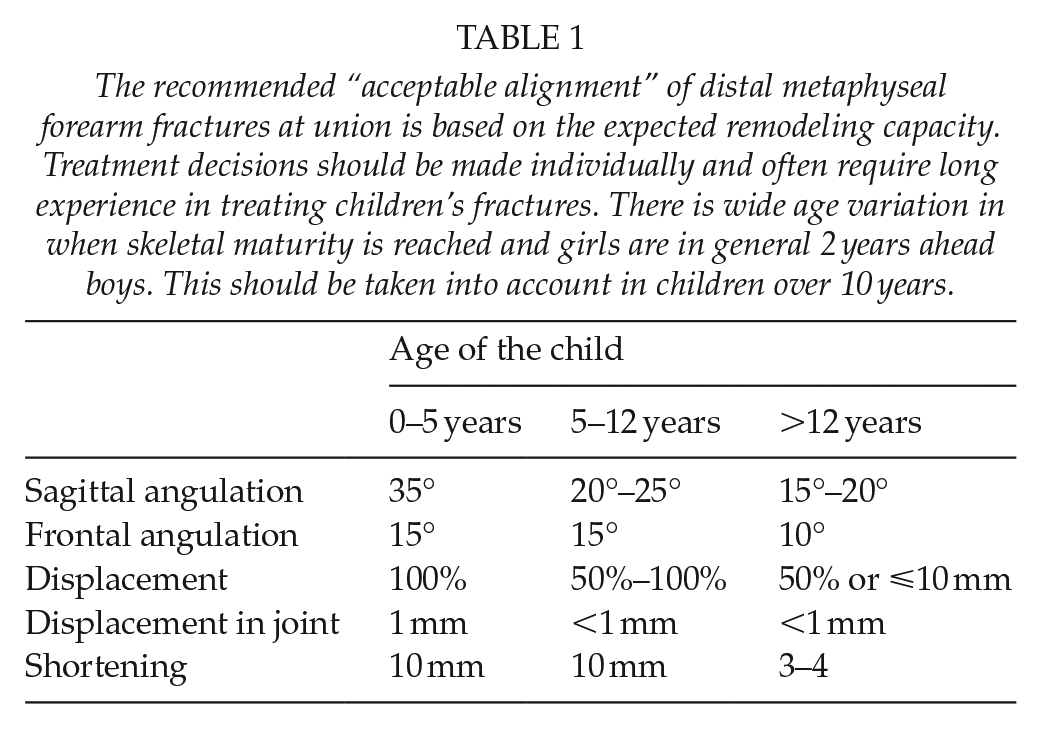
The recommended “acceptable alignment” of distal metaphyseal forearm fractures at union is based on the expected remodeling capacity. Treatment decisions should be made individually and often require long experience in treating children’s fractures. There is wide age variation in when skeletal maturity is reached and girls are in general 2 years ahead boys. This should be taken into account in children over 10 years.
Growth Plate Injuries
The distal radius growth plate is involved in approximately 20%–30% of all pediatric distal forearm fractures, whereas distal ulnar physis is rarely injured. The most widely used classification system for physeal injuries was popularized by Salter and Harris (S–H), but Peterson’s classification is more comprehensive. The fundamental idea of both classifications is to provide a method to predict the natural history of the fracture and to aid in choosing the optimal treatment strategy. J.-J.S. prefers to use the former, and Y.N. the latter. S–H types 1–2 and Peterson types 1–3 physeal injuries of the distal radius are benign in nature and the proliferative layer of the growth plate remains usually intact (Fig. 4). Fractures that split the distal epiphyses and extend to the joint (S–H 3–4 and Peterson 4–6) are rare. These fractures should be anatomically reduced and stabilized with internal fixation in order to avoid partial or complete physeal arrest and post-traumatic degenerative arthritis (Fig. 5). The overall risk of premature growth arrest in physeal injuries of the distal radius is low (<5%) and routine follow-up is not necessary in most S–H type 1–2 (Peterson 1–3) fractures (4). Nevertheless, all children who have sustained a physeal injury of the distal radius by high-energy trauma, or any physeal injury of the distal ulna, two or more years before skeletal maturity, should be seen 6 months after the injury to exclude growth arrest. In general, reduction of physeal fractures should be performed within a couple of days from the injury in order to avoid an iatrogenic damage to the physis. Therefore, young children presenting late with a displaced physeal injury are often best left without reduction.
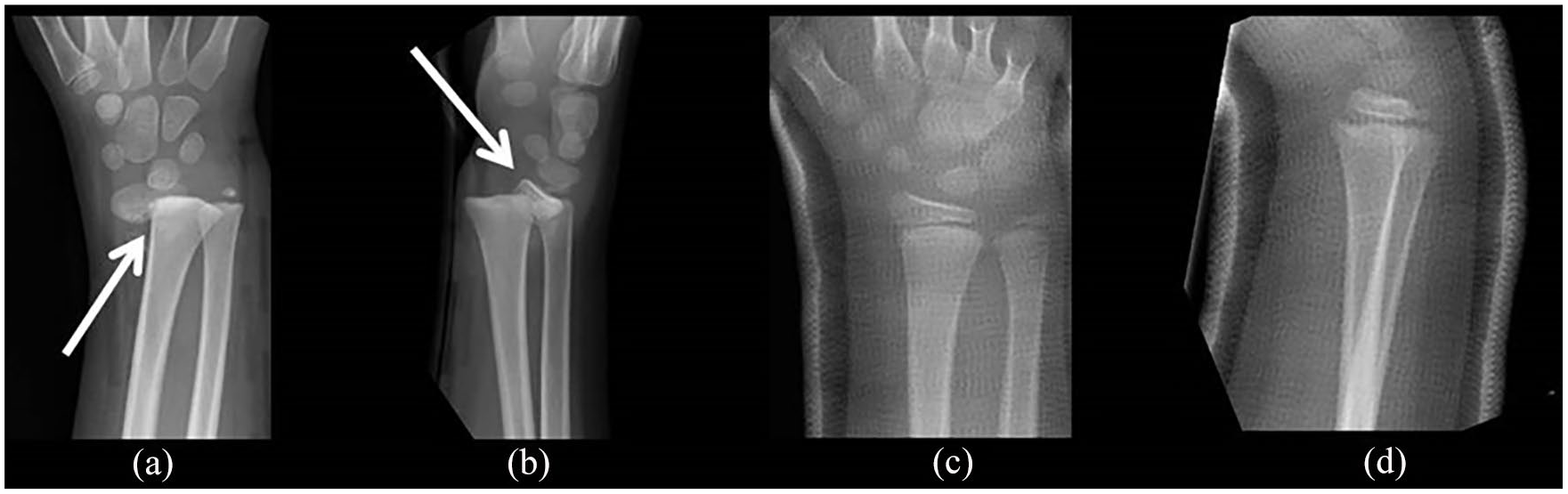
Anterior–posterior (a) and lateral (b) radiographs of an 8-year-old child who had sustained an almost completely displaced physeal fracture (white arrows) of the distal radius (Salter–Harris and Peterson type 2). Anterior–posterior (c) and lateral (d) radiographs after closed reduction under general anesthesia. Follow-up radiographs are unnecessary, because remanipulation is contraindicated even in case of partial loss of reduction in the cast.
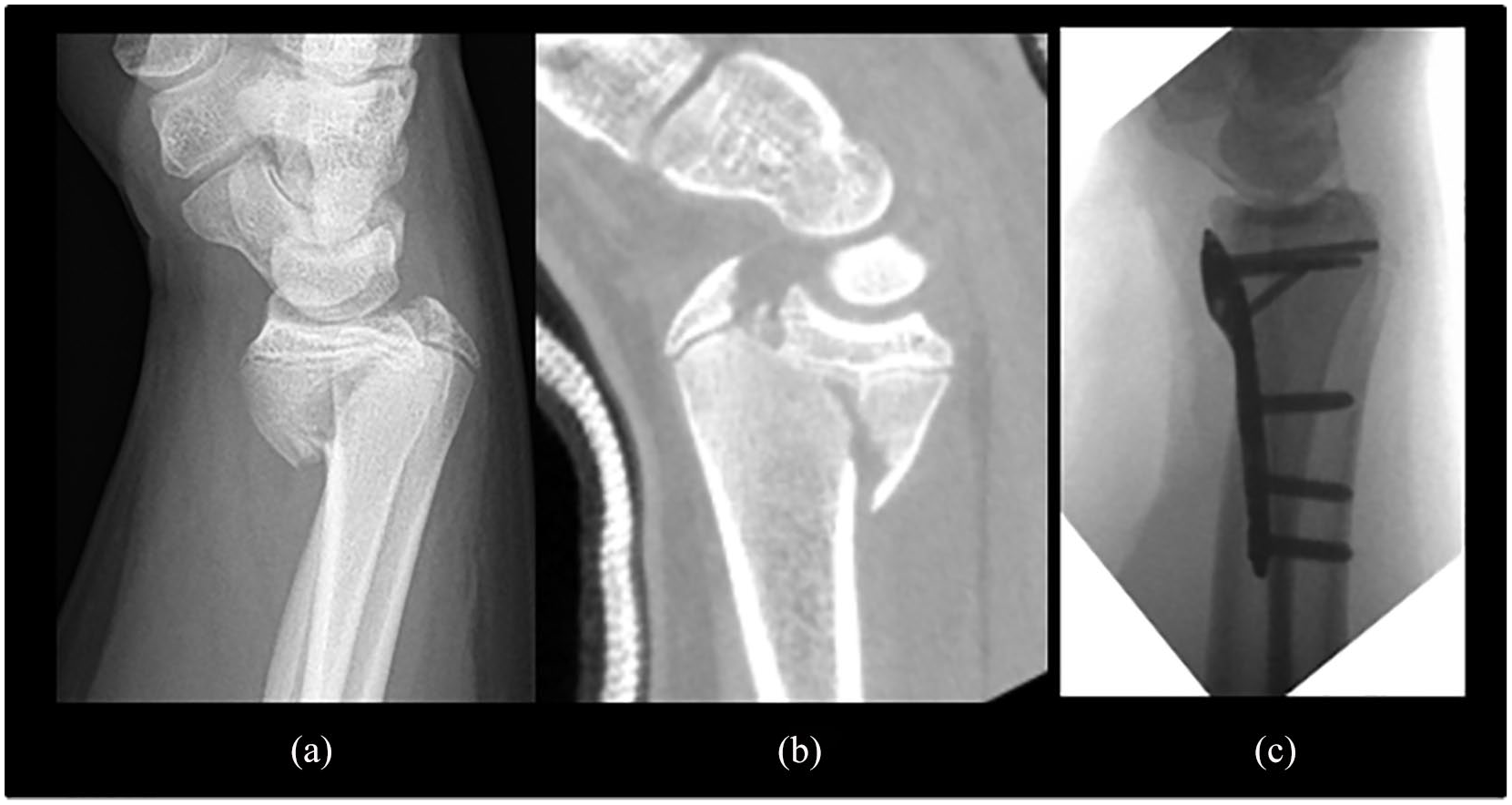
S–H 4 or Peterson 5 type distal radius fracture in a 15-year-old boy (pubertal status P4G4 referring to late adolescence), imagined by (a) a plain radiograph and (b) computer tomograph. (c) Open reduction and internal fixation with a locking plate. Joint surface has been well restored. Little further growth is expected and an acute physiodesis of the distal ulnar growth plate was considered unnecessary.
Concomitant Ulna Injury
Most displaced distal radius fractures have a concomitant ulnar injury, of which an avulsion type fracture of the distal ulnar styloid process (USP) is the most common. USP generally starts to ossify late at the age of 5–9 years; hence, up to 15% of the USP, fractures may be occult (5). USP fractures in children commonly result in non-union, which does not appear to cause much morbidity (5). The risk of growth arrest in physeal ulnar fracture is high (up to 50%), resulting in negative ulnar variance. Torus, greenstick, and complete fractures of the distal ulna are treated in the same manner as equivalent fractures of the distal radius. An apex dorsally angulated distal radius fracture can be associated with posterior dislocation of the ulnar head (Galeazzi fracture dislocation). The authors’ preferred treatment of these fractures is open reduction and plating of the radius. It is best to confirm that the distal radioulnar joint is congruent in the cast, for example, with cone beam computer tomography after surgery.
Casting
A below elbow splint or cast provides adequate support for most distal forearm fractures in children. Incomplete buckle or torus fractures are best treated with a removable soft-cast orthosis or a fabricated wrist immobilizer. J.-J.S. prefers to immobilize displaced distal forearm fractures in children with a wide plaster of Paris cast that covers both dorsal and volar sides of the forearm to provide a three-point support to the fracture. Y.N. prefers to use a synthetic circular cast in greenstick fractures and in reduced complete fractures. A synthetic above elbow dorsal and a below elbow volar splint in over-riding distal metaphyseal forearm fractures left in bayonet position in prepubertal children are the best choice according to both authors.
Internal Fixation
Both authors prefer manipulation under anesthesia if internal fixation is planned. We would both stabilize greenstick and complete distal metadiaphyseal fractures with a plate, for example, in a child who has sustained a Galeazzi fracture dislocation. We would use a four- or five-hole semitubular locking plate with two locking screws (four cortices) both proximal and distal to the fracture. We would both stabilize, if deemed necessary, metaphyseal and physeal fractures of the distal radius percutaneously, with one or two 1.6–2.0 mm smooth pins (6). We insert the first pin into the radial styloid and drill it through the physis, across the fracture into the proximal fragment piercing its ulnar cortex to obtain good stability. A second pin is not necessary in S–H 2 (Peterson 2) fractures, but adds to stability in metaphyseal fractures—we drill it either through Lister’s tubercle in sagittal plane or antegrade from radial to ulnar in frontal plane. Internal fixation of the radius only is usually adequate, even if the ulnar fracture is displaced. Intra-articular radius fractures should be anatomically reduced and stabilized with smooth pins or cannulated screws. Very badly comminuted intra-articular fractures that cannot be anatomically reduced and internally fixed can be stabilized with an external fixator to align forearm and wrist.
Conclusion
Distal forearm fractures comprise one-third of all fractures in children. We treat buckle fractures with a removable splint. Both authors recommend reduction and radiographic follow-up of greenstick fractures. Over-riding distal metaphyseal fractures of the radius can be internally fixed with percutaneous pins or casted in bayonet position in prepubertal children. Displaced physeal and metaphyseal fractures in adolescents should be well reduced and often stabilized with smooth pins.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. J.-J. Sinikumpu is assistant Editor of the Scandinavian Journal of Surgery.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No patients were contacted for this study purpose. No ethical board approval was needed. Clinical registration was not needed.