
Abstract
Background and Aims:
Loop ileostomies are frequently used as diversion of the fecal stream to protect a distal anastomosis. The aim of this study was to identify complications and morbidity related to loop ileostomies in patients with ulcerative colitis at a nonemergent setting.
Material and Methods:
Consecutive patients with ulcerative colitis who received a loop ileostomy at a tertiary referral center in Sweden from January 2006 until December 2012 were included and studied retrospectively.
Results:
In total, 71 patients were identified, and the median age was 39 years. A majority (94%) of the patients underwent proctectomy or proctocolectomy with primary construction of an ileal pouch–anal anastomosis. In total, 38 patients (54%) had one or more postoperative complications at index surgery. Stoma-related complications were seen in 49% where parastomal skin irritation was most common. In total, 18% of the patients were re-admitted due to morbidity related to the ileostomy, and the leading cause was high volume output. Complications related to closure were seen in 29% of the patients, and of these, 30% required surgical intervention. In total, five patients (7%) developed a symptomatic leakage in the ileo-ileal anastomosis. There was no mortality.
Conclusion:
Loop ileostomies in this young patient cohort resulted in considerable morbidity. Closure of the ileostomy was also associated with complications. Although the diverting loop ileostomy is constructed to decrease the clinical consequences of an anastomotic leakage, the inherent morbidity should be considered. Preventive measures for parastomal skin problems could improve results.
Keywords
Introduction
First-line treatment for ulcerative colitis (UC) is pharmaceutical. However, approximately 20% of the patients with UC will require a colectomy, due to refractory disease, intolerance to medical therapies, or development of neoplasia (1). Restorative proctocolectomy with ileal pouch–anal anastomosis (IPAA) has become the standard of care for elective surgery in UC. Most commonly, this is performed as a two- or three-stage procedure with construction of a loop ileostomy at the same time as construction of the ileal pouch (1, 2). It is believed that the diversion of the fecal stream allows for the more distal anastomosis to fully heal while decreasing the rate of pelvic sepsis and the clinical consequences of an anastomotic leakage (1, 3–6). In rectal cancer, a loop ileostomy has been shown to reduce complications related to anastomotic dehiscence after total mesorectal excision (7). However, the diverting loop ileostomy itself is associated with substantial morbidity with reported complication rates of 17%–66% (3, 6, 8, 9), and closure of the ostomy is associated with considerable risk for postoperative complications, with frequencies of 20%–40% and reoperation rates of 6%–15% (9–13).
The aim of this study was to identify complications and morbidity related to loop ileostomies in consecutive patients with UC undergoing elective surgery and to identify possible risk factors for severe complications at closure.
Material and Methods
Study Design
Patients
All consecutive patients with UC and an elective procedure including primary reconstruction or redo surgery with an IPAA who received a loop ileostomy between 1 January 2006 and the 31 December 2012 were identified using the Nordic Medical Statistical Committee (NOMESCO) Classification of Surgical Procedures Version 1.9 codes JFF10 and JFF11. To ensure that no patients were missed, the NOMESCO codes for stoma reversal (JFG00 and JFG20) were checked until the 31 August 2014. At the studied hospital, a diverting loop ileostomy was a standard procedure during IPAA surgery, and only three patients received an IPAA without a loop ileostomy during the study period. These patients were not included in the present analysis. A clinical record form (CRF) was used to retrospectively retrieve patient data from medical charts, including notes from the stoma nurse. All patient records were reviewed until 21 October 2014 or until death. Data were extracted regarding patient demography, primary diagnoses, and details of the surgical procedure (Table 1). In addition, surgical complications at index surgery and ileostomy closure as well as complications related to the loop ileostomy were registered.
Baseline characteristics.
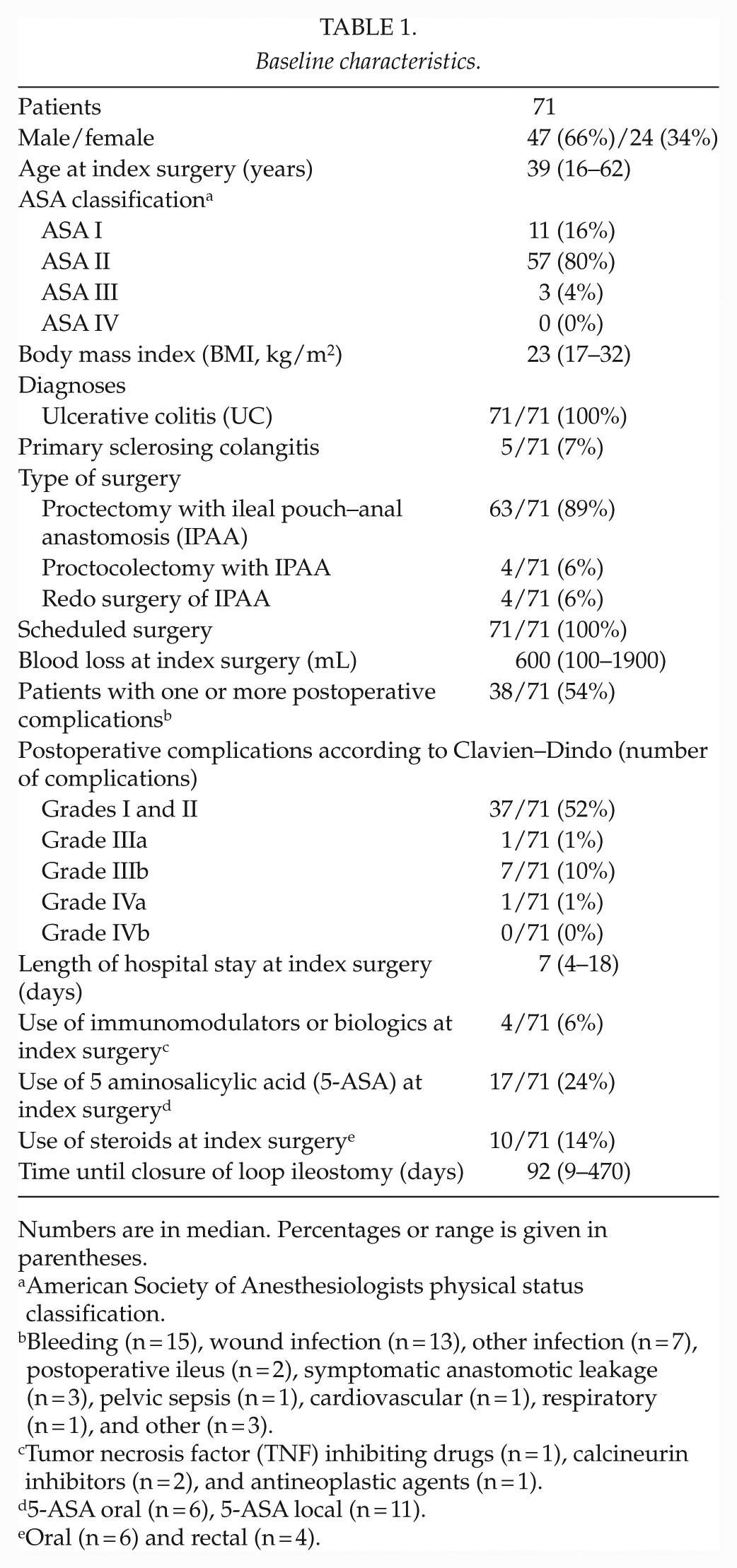
Numbers are in median. Percentages or range is given in parentheses.
American Society of Anesthesiologists physical status classification.
Bleeding (n = 15), wound infection (n = 13), other infection (n = 7), postoperative ileus (n = 2), symptomatic anastomotic leakage (n = 3), pelvic sepsis (n = 1), cardiovascular (n = 1), respiratory (n = 1), and other (n = 3).
Tumor necrosis factor (TNF) inhibiting drugs (n = 1), calcineurin inhibitors (n = 2), and antineoplastic agents (n = 1).
5-ASA oral (n = 6), 5-ASA local (n = 11).
Oral (n = 6) and rectal (n = 4).
Definition of Outcomes
Postoperative complications within 90 days were categorized according to the Clavien–Dindo grading system for the classification of surgical complications (14). To reduce the risk of misclassification, grades I and II were combined. Anastomotic leakage was defined as a symptomatic defect in the anastomosis regardless of the need for therapeutic intervention.
High volume output was defined as a stomal output exceeding 2000 mL/24 h from postoperative day 4 and onward, based on previous studies (13, 15). Postoperative ileus was considered a complication when being the cause for prolonged hospital care or readmission. Parastomal leakage was defined as stomal output outside the appliance bag, and skin irritation was considered a complication when being brought up as a problem at a minimum of two stoma nurse visits.
Statistical Analysis
The statistical analyses were performed with SPSS 21.0 (SPSS, Inc., Chicago, IL). Results are presented as median values with range in parentheses. Logistic regression was performed for multivariate analysis with risk factors for severe complications (Clavien–Dindo ≥ grade IIIa) at loop ileostomy closure. The initial list of prognostic factors to include in the multivariate analysis was decided using data from the literature together with clinical expertise including the factors: gender, body mass index (BMI; <25 respectively >25), comorbidity using the American Society of Anesthesiologists physical status classification (ASA) I and II respectively III and IV, and severe complications at index surgery not associated with the ileostomy (Clavien–Dindo ≥ grade IIIa).
Results
Baseline Demographics and Index Surgery
In total, 71 (24 females) patients were included in the study. Basic demography including preoperative morbidity is displayed in Table 1. A majority (94%) of the patients underwent proctectomy or proctocolectomy with primary construction of an IPAA. A total of 13% of the patients were being treated with immunosuppressants and/or systemic steroids. At index surgery, 54% of the patients had one or several postoperative complications, and the most common was perioperative bleeding requiring blood transfusion (21%) followed by wound infection (18%). For details regarding Clavien–Dindo classification of the complications, see Table 1. In total, three patients had a leakage in the IPAA and one patient suffered from pelvic sepsis, which was regarded as a probable anastomotic leakage. There was no relationship between the use of systemic steroids and/or immunosuppressant treatment with postoperative complications at index surgery.
Loop Ileostomy Complications
Complications related to the loop ileostomy were seen in 35 (49%) patients, and the majority were skin related (23%). High volume output (18%) was the main reason for readmission. The overall readmission rate was 18%.
Reoperation due to stoma-related complications during the loop ileostomy period was performed on two patients (3%). During the follow-up time, four patients (6%) developed a symptomatic hernia at the site of the previous stoma, which lead to surgical intervention. For details, see Table 2.
Loop ileostomy complications.
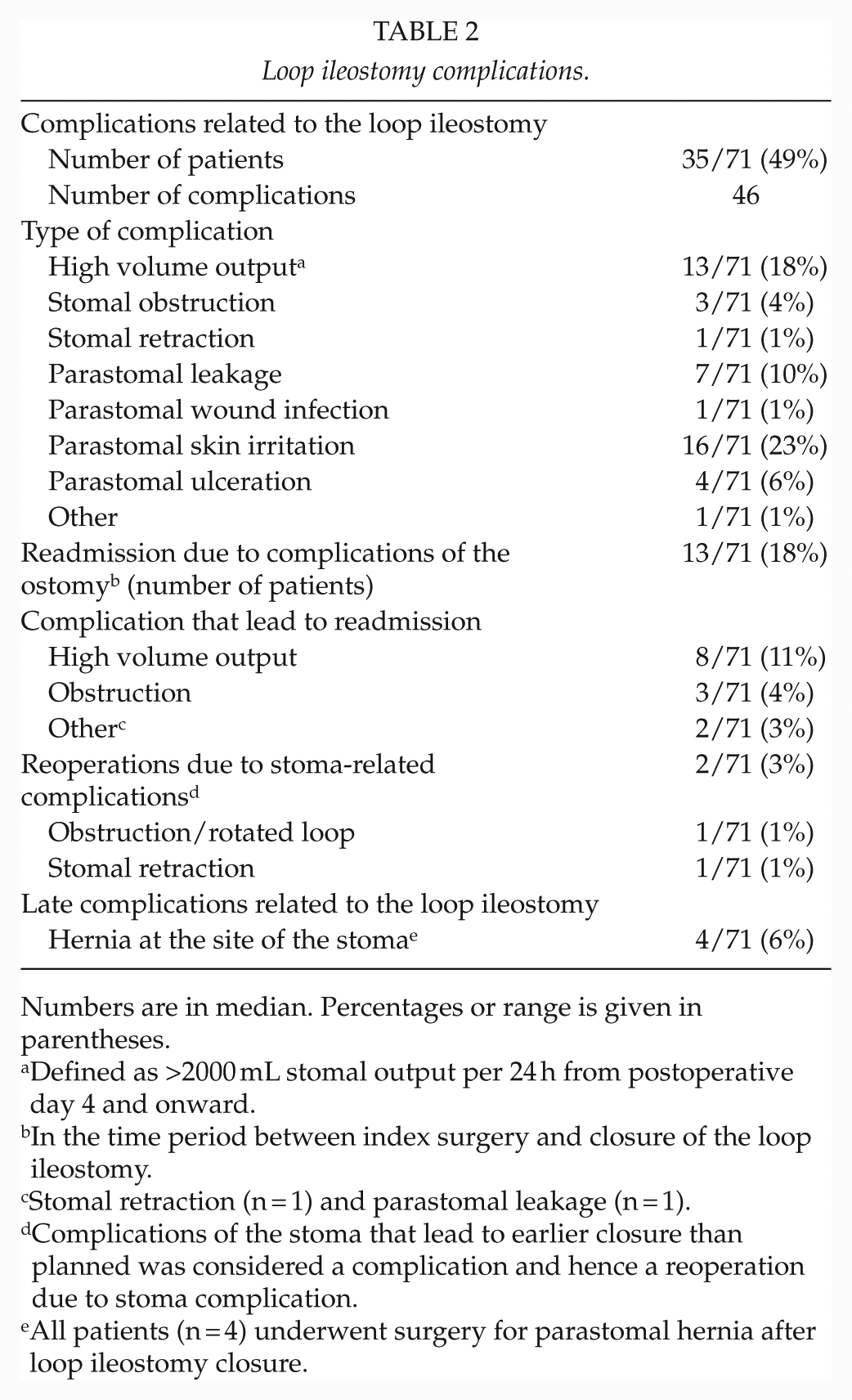
Numbers are in median. Percentages or range is given in parentheses.
Defined as >2000 mL stomal output per 24 h from postoperative day 4 and onward.
In the time period between index surgery and closure of the loop ileostomy.
Stomal retraction (n = 1) and parastomal leakage (n = 1).
Complications of the stoma that lead to earlier closure than planned was considered a complication and hence a reoperation due to stoma complication.
All patients (n = 4) underwent surgery for parastomal hernia after loop ileostomy closure.
Loop Ileostomy Reversal
The loop ileostomy was not reversed in one patient and one patient was lost to follow-up due to migration. Most patients (69/70) underwent both endoscopic examination and rectal enema radiographic sequence, and one patient underwent endoscopic examination and magnetic resonance imaging (MRI) prior to closure. Time until closure of the loop ileostomy was in median 92 days (9–470 days). Overall, post-closure complications were seen in 29% of the patients, with a majority being graded Clavien–Dindo grades I and II (Table 3). In total, six patients (9%) required a reoperation after closure, where one patient underwent two surgical procedures. The causes for reoperation were intraabdominal abscess (n = 1), leakage in the ileo-ileal anastomosis (n = 2), small bowel perforation (n = 1), obstruction of the ileo-ileal anastomosis (n = 1), wound rupture (n = 1), and unknown cause of peritonitis (n = 1). Symptomatic leakage in the ileo-ileal anastomosis was seen in five patients (7%), of whom two needed a reoperation. There was no mortality.
Loop ileostomy closure.
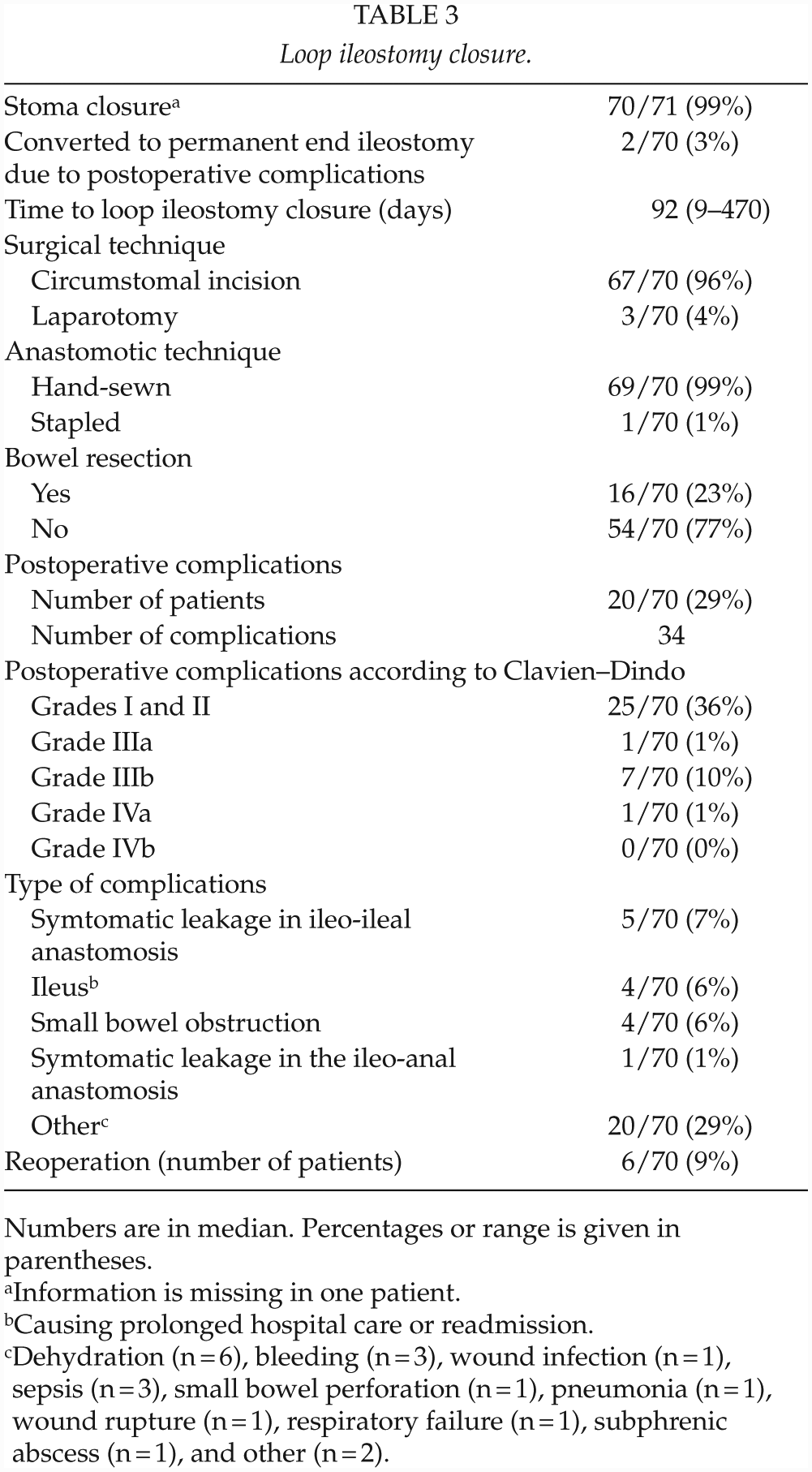
Numbers are in median. Percentages or range is given in parentheses.
Information is missing in one patient.
Causing prolonged hospital care or readmission.
Dehydration (n = 6), bleeding (n = 3), wound infection (n = 1), sepsis (n = 3), small bowel perforation (n = 1), pneumonia (n = 1), wound rupture (n = 1), respiratory failure (n = 1), subphrenic abscess (n = 1), and other (n = 2).
Risk Factors for Complications Related to Stoma Reversal
In multivariate analysis, there were no significant correlations found between prognostic factors and severe complications at index surgery or at stoma closure.
Discussion
This study confirms previous reports that the morbidity with a loop ileostomy and the complications at reversal are considerable in patients with patients with a loop ileostomy (3–6, 9–12, 16, 17). These findings are not new, but many of the previous reports have included a mixture of patients, combining diagnoses such as inflammatory bowel disease (both UC and Crohn’s disease) and colorectal cancer, the latter group consisting of patients that are often considerably older and more comorbid (7, 18). Our study solely includes patients with UC, a young, and apart from their inflammatory bowel disease, fairly healthy cohort, but still our data shows that the complication rates are somewhat discouraging. The reasons for these complications remain partly unknown. In the analysis, we did not find a correlation between postoperative complications and the use of systemic steroids and/or immunosuppressant treatment, although this is a well-known risk factor (19–21). The explanation might be the low number of patients on medication at the time for reconstructive surgery, as they were mainly two- or three-stage procedures.
Some authors have suggested that the loop ileostomy could be omitted in selected cases (16, 22). Zittan et al. (23) have recently suggested this, where a retrospective review of 460 patients indicates that it is possible to omit the loop ileostomy. These results are from a highly specialized center and may highlight the need for centralization of advanced surgery for UC. Still, an anastomotic leakage in the IPAA may be detrimental and render the patient with a lifelong permanent ileostomy or at least a severely affected bowel function. However, some reports have indicated that although the incidence of anastomotic leakage is higher without a loop ileostomy, if correctly treated, the patients may maintain bowel function and quality of life (24–26). Another approach could be to remove the loop ileostomy earlier, within the first 2 weeks after reconstructive surgery, as suggested in rectal cancer (27, 28). This would certainly reduce the stoma-related complications, and some studies also indicate a total reduction of complications in patients with early closure. In this study, one patient had their stoma reversed after 9 days. This was due to a strong request from the patient, and together with satisfying endoscopic and radiological investigation of the anastomosis and a postoperative uncomplicated clinical course, the decision was made to enable an early closure. Early closure was not a routine procedure.
Morbidity related to the stoma was mainly skin-related complications and high volume output, and as many as almost 1/5 of the patients were re-admitted due to stoma-related complications. It is possible that a more active postoperative follow-up as suggested by Nagle et al. (29) could reduce complications, improve patient quality of life, and decrease health-care consumption.
The strengths of this study are the consecutive elective patients at a single institution with data extracted by a single investigator reducing the risk for selection bias. A weakness of this study is the retrospective design and the inherent risk of missing information compared to a prospective collection of data.
In conclusion, we find that the morbidity related to a loop ileostomy and its reversal in otherwise fairly healthy patients with UC requires attention. Closer follow-up, shorter time with a stoma, and attention to potential risk factors at reversal must be addressed to reduce the morbidity in patients with UC.
Footnotes
Acknowledgements
The authors all contributed to conception and design of the study, interpreted data, performed analysis of data, revised the manuscript, and finally approved the manuscript for publication. Jennifer Park acquired most data and drafted this article. The authors would like to express their gratitude to David Bock, statistician, who assisted with the statistical analysis, as well as the rest of the staff at Scandinavian Surgical Outcomes Research Group (SSORG) in Gothenburg, Sweden.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Swedish Society of Medicine and the Agreement concerning research and education of doctors (ALFGBG-493341 and ALFGBG-526501) and Lisa and Bror Björnsson Research Foundation, Gothenburg, Sweden.
Ethical Approval
The Ethical Review Board in Gothenburg, Sweden, approved the research project EPN 399-14.