
Abstract
Background and Aims:
Colectomy due to ulcerative colitis is associated with complications. One severe complication is the risk for blow-out of the remaining rectal remnant. The aim of this study was to compare the frequency and severity of complications in patients with the rectal remnant left subcutaneously versus patients with the rectal remnant left intra-abdominally. A secondary aim was to identify risk factors for complications.
Materials and Methods:
Consecutive patients at two tertiary centers in Sweden were retrospectively reviewed regarding surgical procedures; complications classified according to Clavien–Dindo; and possible risk factors for complications such as preoperative medication, emergency surgery, and body mass index.
Results:
307 patients were identified. Minor complications were more common than previously reported (85%–89%). Severe surgical complications were not related to the handling of the rectal remnant. Leaving the rectal remnant subcutaneously was associated with local wound problems. Risk factors for severe complications were emergency surgery and preoperative medication with 5-aminosalicylic acid.
Conclusion:
Minor complications after colectomy for ulcerative colitis are very common and need to be addressed. Leaving the rectal stump intra-abdominally seems safe and may be advantageous to reduce local wound morbidity.
Introduction
Subtotal colectomy with ileostomy and preservation of the rectal remnant is the preferred surgical treatment for patients with acute severe colitis refractory to medical treatment (1, 2). In Sweden, the postoperative mortality rate after elective surgery is about 1%, but recent studies have shown mortality rates as high as 12.9% (3, 4) after emergency colectomies. The morbidity after surgery is high, especially after emergency surgery, with figures about 30%–40% (2, 5–9). The most commonly reported complications are perioperative bleeding, wound dehiscence, and small bowel obstruction. A more serious and less common complication is rectal stump blow-out. In patients with ulcerative colitis, the remaining rectum is often inflamed, thickened, and fragile, and the frequency of rectal stump blow-out is reported to be between 6% and 12% (1, 10–12).
The management of the rectal remnant remains somewhat controversial. The method of choice varies between hospitals and surgeons. One option is to close the rectal remnant and leave it in the abdomen. This has been thought to increase the risk of pelvic sepsis due to rectal stump blow-out, but results from retrospective studies have been controversial, and it is unclear if the placement of the rectal remnant in the small pelvis increases the risk of pelvic sepsis (1, 12, 13).
Another option involves creating a mucous fistula by exteriorizing the rectal remnant, and a third option is to anchor the closed rectal remnant to the abdominal wall, placing it within the subcutaneous tissue (14). The latter two necessitate a somewhat longer stump (rectosigmoid remnant) but are considered safe choices, because no closed bowel is left in the abdomen (15). It simplifies the subsequent identification of the rectum at a second surgery, but the mucous fistula leaves the patient with two ostomies, which is not easily managed. Anchoring the rectal remnant to the abdominal wall has been associated with a higher frequency of wound infections and insufficient healing (12). The introduction of the laparoscopic technique has further increased the interest in the handling of the rectal remnant, as it is technically more difficult to place the rectal remnant in the subcutaneous tissue during a laparoscopic procedure (16).
The aim of this study was to compare the frequency and severity of complications between patients with a rectal remnant left subcutaneously and those where the rectal remnant was left intra-abdominally. A secondary aim was to identify the risk factors for postoperative complications.
Materials and Methods
Study Design
This is a retrospective cohort study of patients with ulcerative colitis who underwent subtotal colectomy at two university hospitals in Sweden between February 1999 and December 2015. Patients were identified using the hospital administration systems using the International Classification of Diagnosis codes (ICD-10) K51.0, K51.5, K51.8, and K51.9 in combination with the Nordic-Medico Statistical Committee (NOMESCO) codes JFH 10 and JFH 11. The review was performed in 2016 using patient charts and operative notes.
The patients had their rectal remnant either (1) closed with staples with or without anchoring sutures and left in the abdomen or (2) closed with staples with or without anchoring sutures and then anchored to the abdominal fascia and left subcutaneously. No patients had an intentional mucous fistula. The choice of technique was at the discretion of the surgeon. Both hospitals employed the same routine of washing out the rectal remnant and using a drain in the remnant for the first days postoperatively in patients with the rectum left intra-abdominally. A case record form (CRF) was used for follow-up and included all patient characteristics, perioperative variables, and the postoperative outcome. Follow-up for postoperative complications was 90 days.
All the included patients had surgery due to ulcerative colitis. The indications were acute colitis, chronic refractory disease, or dysplasia/malignancy. Both laparoscopic and open colectomies, as well as emergency and elective operations, were reviewed. Acute operations were defined as surgery within 48 h of the decision to operate having been made.
Patient characteristics such as age, sex, and body mass index (BMI), as well as American Society of Anaesthesiologists (ASA) classification, steroids and 5-aminosalicylic acid (5-ASA) within 2 weeks of surgery, thiopurines within 30 days preoperatively, and anti-tumor necrosis factor (anti-TNF) treatment within 2 months of surgery were reviewed (17, 18). The timing of medications in relation to surgery were based on both the literature and clinical experience. Perioperative data extracted from patient charts included operating time, surgery during office hours or not, bleeding, emergency (surgery performed within 48 h after the decision was taken) versus elective surgery as well as wash-out of and perioperative handling of the rectal remnant. Postoperative data extracted from patient charts were hospital stay (days), postoperative complications within 90 days of surgery (blow-out of the rectal remnant; deep or superficial infections; thromboembolism; and cardiac, urinary, or chest infections), re-operations, re-admissions, stoma-related problems (defined as one or more of the following: wound infection, skin irritation, parastomal ulceration, stoma necrosis, stoma prolapse, parastomal hernia, obstruction, leakage, and high volume output defined as more than 2 L per day), symptoms from the remaining rectum (bleeding, secretion, dehiscence, or healing problems of the surgical wound close to the rectal remnant), and mortality. The postoperative complications were graded according to Clavien–Dindo (19). To reduce the risk for misclassification, as all data were extracted from patient charts, Clavien–Dindo I–IIa were combined during collection of data as done previously (20). For analysis, Clavien–Dindo I–IIIa complications were considered to be minor complications and Clavien–Dindo IIIb and higher were combined and considered to be severe morbidity, as this required surgical intervention or intensive care treatment.
End Points
The primary end point was severe morbidity comparing the two different ways of handling the rectal remnant, classified as Clavien–Dindo IIIb and higher.
Ethical Aspects
The University of Gothenburg Ethical committee, EPN013-16, approved the study.
Statistical Analysis
SPSS computer software (version 23) was used for statistics. For univariate analysis, Pearson’s Chi-square and Fisher’s exact test were used for categorical variables, Mann–Whitney was used for continuous variables, and a P-value < 0.05 was considered statistically significant. This was an explorative analysis, and correction for multiplicity was not performed. No imputation for missing values was performed. Multivariate analysis was performed using logistic regression including all known possible risk factors for complications such as age, BMI, operating time, bleeding, emergency versus elective surgery, handling of the rectal remnant, steroids within 2 weeks of surgery, anti-TNF therapy within 2 months of surgery, 5-ASA medication within 2 weeks of surgery, and thiopurines within 30 days preoperatively.
Results
In total, 307 patients were identified and stratified according to the handling of the rectal remnant (Table 1). In 144 patients, the rectal remnant was left subcutaneously (subcutaneous groups), and in 157 patients, the rectal remnant was left intra-abdominally (intra-abdominal group). The median BMI was higher in the intra-abdominal group (Table 1).
Demographic and clinical data.
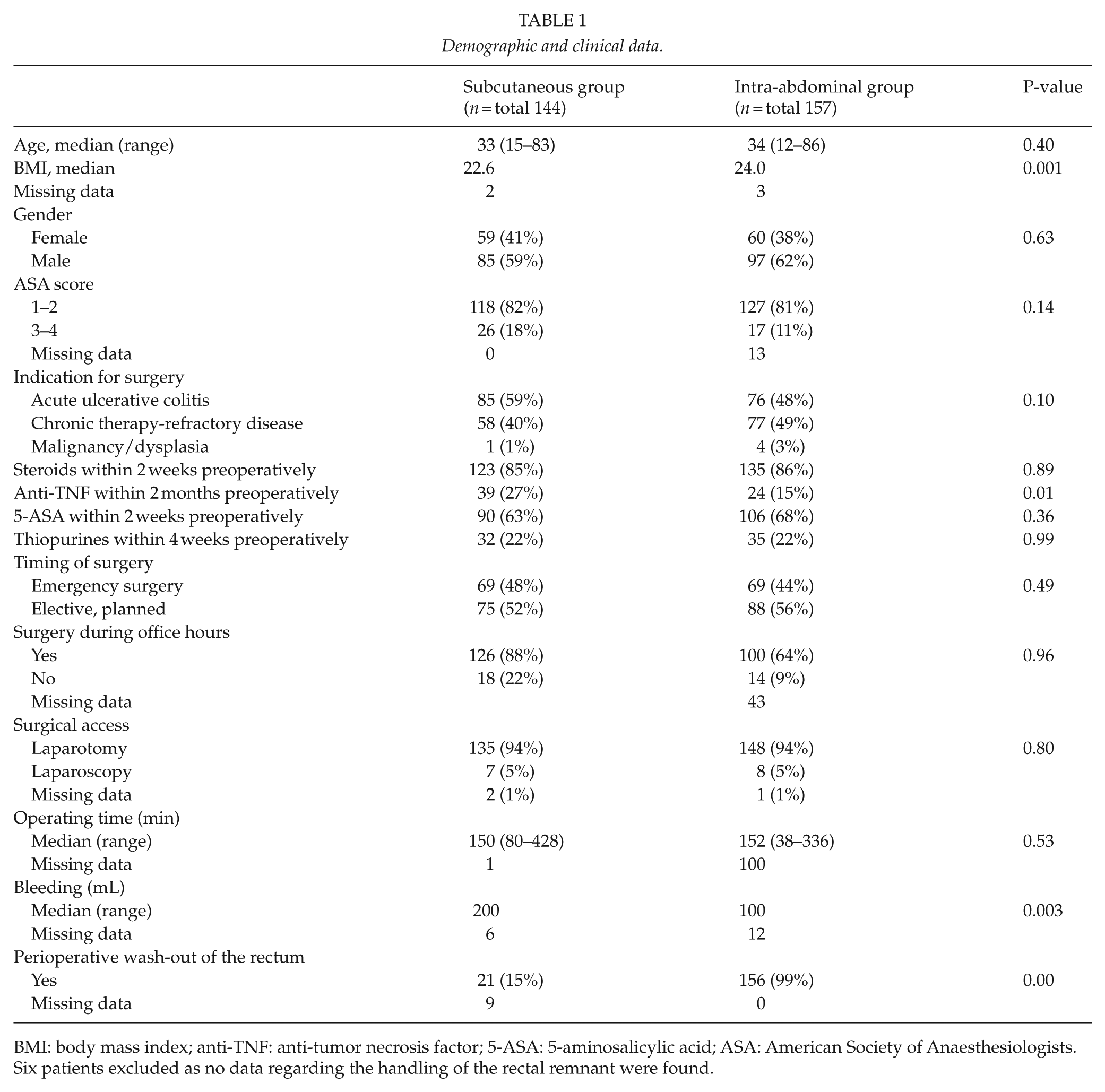
BMI: body mass index; anti-TNF: anti-tumor necrosis factor; 5-ASA: 5-aminosalicylic acid; ASA: American Society of Anaesthesiologists.
Six patients excluded as no data regarding the handling of the rectal remnant were found.
The use of TNF inhibitors preoperatively was more common in the subcutaneous group, apart from which the groups did not differ regarding preoperative medication such as steroids, 5-ASA, or thiopurines. The surgical details for the groups were similar, but the median amount of blood loss was higher in the subcutaneous group (Table 1). Perioperative wash-out of the rectum was much more common in the intra-abdominal group. Postoperative outcomes are shown in Table 2; there were more stoma-related problems and local problems with the rectal remnant in the subcutaneous group. The groups had similar postoperative complications graded according to Clavien–Dindo (Table 2). There was no statistical difference between minor (Clavien–Dindo I–IIIa) or major (Clavien–Dindo IIIb–IVb) complications between the two groups.
Postoperative outcomes.
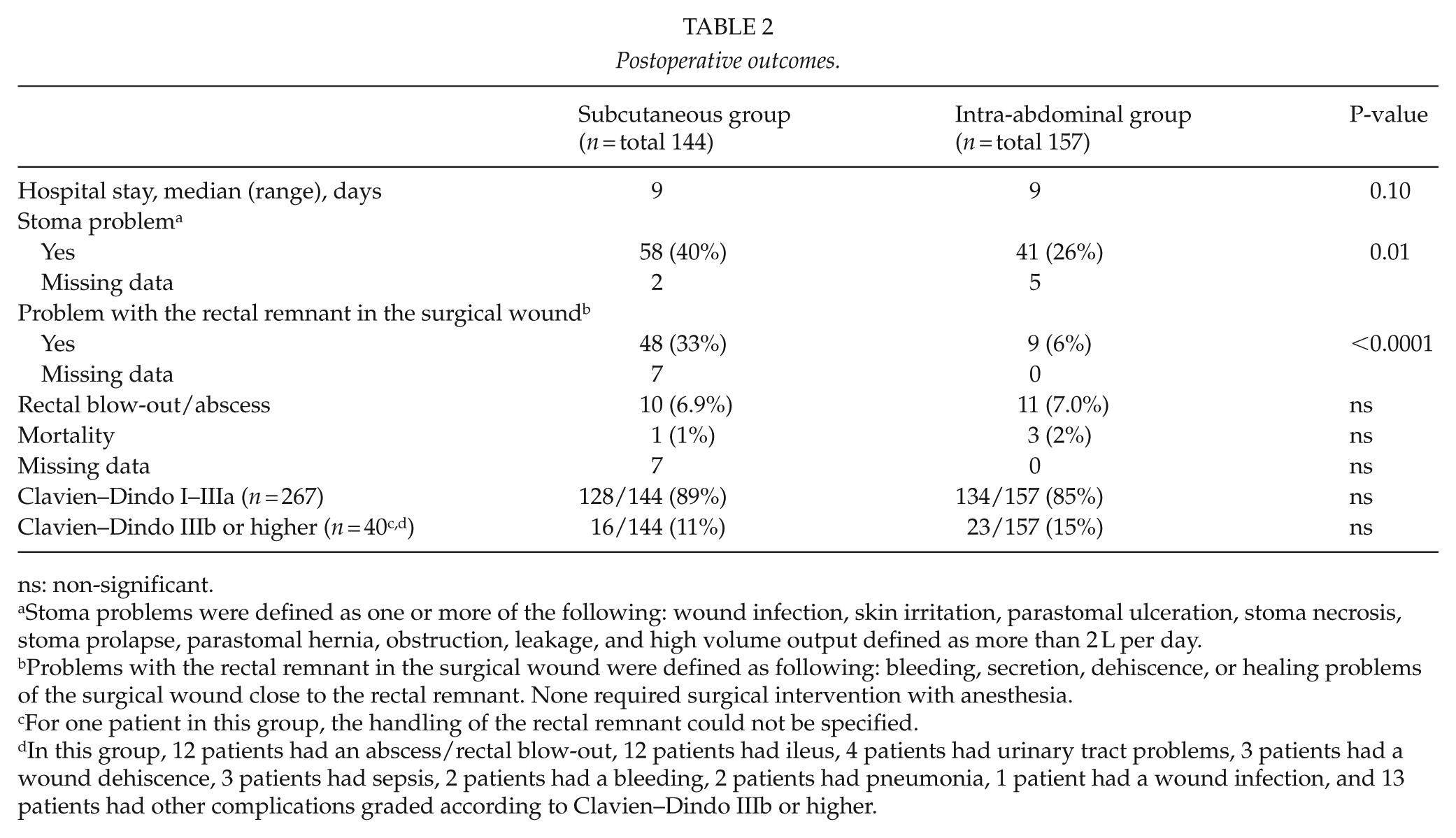
ns: non-significant.
Stoma problems were defined as one or more of the following: wound infection, skin irritation, parastomal ulceration, stoma necrosis, stoma prolapse, parastomal hernia, obstruction, leakage, and high volume output defined as more than 2 L per day.
Problems with the rectal remnant in the surgical wound were defined as following: bleeding, secretion, dehiscence, or healing problems of the surgical wound close to the rectal remnant. None required surgical intervention with anesthesia.
For one patient in this group, the handling of the rectal remnant could not be specified.
In this group, 12 patients had an abscess/rectal blow-out, 12 patients had ileus, 4 patients had urinary tract problems, 3 patients had a wound dehiscence, 3 patients had sepsis, 2 patients had a bleeding, 2 patients had pneumonia, 1 patient had a wound infection, and 13 patients had other complications graded according to Clavien–Dindo IIIb or higher.
Our secondary aim was to look at risk factors for severe complications (graded Clavien–Dindo IIIb or higher). The only significant risk factors identified were emergency surgery and the use of 5-ASA medication 2 weeks prior to surgery (Table 3).
Risk factors for postoperative complications.
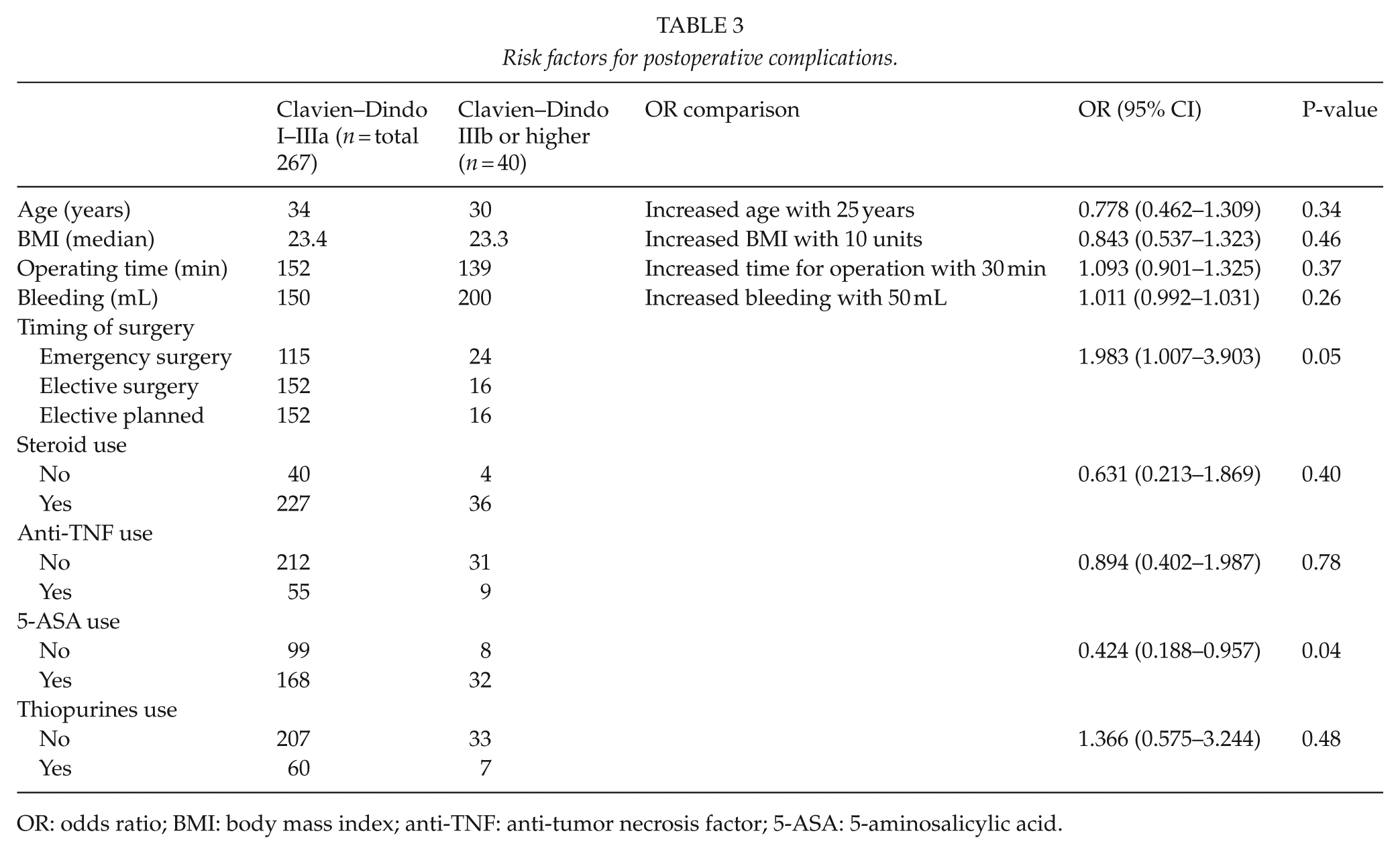
OR: odds ratio; BMI: body mass index; anti-TNF: anti-tumor necrosis factor; 5-ASA: 5-aminosalicylic acid.
Discussion
This large study of consecutive patients with ulcerative colitis shows that the handling of the rectal remnant did not affect the risk of severe complications. There was a low risk of rectal blow-out or intra-abdominal infection regardless of whether the rectum was subcutaneous or left in the abdominal cavity.
The morbidity after colectomy for ulcerative colitis is high, as previously reported (8), but in our study, the rate of minor complications is much higher than in most other reports. In our cohort, many patients had deviations related to postoperative analgesia, and the findings indicate that the complications could be reduced substantially with an improved plan of postoperative analgesics.
We found that many patients in the subcutaneous group had local problems in the wound related to the rectal remnant. Many of the patients are left with a second stoma, which may cause considerable morbidity over a long period of time. This has been reported previously (13), and measures such as rectal wash-out have been suggested (21) to reduce these symptoms. In our series, this did not change the outcome, but it was performed in few patients in this group, which makes it difficult to reach firm conclusions. Still, as we could not find any data to support that leaving the rectum subcutaneously reduced the amount of severe complications, it is possible that leaving the rectal remnant intra-abdominally could improve the quality of life postoperatively.
Possibly emergency surgery could be a risk factor for complications, but previous studies have shown high dose steroids, low albumin, low BMI, and long duration of active disease prior to surgery to be of more significance, and thus, long-standing duration of active disease prior to surgery might be of equal, or greater, importance than if the surgery was performed within 48 h or not (6, 22–24). In our study, the number of patients who had emergency surgery was similar in both groups, and we have chosen not to perform any further analysis regarding this.
We found that many patients have complications related to their stoma. This has been seen previously in patients with inflammatory bowel disease and loop ileostomies (25), but must also be acknowledged in this patient group, as the stoma may be a permanent stoma in more than half of the cases (26). This study does not include the details regarding reconstruction and removal of the stoma. It is possible that it is easier to perform an ileorectal anastomosis if the rectal remnant is subcutaneous as it may be easier to find. Apart from this, the handling of the rectal stump probably does not affect the timing and the type of reconstruction.
One of the strengths of this study is the inclusion of consecutive series of patients at two tertiary referral centers. The collection of data was improved by the predefined clinical record form. The long study period is a strength, as it involved a large number of patients, but implementation of laparoscopic surgery only began during the period covered by the study and is reflected by the large number of open procedures.
Limitations include the retrospective design, as data may be misinterpreted or not accessible. It is also possible that some complications were missed due to insufficient reporting. Additional follow-up with quality of life data would further improve our understanding of the postoperative and long-term morbidity in patients who undergo subtotal colectomy due to ulcerative colitis. The long time period of inclusion (16 years) may have affected the result, which must be taken into account when interpreting the data.
In summary, we conclude that it may be advantageous to avoid leaving the rectal stump subcutaneously, as it often raises concern regarding local wound complications, may create a secondary stoma, and does not seem to reduce the risk for severe complications.
Footnotes
Acknowledgements
Data from the research can be accessed by contacting the authors.
Author Contributions
M.L., S.O., P.M., M.B., and E.A. designed the study. M.L. and S.O. collected the data; M.L. and E.A. analyzed the data; M.L., S.O., P.M., M.B., and E.A. interpreted the results; M.L. and E.A. drafted the article; M.L., S.O., P.M., M.B., and E.A. all critically revised the article and gave final approval for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The University of Gothenburg Ethical committee, EPN013-16, approved the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Sahlgrenska Academy supported this research, which was performed for a Master’s thesis. Sahlgrenska University Hospital, agreement concerning research and education of doctors: ALFGBG-493341 and ALFGBG-426501.