
Abstract
Background and Aims:
Implementation of a clinical risk score into diagnostics of acute appendicitis may provide accurate diagnosis with selective use of imaging studies. The aim of this study was to prospectively validate recently described diagnostic scoring system, Adult Appendicitis Score, and evaluate its effects on negative appendectomy rate.
Material and Methods:
Adult Appendicitis Score stratifies patients into three groups: high, intermediate, and low risk of appendicitis. The score was implemented in diagnostics of adult patients suspected of acute appendicitis in two university hospitals. We analyzed the effects of Adult Appendicitis Score on diagnostic accuracy, imaging studies, and treatment. The study population was compared with a reference population of 829 patients suspected of acute appendicitis originally enrolled for the study of construction of the Adult Appendicitis Score.
Results:
This study enrolled 908 patients of whom 432 (48%) had appendicitis. The score stratified 49% of all appendicitis patients into high-risk group with specificity of 93.3%. In the low-risk group, prevalence of appendicitis was 7%. The histologically confirmed negative appendectomy rate decreased from 18.2% to 8.7%, p<0.001, compared to the original dataset.
Conclusion:
Adult Appendicitis Score is a reliable tool for stratification of patients into selective imaging, which results in low negative appendectomy rate.
Keywords
Introduction
The more common use of imaging studies, especially computed tomography (CT), in the diagnostic workup of patients with suspected acute appendicitis has led not only to improved diagnostic accuracy but also to increased exposure to ionized radiation and diagnostic delay (1, 2).
In some institutions, imaging before surgery for suspected acute appendicitis is mandatory (3). In other institutions, imaging studies are used less and with no guideline leading to unacceptably high negative appendectomy rate (4). Recent evidence shows that selective use of CT imaging does not increase the rate of negative appendectomies compared to mandatory CT (5, 6).
The Implementation of a clinical risk score into the diagnostic pathway prevents over- and underuse of imaging studies in patients with suspected acute appendicitis (7). Scoring provides a method for selecting high-risk patients directly into surgery, low-risk patients to outpatient care, and intermediate-risk patients to further investigations. The existing diagnostic scores for suspected appendicitis lack either specificity or sensitivity to be used for stratification of patients in routine diagnostic workup (4, 7).
We have developed a new diagnostic score, the Adult Appendicitis Score (AAS), for adult patients with suspected acute appendicitis (8). The score takes into account the time passed between the beginning of the symptoms and diagnostics as well as the special challenges in diagnosis of fertile-aged women. The score was implemented into the routine clinical pathway in two hospitals during the fall 2014 with the aim to validate the AAS in two relatively different hospitals as a part of emergency room routines. In both study hospitals, there was underuse of imaging modalities in suspected acute appendicitis, and scoring was implemented to reduce negative appendectomy rate with increased but selective use of imaging. The accuracy of the diagnosis was compared to the period before introducing the score.
Methods
Patients
The data were prospectively collected in surgical emergency departments of two university hospitals, the biggest (hospital A) and the smallest (hospital B), in Finland from September 2014 to May 2015. All adult (aged 16 years or more) patients admitted to these two health care facilities for right lower quadrant abdominal pain or suspected acute appendicitis (AA) were included in this study. The reference population comprised 829 patients with suspected acute appendicitis. The patient data of reference population were originally prospectively collected in hospital A during 2011–2012 for the construction of the score with detailed characterization in the original article (8). The institutional review board approved the study design.
AAS (Table 1) was introduced as a simple web-based application that collects the necessary information, calculates the score, and based on the scoring result stratifies patients into low-, intermediate-, and high-risk groups for appendicitis. The application thereafter suggested surgery without imaging studies for the high-risk patients, imaging for the intermediate-risk patients, and no imaging studies for the low-risk patients. In case of imaging, ultrasound was recommended as a primary method for patients younger than 35 years followed by CT if no diagnosis was established. In patients aged 35 years or older, CT was recommended as a primary method for imaging. In pregnant patients, magnetic resonance imaging was recommended instead of CT.
Adult Appendicitis Score (AAS): score ⩽10 low risk of appendicitis, score 11–15 intermediate risk of appendicitis, and score ⩾16 high risk of appendicitis.
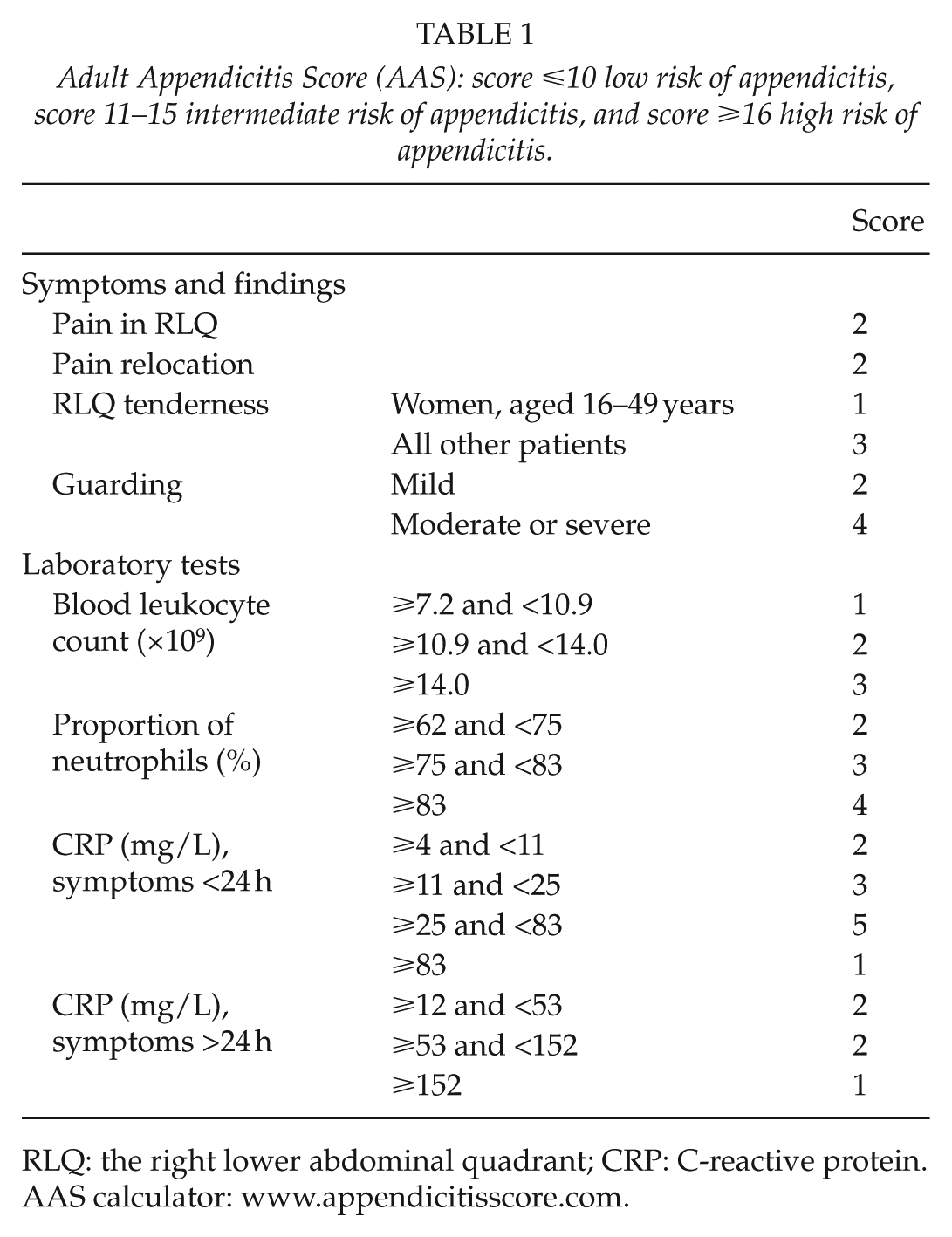
RLQ: the right lower abdominal quadrant; CRP: C-reactive protein.
AAS calculator: www.appendicitisscore.com.
Fig. 1 illustrates a flowchart of the clinical pathway of the study.
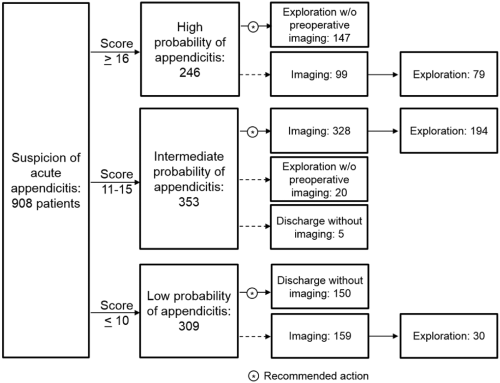
Patients’ flow during the study. In case of imaging, ultrasound was recommended as a primary method for patients younger than 35 years followed by computed tomography (CT) if no diagnosis was established. In patients aged 35 years or older, CT was recommended as a primary method for imaging. In pregnant patients, magnetic resonance imaging was recommended instead of CT.
After initial physical examination and laboratory tests, the physicians and surgeons at the emergency departments used the application as a diagnostic tool. Imaging was available at all times; the recommendations based on the score were not mandatory and physicians had the option to order imaging studies based on their clinical suspicion. However, during the study period, scoring was mandatory for all patients suspected of acute appendicitis.
The patient data necessary for calculation of the score for this study were retrieved from the scoring application. Further information concerning patient characteristics, imaging, surgery, hospitalization, and final diagnoses, as well as possible complications were acquired from patient databases. The medical records were reviewed after a minimum of 1 month after hospital discharge for final histological diagnoses and possible complications or failures in diagnostics.
When performing surgery for suspected appendicitis, the appendix was at all times removed. The final diagnosis of acute appendicitis was based on histological examination showing transmural infiltration of neutrophils in the appendix with the exception of three patients who underwent non-operative treatment for appendiceal abscess in hospital B. In these patients, the diagnosis was based on CT findings. Complicated appendicitis was, for this study, defined as perforation with peritonitis or abscess detected during surgery or in three patients undergoing non-operative treatment, abscess detected on CT.
The aim of this investigation was to validate the AAS in two relatively different hospitals as a part of emergency room routines. The diagnostic performance of the score (specificity, sensitivity, likelihood ratios, and diagnostic odds ratio) was calculated. The negative appendectomy rate, perforation rate, and utilization of imaging were compared with the reference population.
Statistical Analysis
Statistical analysis was performed using SPSS® version 22 (IBM, Armonk, NY, USA).
Results
Patients
This study enrolled 908 patients. Median age was 31 (range: 16–86) years, and 556 (61.2%) of patients were women. Of these patients, 432 (47.6%) had appendicitis. The proportion of complicated appendicitis was 91 of 432 (21.1%). Altogether, 470 patients underwent surgery for suspected appendicitis. Three patients with appendiceal abscess were treated conservatively. Other specific diagnoses were found in 207 (22.8%) patients, whereas 292 (32.2%) patients had non-specific abdominal pain.
In the reference population, there were 829 patients with suspected appendicitis, and 392 (47.3%) of these patients had appendicitis. Median age was 32 (range 16–97) years, and 483 (58%) of patients were women.
Diagnostic performance of the aas
The specificity of AAS ⩾16 was 93.3% and the sensitivity 49.4%. The sensitivity in patients with the score ⩾11 was 94.7%, and the specificity 60.2%. The negative predictive value of AAS (likelihood of no appendicitis in the low-risk group) was 93% in this study. For more detailed information of the performance of the score, see Tables 2 and 3.
Adult Appendicitis Score results and appendicitis in hospitals A and B.
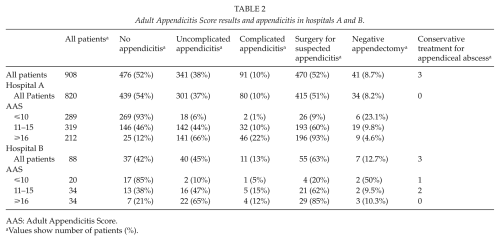
AAS: Adult Appendicitis Score.
Values show number of patients (%).
Adult Appendicitis Score in the diagnostics of acute appendicitis.
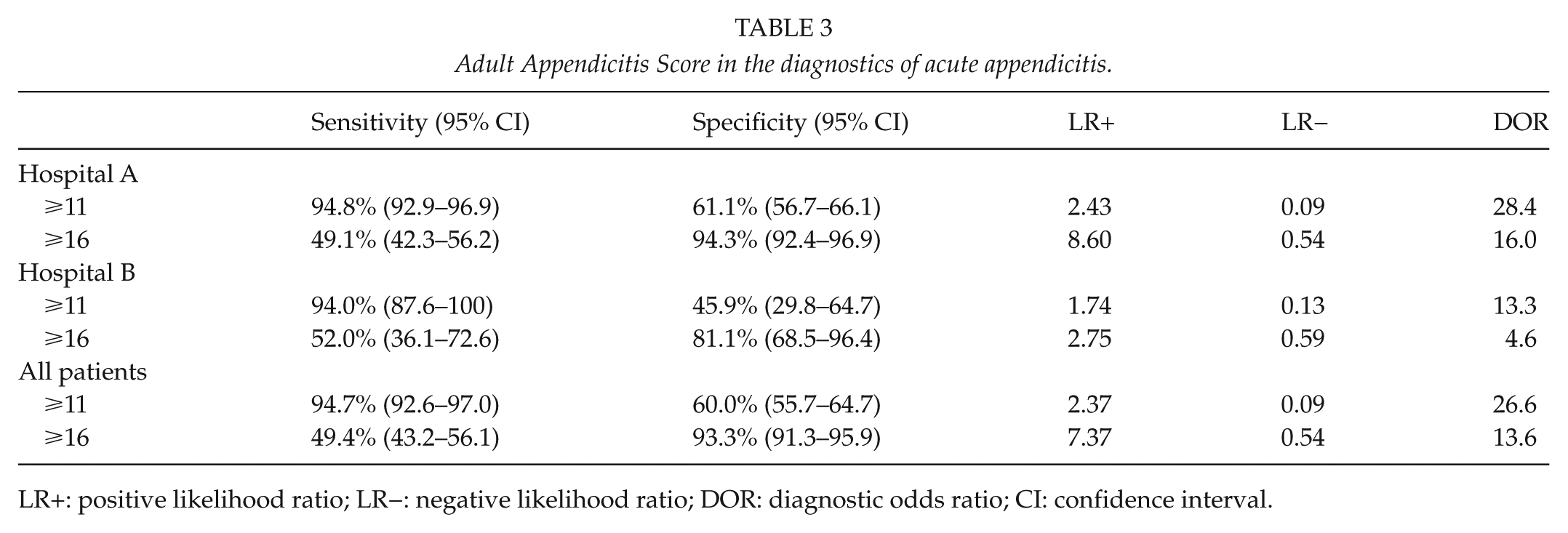
LR+: positive likelihood ratio; LR−: negative likelihood ratio; DOR: diagnostic odds ratio; CI: confidence interval.
High Risk, Aas ⩾16
Of all patients with appendicitis, 213 (49%) were stratified to the high-risk group. There were altogether 246 (27.1%) patients stratified to this group. Surgery for suspected appendicitis was performed on 225 patients. In 12 (5.3%) of these operations, no appendicitis was detected. A total of 99 (40%) patients underwent diagnostic imaging (Tables 2 and 3).
Intermediate Risk, Aas 11–15
In the group of possible appendicitis (AAS 11–15), there were 353 (38.9%) patients. Of these patients, 196 (56%) had appendicitis. These patients comprised 45% of all appendicitis patients. A total of 328 (93%) patients underwent diagnostic imaging (Tables 2 and 3).
Low Risk, Aas ⩽10
Of all patients, 309 (34.0%) had a score of 10 or less. Of these patients, 23 (7.4%) had appendicitis. There were no patients with perforated appendicitis and peritonitis in this group. Three patients had appendiceal abscess. A total of 159 (51%) patients underwent diagnostic imaging (Tables 2 and 3).
Negative Appendectomy Rate
The overall negative appendectomy rate was 41 (8.7%) out of 470. The lowest negative appendectomy rate 12 out of 225 (5.3%) was in the high-risk group, patients with AAS ⩾ 16 (p < 0.001). Furthermore, 3 of these 12 patients had other disease requiring emergency surgery, resulting in low rate (4%) of unnecessary operations in patients in the high-risk group. The highest negative appendectomy rate 8 of 30 (26.7%) was in patients with AAS ⩽ 10. Of these negative appendectomies, four (50%) were performed due to false-positive imaging results and four due to clinical suspicion despite negative preoperative ultrasonography (US) studies. Altogether, 13 negative appendectomies were performed due to clinical suspicion either without preoperative imaging or after negative or inconclusive imaging in the low- and intermediate-risk groups. In hospital A, after introduction of AAS, the rate of negative appendectomy was 34 of 415 (8.2%), whereas before the implementation of AAS the rate was 87 of 477 (18.2%) (p < 0.001, chi-square test). In patients operated on without preoperative imaging studies, negative appendectomy rate was after the introduction of AAS 15 of 167 (9.0%). Of these patients, two were in the intermediate probability group, and seven in the high probability group. Before the implementation of the score, the rate of negative appendectomy in patients without preoperative imaging was 59 of 263 (18.3%) (p = 0.002, chi-square test). The rate of complicated appendicitis was similar in the study population 91 of 432 (21%) and in the reference population 94 of 392 (24%), p = 0.32.
Diagnostic Imaging
In this study, 152 of 432 (35.2%) patients with AA underwent surgery without preoperative imaging. In the reference population, surgery was performed without preoperative imaging in 67% of patients with AA. Before the introduction of AAS, 20.9% of all patients suspected of acute appendicitis underwent CT, whereas during this study the proportion was 40.1%.
Discussion
This study showed that, with help of AAS, an acceptable rate of negative appendectomy was achieved without mandatory preoperative imaging. In this study, the rate of negative appendectomies in hospital A was significantly lower than before the introduction of the score. The diagnostic performance of the score was comparable to the performance in the original publication describing the construction of the score (8). After implementation of the AAS, the use of diagnostic imaging was increased in a controlled manner, helping to reduce the negative appendectomy rate.
Half of patients with appendicitis were stratified to high-risk group with the specificity of 93.3%, which is comparable to the specificity of CT. Therefore, mandatory imaging before surgery offers limited benefit in this group. In the low-risk group, there was high negative appendectomy rate, half of cases due to false-positive findings in imaging studies. Only 7% of patients in the low-risk group had appendicitis, no patients with peritonitis among them, suggesting that observation rather than mandatory imaging would be the best management in these patients in case appendicitis is clinically suspected despite the low scoring result. This leaves only the intermediate-risk group, 39% of all patients, to mandatory imaging.
In a recent analysis in Lancet by Bhangu et al. (9), scoring was proposed as a step in diagnostic flowchart of patients with suspected appendicitis. In this study, the new AAS score was superior compared to published validation results of Alvarado and Appendicitis Inflammatory Responce Score (AIR) score mentioned in the analysis by Bhangu. AIR score has excellent specificity but lacks sensitivity in high-risk group in validation studies. This means that only a minority of patients with appendicitis are stratified to high-risk group. Alvarado score has better sensitivity but lacks specificity. The sensitivity of AIR score was 23%–33% in previous studies compared to the sensitivity of the new AAS of 49% in this study. AAS classified half of all patients with appendicitis to high-risk group, whereas in the study by Scott et al. (4) AIR recognized 30 of 132 (23%), and in the study by Kollar et al. (7) 22 of 67 (33%). The negative predictive value (likelihood of no appendicitis in the low-risk group) was 93% in this study and in the studies of AIR score mentioned above, the value was 94%–95%. In the study by Kollar et al. (7), the Alvarado score stratified 53 of 67 (79%) patients with appendicitis to the high-risk group with specificity of 76%. The negative predictive value of Alvarado score was 93%. Hence, Alvarado score recognizes patients with low risk of appendicitis, but does not replace imaging in the high-risk group. Because of lack of specificity, Alvarado score is inferior to AIR score and, in the light of this study, the new AAS. This study did not include direct comparison with other scoring systems. However, in the original study of construction of AAS, we compared the diagnostic accuracy of AAS with AIR and Alvarado scores. In that study, AAS was superior to both AIR and Alvarado.
A diagnostic scoring system does not replace imaging but helps selecting the patients in need of imaging. This is important, on one hand, because of harms of false-positive diagnosis with negative explorations and, on the other hand, because of potential harms of imaging.
Risks of radiation are of special importance in young patients who represent the majority of patients with suspected appendicitis. There are estimations that on young adults suspected of acute appendicitis, 2000 CT scans would result in at least one cancer death (2, 10). In addition to increase in cancer risk, other potential harms include allergic reactions to contrast medium and contrast-induced nephropathy (11).
There are several ways to avoid excessive radiation. Low-dose abdominal CT has equal diagnostic accuracy compared to standard-dose CT in diagnosis of acute appendicitis with significantly lower radiation dose (12). In several studies, US has been implemented as a method to stratify patients according to risk of appendicitis (13–15). Unfortunately, US frequently fails to exclude appendicitis and accurately diagnose the most common differential diagnoses (16). Performing US on a patient with suspected AA inevitably takes time and requires experienced performer.
Definition of negative appendectomy varies. Thus, comparison of negative appendectomy rates between different studies can be inaccurate (17). However, the negative appendectomy rate in the study population was comparable to the negative appendectomy rate in studies from hospitals with mandatory preoperative imaging (3, 6). Thus, it seems that mandatory imaging could be restricted for patients with equivocal appendicitis according to clinical scoring. In this study, nearly two-thirds of all patients were either in the low-risk group or in the high-risk group, where mandatory imaging has limited benefits.
The instructions of imaging given by the scoring system were not fully followed during the study. Instead, the proportion of patients who underwent diagnostic imaging was greater, and some patients with low or intermediate score were operated on without imaging. This is probably partly due to surgeons’ hesitation in trusting a newly introduced diagnostic tool. However, no diagnostic method is infallible—a strong clinical suspicion of either appendicitis in the low-risk group or alternative diagnosis in all groups should always authorize imaging. There were 13 patients in the intermediate- and low-risk groups who underwent negative appendectomy due to clinical suspicion either without preoperative imaging or after negative or inconclusive imaging. If the instructions would have been followed in these cases, the negative appendectomy rate would have been 6.0%.
There were 152 (35.2%) patients with AA who underwent surgery without preoperative imaging. Interestingly, the highest negative appendectomy rate was in patients with initially low probability of appendicitis according to scoring with high rate of false- positive imaging study result. In order to reduce negative appendectomy rate even more, patients with low probability according to scoring should not undergo diagnostic imaging nor surgery in the first place.
This study had a potential limitation: the score was implemented in hospital B to achieve external validation. The amount of patients enrolled in hospital B was 88 (9.7%) of 908 patients. The low number of patients from hospital B limits the value of external validation, and more studies outside hospital A are needed for the external validation of the AAS.
In summary, the introduction of AAS helped to reduce negative appendectomy rate without mandatory imaging in patients suspected of acute appendicitis. AAS is an accurate, fast, and easily applicable method for stratifying patients according to risk of appendicitis. AAS is available as an online calculator on www.appendicitisscore.com.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was financially supported by the Mary and Georg C. Ehrnrooth’s foundation and the Martti I. Turunen’s foundation (personal research grant for the corresponding author).