
Abstract
Key Takeaways
• Evaluation of children with abdominal pain is a leading cause of transfer to a Children’s Hospital. • In this study, we created a clinical score (Avoiding Transfer in Pediatric Abdominal Pain Score (AT-PAPS) to predict which children do not need to be transferred to a higher level of care for an appendicitis evaluation. • A score of 5 or less was predictive of an unnecessary transfer with a sensitivity of 90% and negative predictive value of 90.9% potentially leading to cost and time savings for the family.
Introduction
Acute appendicitis is the most common reason to seek care from a pediatric surgeon1,2 and is associated with a high rate of inter-hospital transfers. 3 Many of these patients initially present to referring hospitals for abdominal pain and are subsequently transferred for an additional appendicitis workup at a dedicated children’s hospital. Current literature suggests that pediatric patients who are transferred for appendicitis do not have more advanced disease or increased rates of complication; however, these patients are exposed to more ionizing radiation during their appendicitis workup.4,5 Additionally, non-pediatric hospitals use CT at a higher rate to diagnose appendicitis in the pediatric population, but despite increased imaging, negative appendectomy rates are similar between transferred and non-transferred patients. 5 Furthermore, literature suggests that there is a high utilization of resources during an appendicitis workup in patients who are at a low risk of appendicitis, highlighting an opportunity to selectively improve resource stewardship. 6
Numerous scoring systems have been developed to accurately predict if a pediatric patient presenting with abdominal pain does have appendicitis, such as the Pediatric Appendicitis Score (PAS) 7 or the Pediatric Appendicitis Risk Calculator (pARC). 8 To rule in appendicitis, these scoring systems use a combination of demographics, vital signs, laboratory date, and symptomatology. These scoring systems each look at a combination of age, sex, temperature, anorexia, pyrexia, nausea and/or vomiting, pain characteristics, white blood cell count, and absolute neutrophil count. Additionally, the Pediatric Appendicitis Laboratory Score (PALabS) assesses similar factors to predict which children are a low risk for appendicitis. 8 However, to our knowledge, none of the pre-existing clinical scores were designed to predict who does not need to be transferred to a children’s hospital for an appendicitis evaluation. While it may be that a negative appendicitis score indicated that a patient does not need to be transferred, the available literature does not necessarily support that claim.7-9
At our institution, we found that the majority of our patients being transferred for an appendicitis workup (66%) did not have appendicitis. To address this gap, we created a clinical score, the Avoiding Transfer in Pediatric Abdominal Pain Score (AT-PAPS) to predict who does not need to be transferred to a higher level of care for an appendicitis evaluation. Incorporation of this score into clinical decision making is an opportunity to better utilize hospital resources and to decrease the cost burden for patients and their families.
Methods
Data Collection
A retrospective review was performed of all pediatric patients (ages 5–17 years) who were transferred into Greenville Memorial Hospital from January 1, 2017, to March 31, 2022. Study exemption was granted by the Prisma Health Institutional Review Board, Greenville, SC. Patient records were obtained from the electronic medical record transfer log report. Inclusion criteria included patients who had all three of the following characteristics: a chief complaint of abdominal pain or admission diagnosis of appendicitis (N = 1404), a workup for possible appendicitis (N = 1354), and complete data (N = 1314). 40 patients were missing lab data and were excluded. Data collected included demographics (age, sex, race, and ethnicity), clinical presentation (length of symptoms, initial presenting symptoms, and vitals), labs (CBC, BMP/CMP, ESR, and CRP), length of hospital stay, and diagnosis of appendicitis, as confirmed by intraoperative findings.
Score Development and Validation
To develop and test our proposed scoring system we divided the data into a “derivation” data set and a “validation” data set based on transfer date. The derivation data included patients from January. 1, 2017, to Mar. 31, 2021 (N = 1099). The validation data set included patients from April 1, 2021, to March 31, 2022 (N = 251). Bivariate analyses of possible predictors for the diagnosis of appendicitis were assessed using the Chi-square test for proportions and Student’s t test (or Wilcoxon Rank Sum) for continuously distributed data. Variables with >10% missing data were excluded from assessment for possible inclusion in the scoring system. Factors showing potential relationships with confirmed appendicitis (P-values <0.10 in bivariate analyses) were included in the full logistic exploratory model. Backward stepwise multiple logistic regression analysis was then used to assess for independent predictors of appendicitis. Adjusted odds ratios from the final model were used for the weighting of scores in the proposed scoring system. Cutoff scores were evaluated using sensitivity, specificity, positive predictive value, and negative predictive value. Receiver operator curve analysis (ROC) and area under the curve (AUC) were used to define and assess scoring system accuracy. P-values of <0.05 were considered indicative of statistical significance. SAS Enterprise Guide 8.3 software (SAS Institute, Cary, NC) was used for all statistical analyses.
Results
Study Population
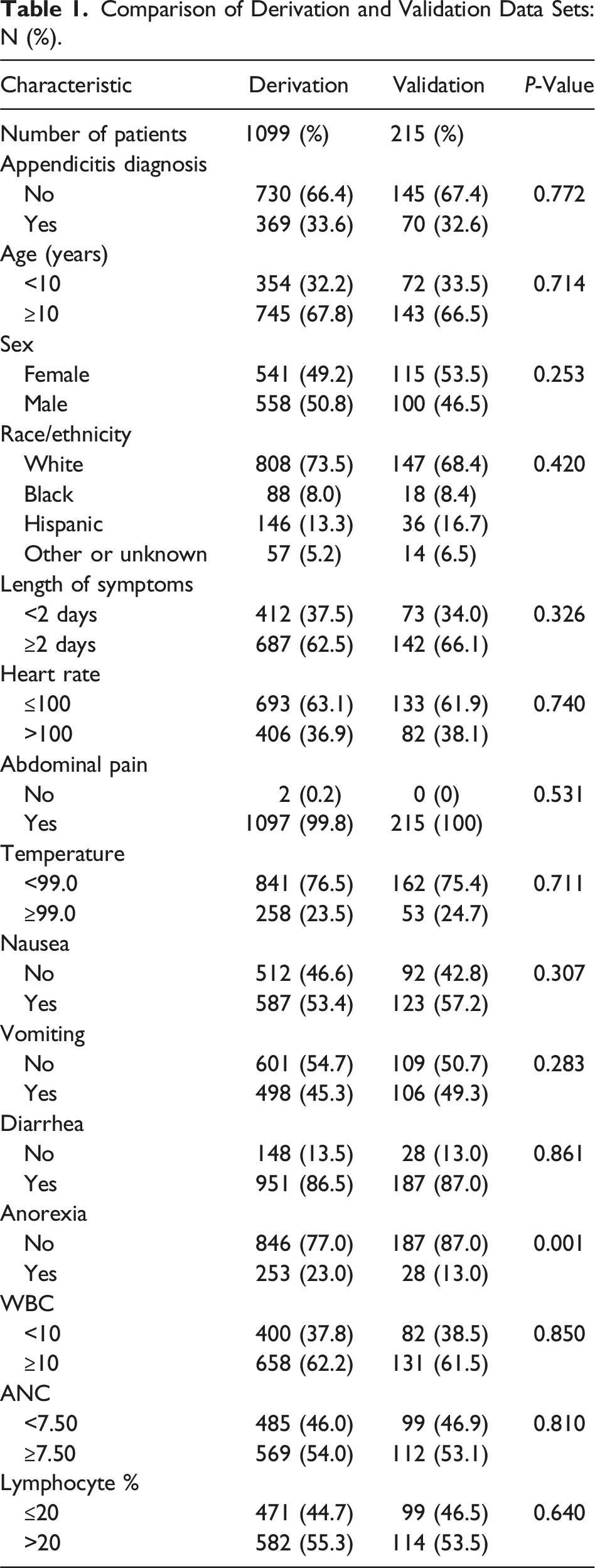
Comparison of Derivation and Validation Data Sets: N (%).
Score Development
Assessment of Continuously Distributed Variables by Diagnosis of Appendicitis [Derivation Set]: (Mean ± SD).
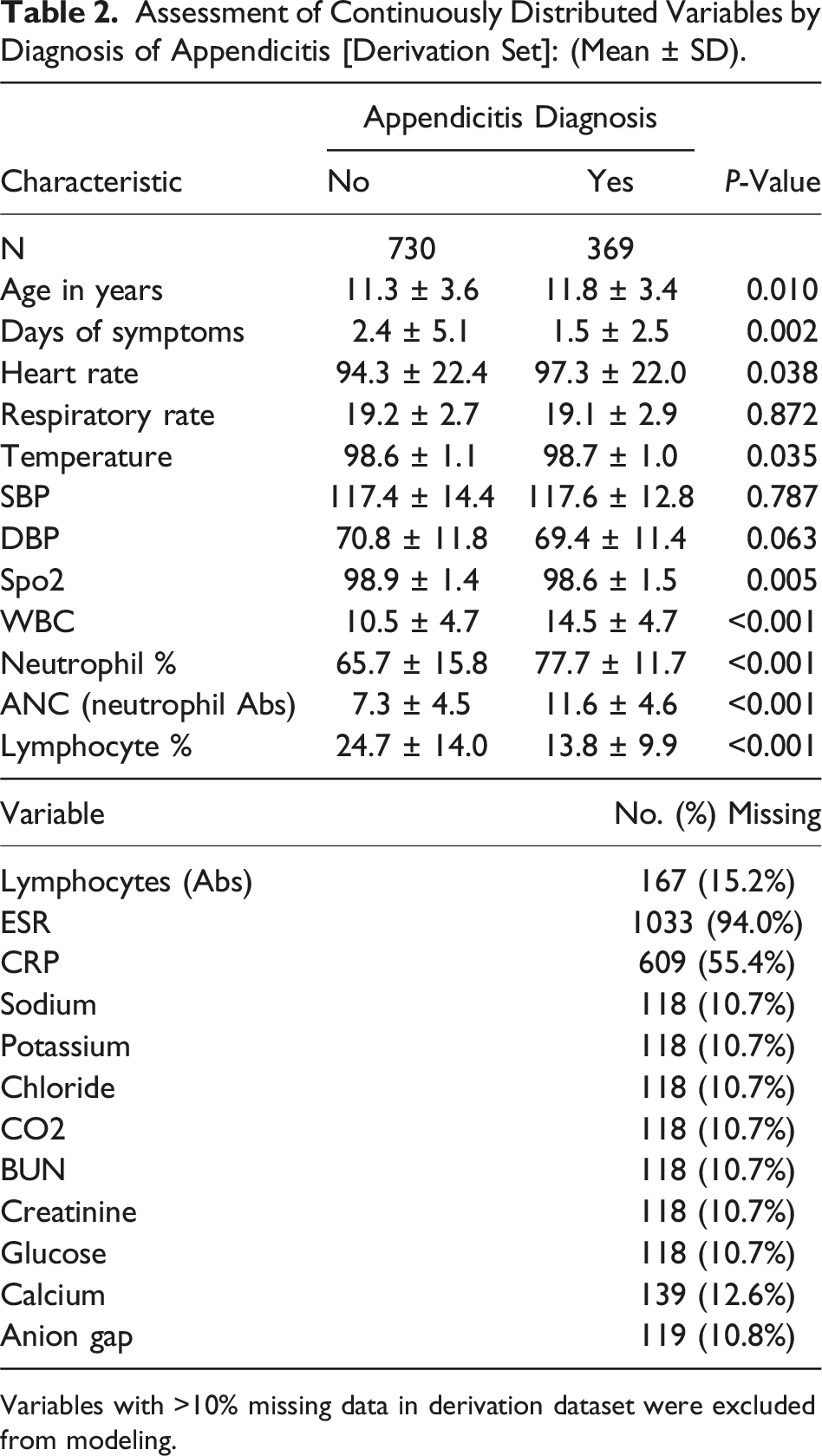
Variables with >10% missing data in derivation dataset were excluded from modeling.
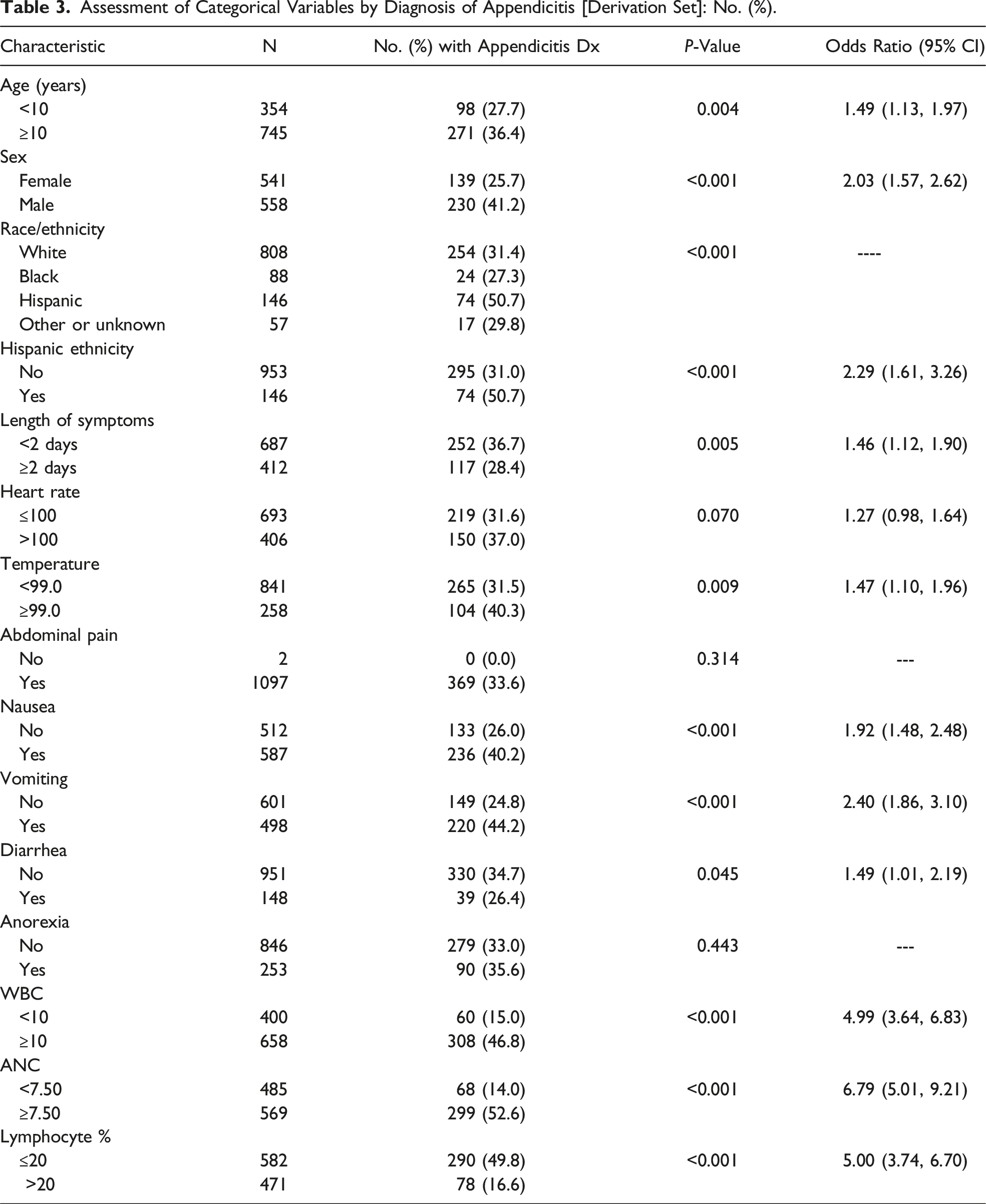
Assessment of Categorical Variables by Diagnosis of Appendicitis [Derivation Set]: No. (%).
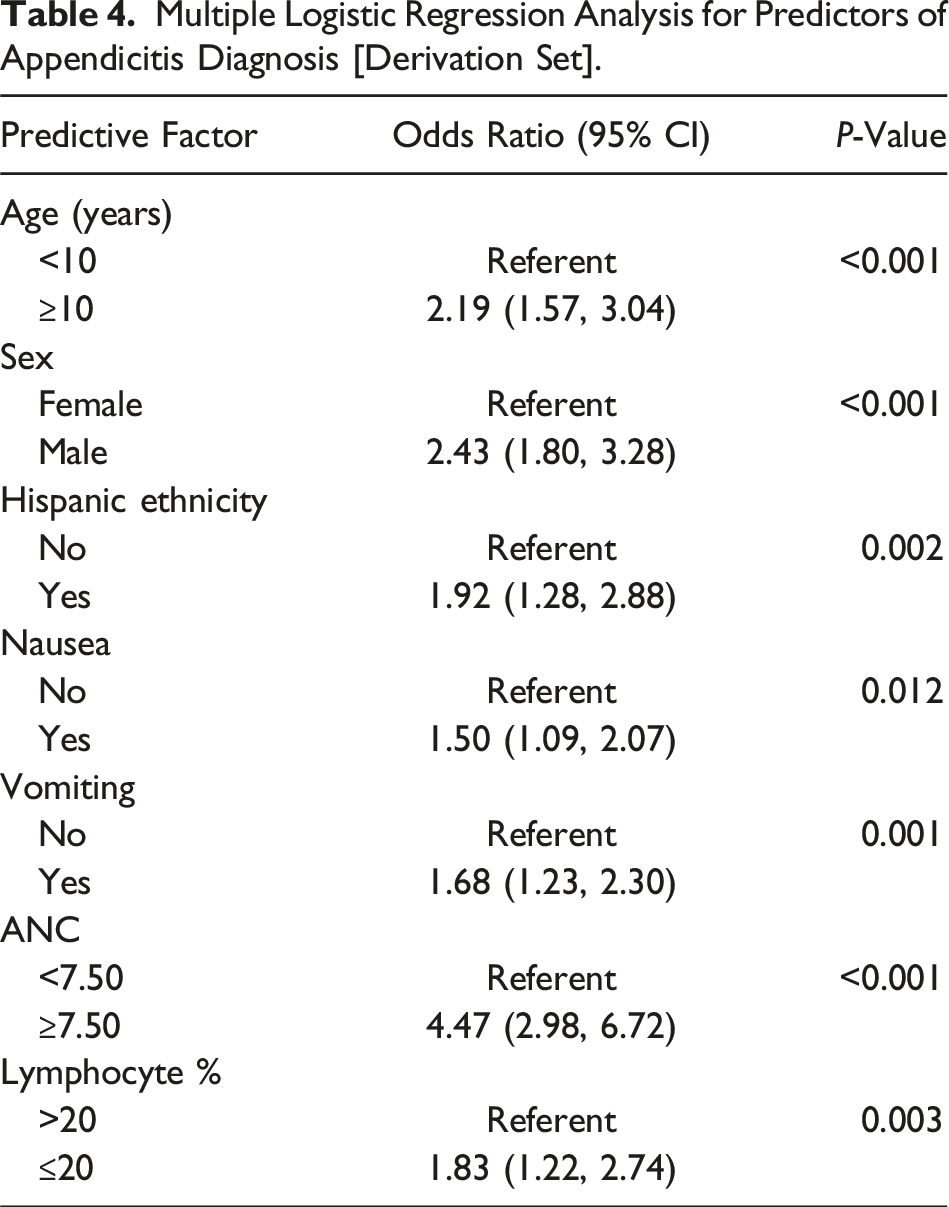
Multiple Logistic Regression Analysis for Predictors of Appendicitis Diagnosis [Derivation Set].
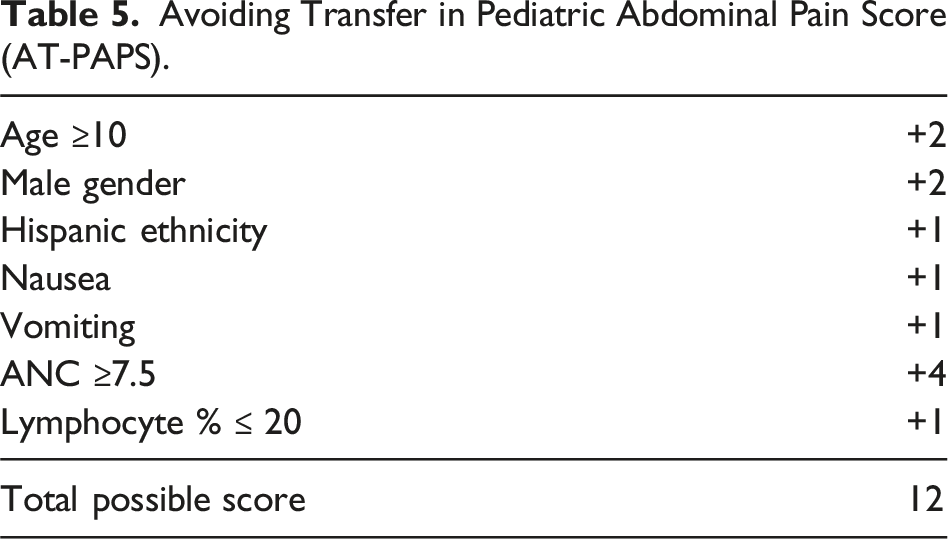
Avoiding Transfer in Pediatric Abdominal Pain Score (AT-PAPS).
Distribution of Total Score [Derivation Set].
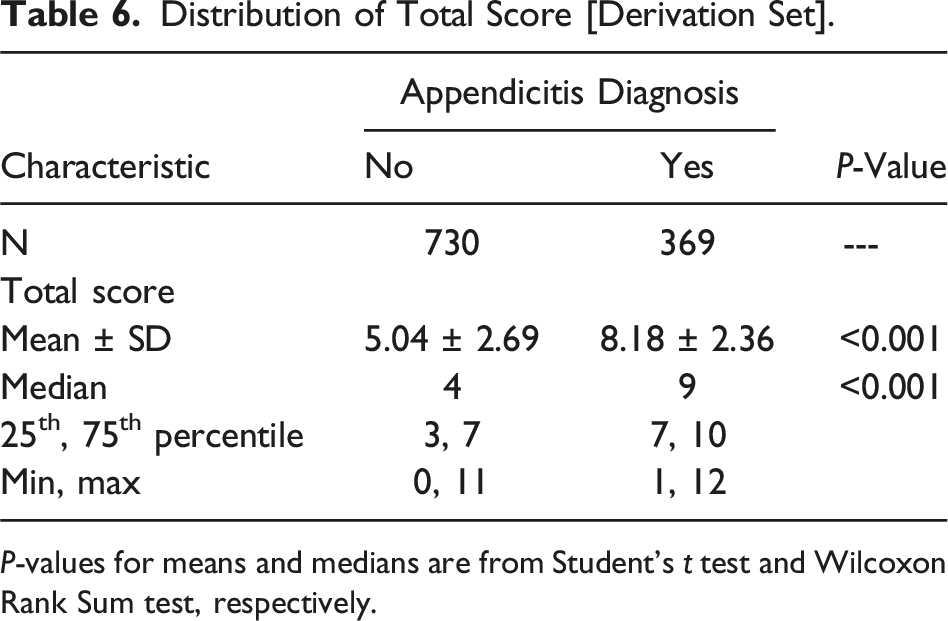
P-values for means and medians are from Student’s t test and Wilcoxon Rank Sum test, respectively.
Distribution of Total Score [Validation Set].
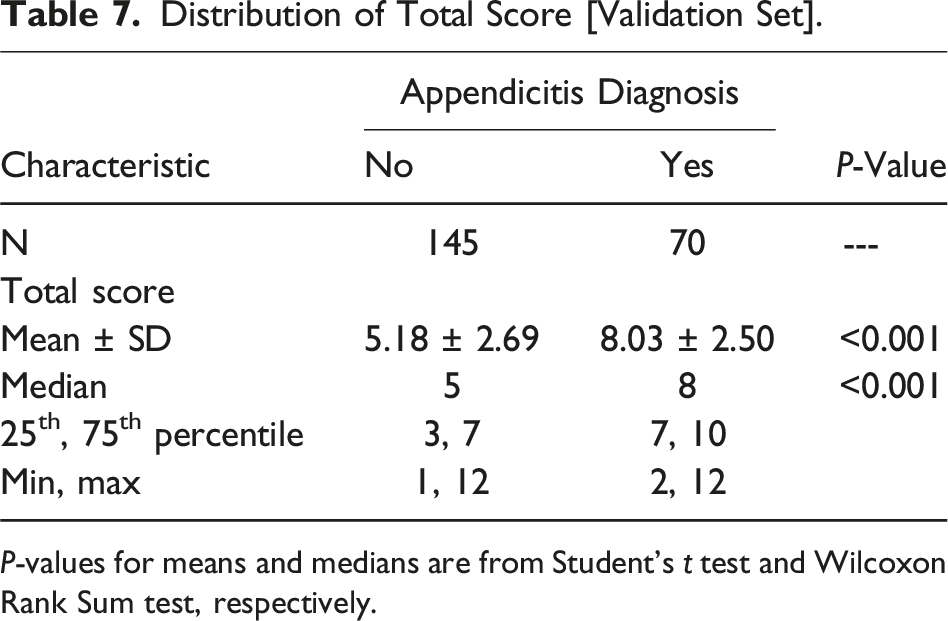
P-values for means and medians are from Student’s t test and Wilcoxon Rank Sum test, respectively.
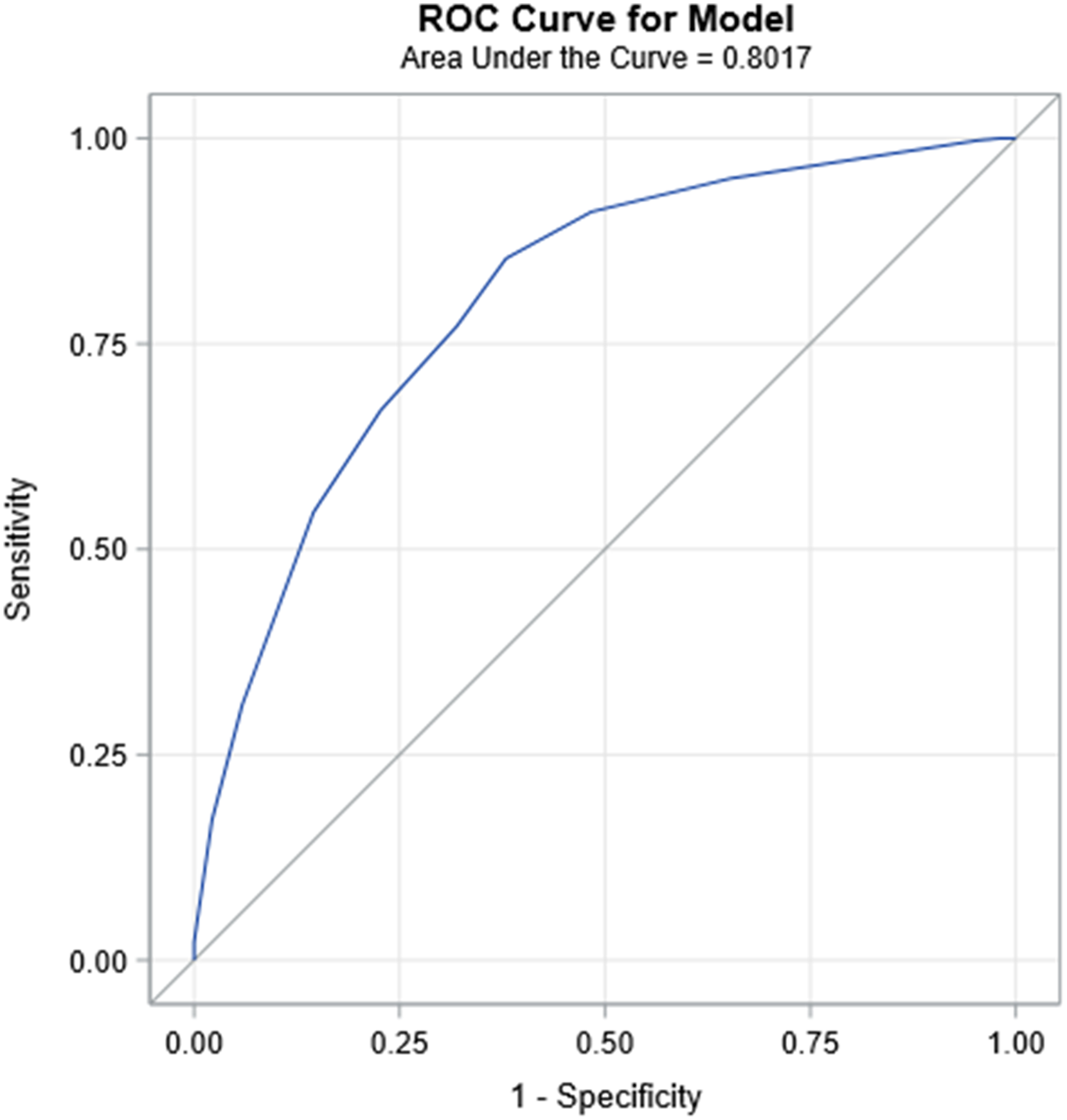
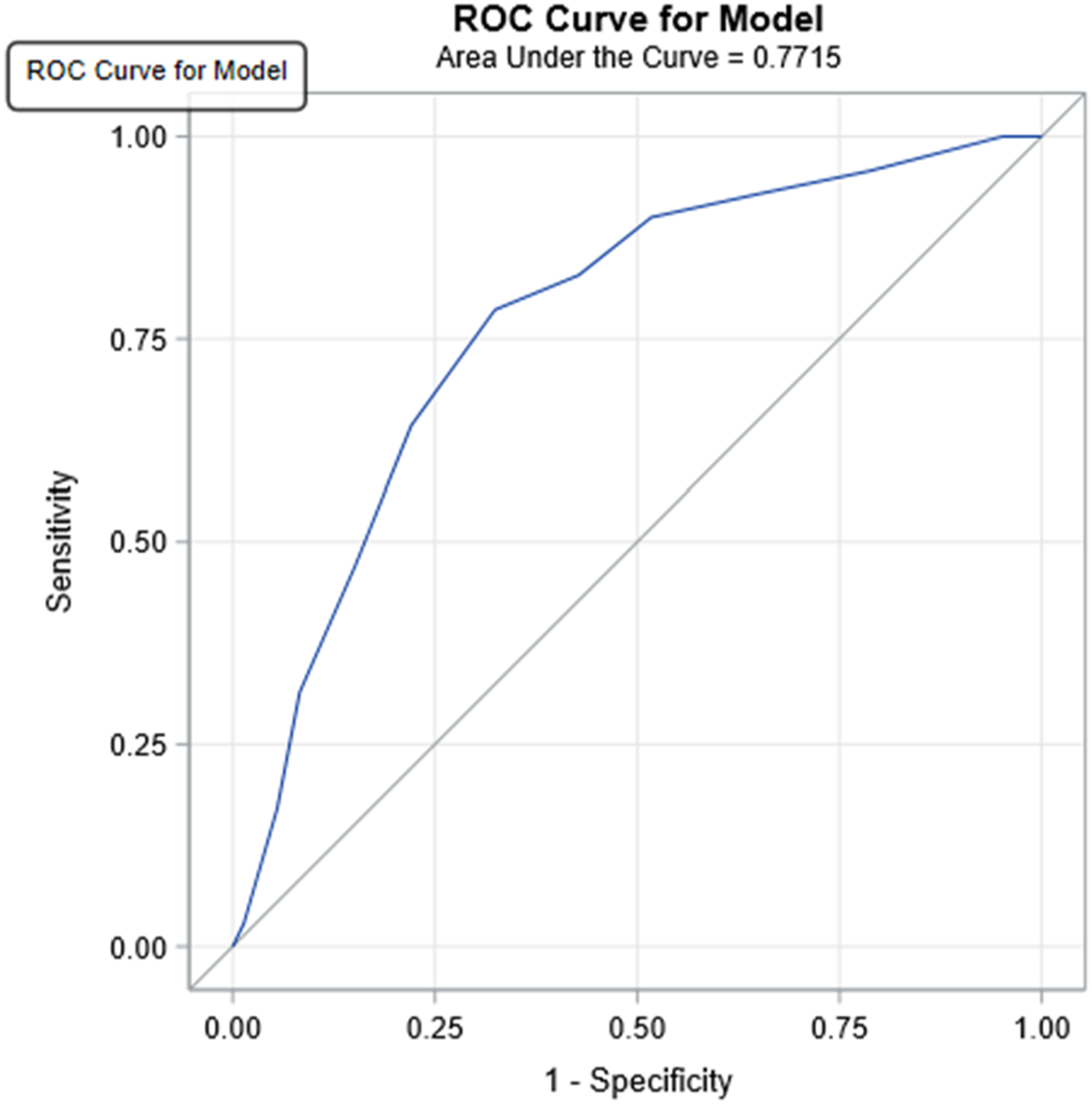
A score of ≤5 points predicted unnecessary transfer (P < 0.001), with a sensitivity of 90%, negative predictive value of 90.9% (Figure 1), and AUC values of 0.802 and 0.772 in the derivation and validation sets, respectively (Figures 2 and 3). AT-PAPS score sensitivity and negative predictive values. ROC curve for model [derivation set]. ROC curve for model [validation set].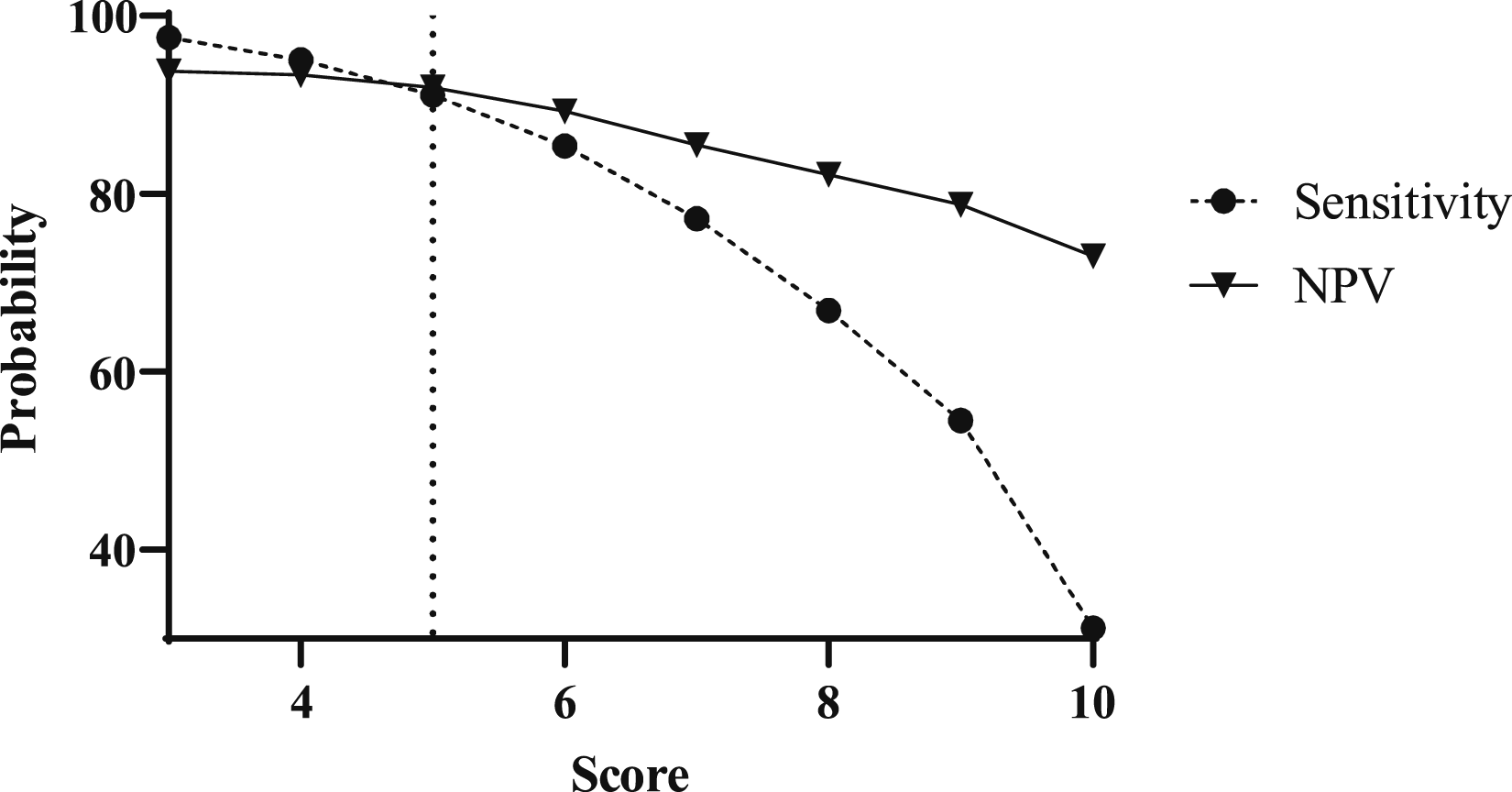
Discussion
As many interfacility transfers for pediatric appendicitis evaluation are unnecessary, we created a clinical score, the Avoiding Transfer in Pediatric Abdominal Pain Score (AT-PAPS), to predict which patients do not need to be transferred to a higher level of care for an appendicitis evaluation. This system utilized backward variable selection multiple logistic analysis to select seven easily obtained data points and demonstrated that a score of < 5 predicted excessive transfers with 90.9% sensitivity in a separate validation cohort.
França and McManus suggest that 30% of pediatric patients transferred for abdominal pain and appendicitis were discharged without undergoing any intervention, suggesting that there is an opportunity to decrease patient transfers. 3 Furthermore, O’Guinn et al found that 28.8% of patients transferred to their center with a diagnosis of appendicitis were unnecessary. 10 At our institution, we found that 66% of patients transferred for an appendicitis workup were not diagnosed with appendicitis, indicating that this is a prevalent topic throughout multiple health systems and with significant effects on patients, providers, and payers.
We found that variables significantly associated with appendicitis included: age ≥10 years, male gender, Hispanic ethnicity, nausea, vomiting, absolute neutrophil count ≥7.5, and lymphocyte percent ≤20 (Table 5). Our proposed scoring system has a total of 12 points, and an AT-PAPS of ≤5 points predicted no transfer requirement (P < 0.001). The cutoff of ≤5 points represents the maximum score that is able to maintain greater than 90% sensitivity, given our goal of determining which patients who do not require a transfer. The negative predictive value of a score of ≤5 points is 90.9% (Figure 1). Worth noting, the average AT-PAPS score in our negative appendicitis group was greater than the cut off of 5 points; however, given that our aim is to reduce avoidable transfers without creating barriers to subspecialty care, we chose a lower value to minimize false negatives and allow for clinical decision making.
Compared to existing scores which aim to diagnose appendicitis, our score is unique in that this model is designed to reduce unnecessary transfers for an appendicitis workup. As such the data are derived from a cohort of patients who were transferred for an appendicitis evaluation, where there was a higher pre-existing clinical suspicion for appendicitis in these patients. This enriched population is more pertinent to creating a model focused on transfer necessity. Likewise, in contrast with diagnostic models which aim for high specificity, this system focused on negative predictive value and sensitivity. Despite these differences in purpose and cohort, the criteria used to develop AT-PAPS are similar to those in numerous scoring systems exist to rule in appendicitis, including the PAS and pARC scores.7,8 These scoring systems each look at a combination of age, sex, temperature, anorexia, pyrexia, nausea and/or vomiting, pain characteristics, white blood cell count, and absolute neutrophil count, focusing on achieving a high specificity.7,8 Alternatively, the Pediatric Appendicitis Laboratory Score (PALabS), which assesses white blood cell count, neutrophil count, C-reactive protein, calprotectin, and clinical signs was designed to predict which children are a low risk for appendicitis. 9 In designing our model, we were intentional in the data that we incorporated to make the score accessible for a variety of clinical settings with differing resources. We excluded any imaging findings in our clinical score, assuming that some settings may not have readily accessible ultrasound or CT, which would lead to their interfacility transfer in the workup of appendicitis. Furthermore, right lower quadrant (RLQ) pain was excluded from our score given that it was within the study inclusion criteria. Given the intention for AT-PAPS to be used to distinguish which patients being evaluated for appendicitis require a transfer, we expect that the majority will have RLQ pain in their presentation, making it a less sensitive marker for predicting transfer requirement.
Prior investigation has supported the findings from which our score is derived. Factors associated with avoidable transfer include a lack of common symptoms such as fever, migratory abdominal pain, anorexia, nausea, shorter duration of symptoms, younger patients, lower WBC, and lower inflammatory markers, in line with our results. 10
The need to predict which patients can avoid transfer is well supported in the literature, as inter-hospital transfers result in a higher cost burden for patients due to additional expenses for ambulance transport, lodging, family travel, increased probability of hospital admission, and often, redundant diagnostic testing.3,5,10-13 O’Guinn et al found that 42.9% of avoidable transfers for appendicitis workup undergo repeat imaging, submitting these patients to additional ionizing radiation and financial morbidity. 10 In studying the cost burden to rural families for avoidable transfers to a children’s hospital, Mohr et al found that there was a median additional cost of $909 for transferred patients and their families. 13 Reducing potentially avoidable transfers is an opportunity to reduce resource utilization and repetitive diagnostic testing, which are both expensive and emotionally stressful for patients. By creating a clinical score to predict which patients do not require a transfer to a higher level of care for an appendicitis evaluation, AT-PAPS is intended to be used as a tool to incorporate into clinical decision making to reduce avoidable transfers.
This study is not without limitations. Our model was created from a single-institution patient cohort, thus limiting external validity. Patient populations and transfer protocols vary widely between institutions, and it would be beneficial to incorporate data from additional institutions into our model. Additionally, while we intentionally excluded imaging results from our model for ease of clinical implementation, its inclusion could enhance the sensitivity and NPV of our model. Future prospective studies to validate the model in additional institutions and to assess the impact on clinical decision making will provide valuable insight into its application and benefit for reducing unnecessary transfers for pediatric appendicitis evaluations.
In conclusion, we found that the majority of patients transferred to our institution for an appendicitis evaluation ultimately were not diagnosed with appendicitis, which highlights the need for a clinical tool to improve transfer decisions. AT-PAPS is a clinical score designed to predict which patients do not require transfer to a higher level of care for an appendicitis evaluation. We intend for AT-PAPS to be used as screening tool to aid clinicians in transfer decisions, reducing avoidable transfers, financial burden on families, and unnecessary resource use.
Footnotes
Acknowledgments
We thank the University of South Carolina School of Medicine Greenville Academic Medicine Research Elective for their support of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Full data available from authors upon request.