
Abstract
Background and Aims:
Many kinds of insoles and pads are commonly used as a conservative treatment of metatarsalgia. However, earlier studies of insole treatment provide contradictory results, and the natural progression of metatarsalgia is still unknown. The aims of this study were to (1) determine whether simple custom-made metatarsal pad insoles reduce pain and improve functional ability, (2) find out patients’ satisfaction with padding treatment, and (3) investigate predisposing factors for metatarsalgia.
Material and Methods:
All metatarsalgia patients provided with metatarsal pad insoles during a 2-year period at Kuopio University Hospital (n = 45) were included in the study and observed at least a year. In all, 25 patients were interviewed about their situation before and after treatment. The Numeric Rating Scale for pain and American Orthopaedic Foot & Ankle Society forefoot questionnaire included questions about predisposing factors, other diseases, exercise, work, shoes, and satisfaction with insoles. Foot X-rays taken from 45 patients during treatment were analyzed.
Results:
The mean age of the patients was 56 years (range 34–84 years); 87% of them were women. In all, 47% of patients had osteoarthritic changes in the first metatarsophalangeal joint, and 42% had hallux valgus. In the interviewed subgroup (n = 25) body mass index was normal in 44%, and 36% were mildly overweight. High-heeled shoes were used by 40% daily, and 68% had done standing work for several years. Pain decreased significantly on the Numeric Rating Scale: 3.2 points in all patients (p < 0.001), 3.1 points among women, and 4.25 points among men. The American Orthopaedic Foot & Ankle Society score improved 24.2 points in all patients (p < 0.001, range 0–100), among women 19 points, and among men 29 points.
Conclusion:
Metatarsalgia affects mostly women and is often preceded by extensive use of high heels and standing work. Also, a high association of first metatarsophalangeal arthrosis and hallux valgus was found. Metatarsal pads reduce pain and improve the American Orthopaedic Foot & Ankle Society score. We recommend metatarsal padding as a safe and inexpensive alternative in treating metatarsalgia patients.
Introduction
Pain under the distal heads of the metatarsal bones, usually in the second and third rays, is called metatarsalgia (Fig. 1). Most of the pressure during the toe-off phase of the gait concentrates on this area (1, 2). Metatarsalgia is a quite common condition; it can restrict movement or even totally prevent walking. Metatarsalgia is often related to common foot malpositions such as hallux valgus, hammer toe and flat foot, or hypermobility of the first ray (2–4). In spite of associations with malpositionings, there are only a few x-ray measurements in the literature about anatomic characteristics of bony structures among metatarsalgia patients. Predisposing factors for metatarsalgia might also be rheumatoid arthritis and diabetes (2). In addition to increased pressure load, there can also be inflammation, neuropathy, or malpositioning of the fat pad under the forefoot (2). The natural progression of metatarsalgia is still unknown.
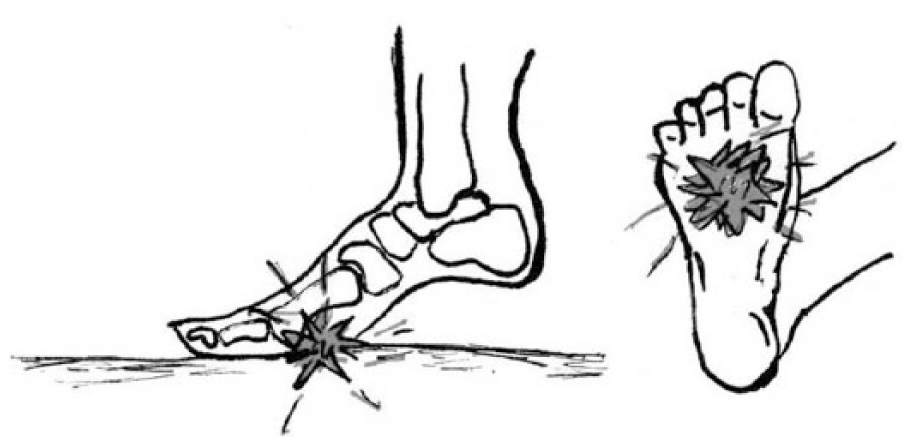
Metatarsalgia is usually located under the distal parts of the second and third metatarsal bones.
Different kinds of insoles and metatarsal pads or toe orthoses are commonly used as a conservative treatment of metatarsalgia (1, 2, 5). Kang et al. (2) found out that metatarsal pads (Fig. 2) can diminish plantar pressure under painful metatarsal heads by spreading it to a larger area and by elevating the possibly fallen horizontal arch of the forefoot (2). It also seems that this arch elevation creates more space between metatarsal heads; this feature could play a role in pain reduction especially in Morton’s neuralgy, where increased load on the forefoot causes interdigital nerve compression and irritation (6). Morton’s neuralgia is quite common and is usually treated conservatively with metatarsal pads, corticoid injections, and physiotherapy. Interdigital neurinectomy could help in incalcitrant cases.
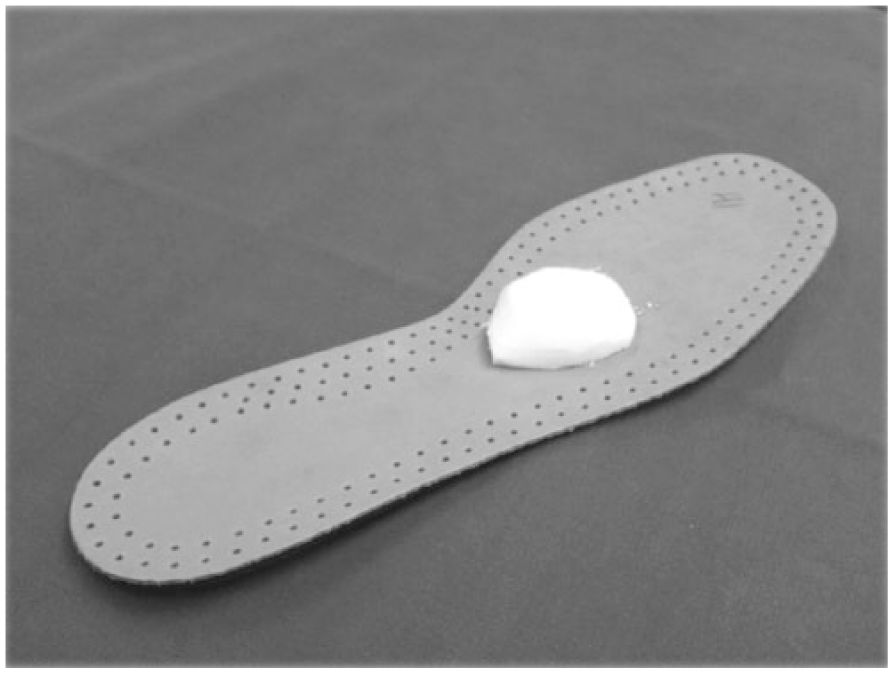
The insole with metatarsal pad.
The placement, size, and material of metatarsal pads are important (1, 2). Changes in pressure distribution caused by the pad correlate with pain reduction (2, 7, 8). However, the effects of conservative treatments vary considerably, including the use of insoles and pads.
The aims of this study were to (1) determine whether simple custom-made metatarsal pad insoles reduce pain under the forefoot and improve functional ability, (2) find out patients’ satisfaction with padding treatment, and (3) investigate predisposing factors for metatarsalgia using a questionnaire and X-ray analysis for foot morphology and deformities.
Our working hypotheses were as follows:
Metatarsal pad insoles relieve metatarsal overload pain (at least two points on the Numeric Rating Scale (NRS))
Hallux valgus, high-heeled shoes, and standing work predispose for metatarsalgia.
Materials and Methods
Participants and Selection
All patients diagnosed with metatarsalgia and provided with metatarsal pad insoles during a 2-year period at Kuopio University Hospital were included in the study. The exclusion criteria were age under 18, incompetency, serious mental disorder, or failure to see a physician during treatment. Of 59, 14 were thus excluded. An invitation letter for a telephone interview was sent to the remaining 45, and 25 participated. X-rays and diagnoses from case histories were analyzed for all 45 patients. The subjects gave informed consent, and the study protocol was approved by the Ethics Committee of Kuopio University Hospital.
Treatment
All patients selected were first evaluated by an orthopedic surgeon and then provided with metatarsal pad insoles by a cast technician in Kuopio University Hospital. The insoles were made by the cast technician by gluing a pad to a simple flat leather insole. The pads were made of 14-mm high foam rubber (Camp Scandinavia, Sweden), which was suitably cut (Fig. 2). The purpose of metatarsal padding is to elevate the horizontal arch of the forefoot. Patients visited the hospital every 2 weeks to have the pads and insoles changed because they wear out, and the right position may have to be reassessed. During these visits, patients were asked about pain relief; if the pads helped, custom-made foot orthoses including metatarsal pads were provided.
The Interview
Patients were interviewed by telephone, and during the interview, their symptoms before the insole treatment and at the time of the interview were asked. To evaluate pain and ability to function, the interviewer used the NRS and American Orthopaedic Foot & Ankle Society (AOFAS) forefoot questionnaires (9). A decrease in two points or 33% on the NRS is clinically relevant (10). The interviewer also sought information about predisposing factors, other diseases, medications, exercise, former treatment, and satisfaction with metatarsal pad insoles. Patient’s professions were divided into seven categories (11) based on the physical heaviness involved.
X-Ray Observations
During treatment, foot X-rays were taken from most patients as a part of normal treatment practice. These X-rays were analyzed to measure the length of the first and second metatarsal bones, intermetatarsal angle (IMA), hallux valgus angle (HVA), and Meary’s angle. An experienced orthopedic surgeon analyzed these X-rays. Signs of increased stress on the second metatarsal were noted, and the level of arthrosis in the first to third metatarsophalangeal (MTP) joints was evaluated using the Kellgren-Lawrence scale (8).
Statistical Analysis
All statistical analyses were performed using SPSS 17.0 for Windows, IBM Corporation. The paired samples t-test was used to compare changes in NRS and AOFAS scores. The X-rays were measured using Sectra Workstation IDS7, version 15.1.8.5., Linköping, Sweden.
Results
Subject characteristics
There were 45 patients, 25 of whom consented for an interview. Most of the patients were women: 86.7% of all and 84% of the interviewed subgroup. The average age of all our patients was 56 years (range 34–84 years); it was 59 years (40–74 years) in the interviewed subgroup. In the interviewed subgroup, 44% were normal weight, and 36% were mildly overweight (body mass index (BMI) 25–30).
Other Diseases
Patients in the interviewed subgroup were requested for information about other health problems, and the case histories of all the patients were checked. The most common diseases were degenerative diseases, for example, sciatica, prolapsus disci, spinal stenosis (56%), and osteoarthrosis of major joints (44%). The prevalence of hypertension was 27%, that of hypothyreosis was 27%, and that of rheumatoid arthritis was 16%. Only 7% had osteoporosis, 11% had diabetes, and 4% had polyneuropathy. However, 24% had various shoulder problems, and 16% had various ligament and meniscus ruptures; 7% patients had scleroderma.
Work, Exercise, and Shoes
Of the interviewed subgroup, 52% were not working at the time of the interview. Most of them were retired because of age. Most (68% of all, 53% of females, 100% of males) had done standing work for 3–40 years during their working career; the average was 23. Aromaa and Koskinen (11) used a work heaviness classification divided into seven categories: 0 = never worked (0%), 1–2 = light or sitting work (24%), 3–4 = light standing and standing work (40%), and 5–6 = hard manual and really heavy work (36%). Most men were placed in categories 5 and 6 (75%).
All the patients interviewed exercised in varying degrees. There were no competing athletes, but 64% exercised regularly, 24% sometimes, and 12% rarely. In all, 40% of our patients used or had used high-heeled shoes (heel over 2 cm) daily for many years. Those who could no longer wear them had to stop because of pain in the ball of the foot.
Previous Treatment
In all, 64% of the patients had used some kind of insole or other device in the shoes before attending our study: insoles with heel paddings, medial arch supports, and even metatarsal pads. Most of those were commercial and non-customized products. Some patients were unable to describe the insoles they had used. Of the patients, 16% had had physical therapy for metatarsalgia; 60% had had lower extremity or back operations before this study. Of those operations, 60% (36% of the patients interviewed) were in the forefoot area.
The Effects of Treatment
Metatarsal pad insole use
In all, 72% of the patients interviewed used their insoles all day long; 16% used them sometimes, and 8% had not used them at all. The average duration of insole use was 11.2 months (range 1 month to 3 years). Insole treatment was considered beneficial by 68% of our patients. Finally, 56% of the patients got individually made custom orthoses.
Only 52% would start the insole treatment again if they got metatarsalgia a second time, 20% were unsure, and 28% would not. Those who refused to start again either had had an operation and been healed or wanted to have more effective insoles or deemed insole use too laborious.
After treatment for at least 1 year, 48% were still using insoles because those devices relieved pain. Patients who had discontinued had obtained permanent help and had no need for insoles anymore (4%), had had an operation (20%), or had had some help but not enough (8%) or no help at all (20%).
The reasons for quitting insole use were that the insoles caused pain (16%), insoles did not help (16%), a shoe did not fit anymore (8%), or the patient had had an operation (20%). Of our patients, 24% had had an operation, and one of them is still using insoles. The majority (83%) of the operated patients were diagnosed for Morton’s neuralgy, and neurinectomy was performed. One Weil osteotomy was conducted to decrease metatarsal pressure.
During insole treatment, among patients who had some pain, 76% of the whole group perceived no location change in lower limb pain and 84% in lower back pain.
Simultaneous conservative treatments
During insole treatment, most patients interviewed were advised to do forefoot muscle exercises and calf stretching. In all, 64% of them had done the former and 52% the latter. A few (12%) had also had physiotherapy.
Change in pain and function
Pain on the NRS was reduced in 84% of the patients, stayed the same in 8%, and increased in 8%. A clinically relevant reduction of at least two points on the NRS was evident in 72% of the patients. The pain decreased significantly: 3.2 points in all patients (average 2.8, p < 0.001), 3.1 points among women (n = 21), and 4.25 points among men (n = 4).
The AOFAS score increased in 88% of patients, stayed unchanged in 8%, and decreased in 4%. In all our patients, the total increase was 24.2 points (scale 0–100, p < 0.001): among women 19 points and among men 29 points (Table 1).
Pain in NRS and AOFAS midfoot scale before and after insole treatment, n = 25.
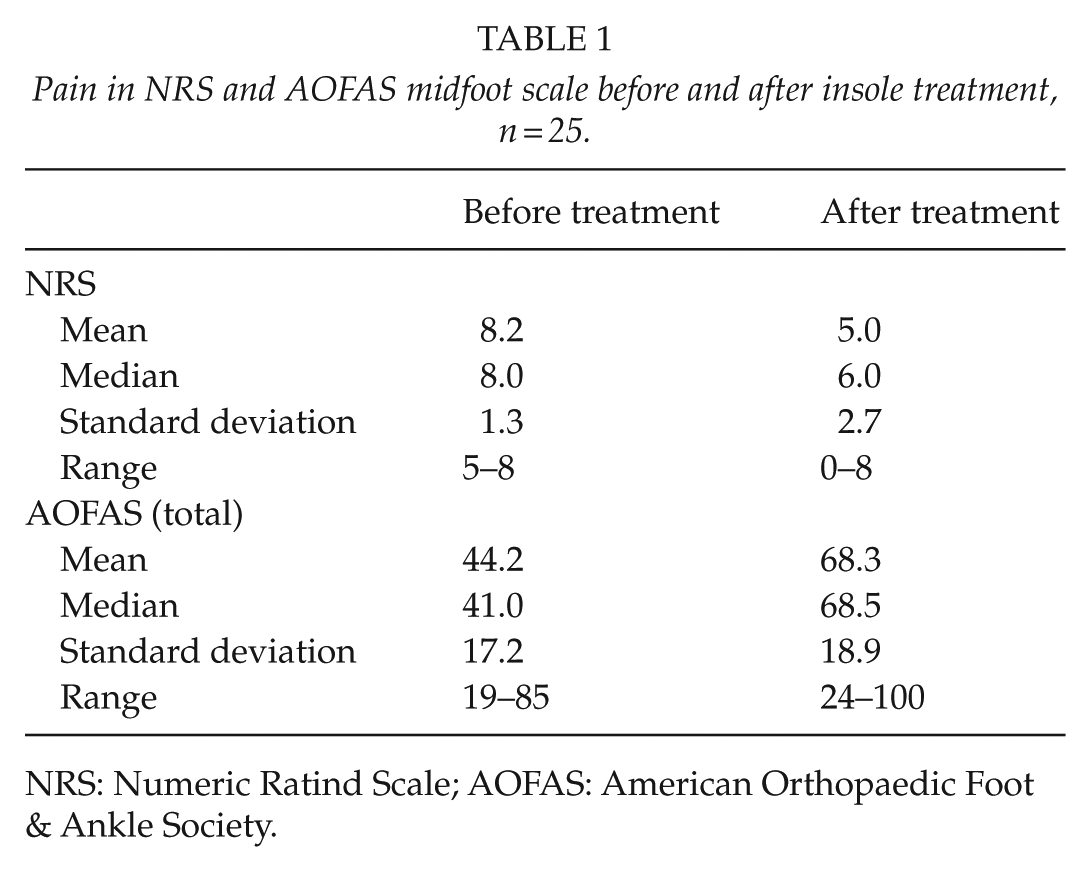
NRS: Numeric Ratind Scale; AOFAS: American Orthopaedic Foot & Ankle Society.
In the AOFAS questionnaire, patients reported 12.9 points of improvement in pain (scale 0–40, p < 0.001), and 10.0 points of increase in function (0–45, p < 0.001). Metatarsal padding had no effect on patient-evaluated foot alignment scores. Activity limitations improved by 1.9 (0–10, p = 0.003), gait abnormalities by 2.4 (0–10, p = 0.001), and maximum walking distance by 3.5 (0–10, p = 0.001). There was no significant change in footwear requirement or walking surfaces (Table 2).
AOFAS Midfoot Scale comparison after and before insole treatment, n = 25.
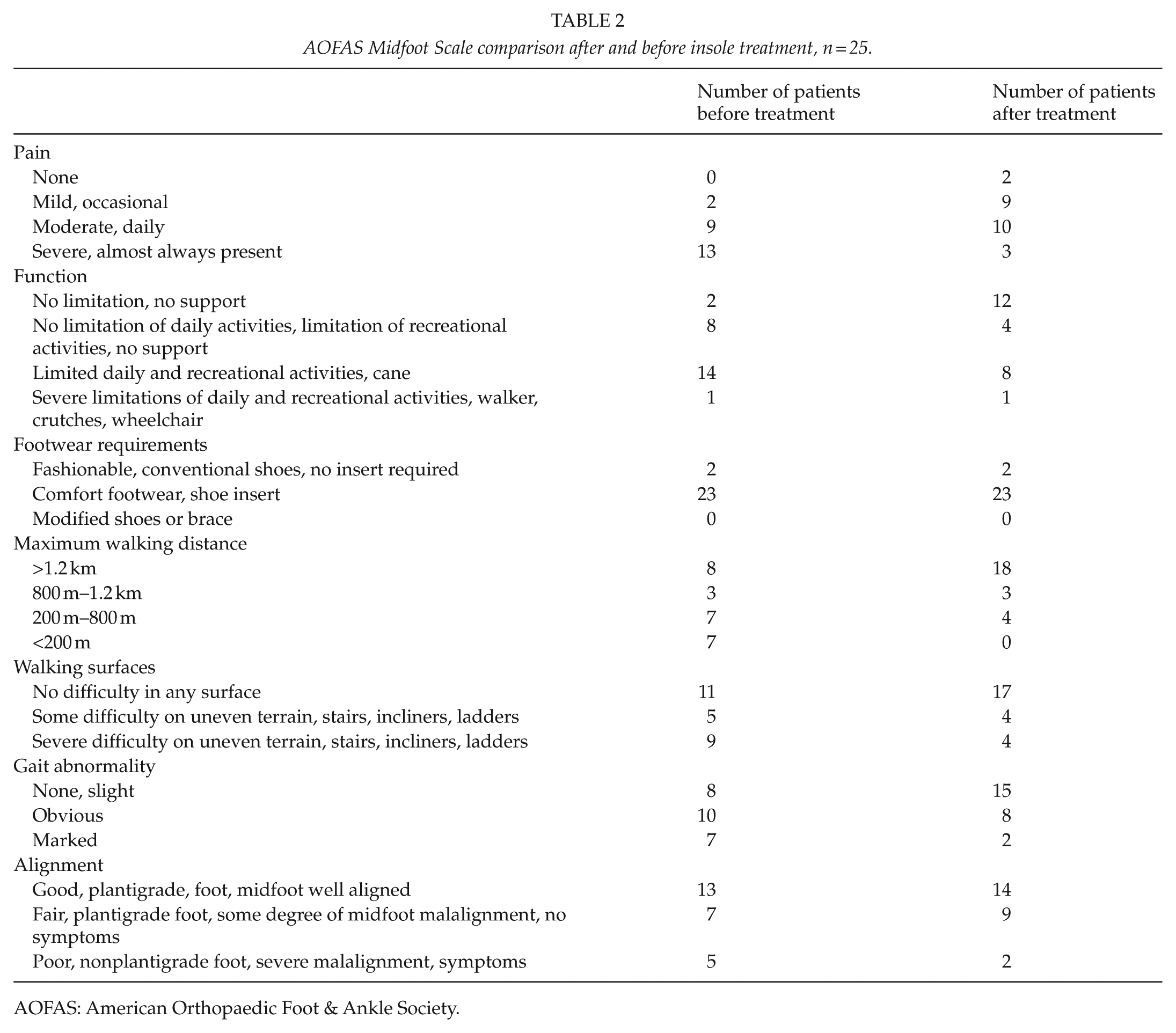
AOFAS: American Orthopaedic Foot & Ankle Society.
X-ray findings
Seven out of 45 patients had thickening of the second metatarsal. One patient’s foot had a markedly short first metatarsal (Morton’s foot) (12). The mean MT1 length was 60.6 mm, and the MT1/MT2 ratio 0.89. The HVA was measured in 31 patients. When categorized according to the level of HVA (foot with wider angle chosen), 58% of the patients had normal HVA (<15°), 10% had mild (15–20°), 29% moderate (21–40°), and 3% severe (>40°) hallux valgus. The mean IMA was 11.1, and the mean Meary’s angle was −3.2° (Table 3). The most arthrotic MTP joints were the first, then the second, followed by the third. Overall, 69.5% had arthritic changes in their first to third MTP joints.
Bone lengths and angles.
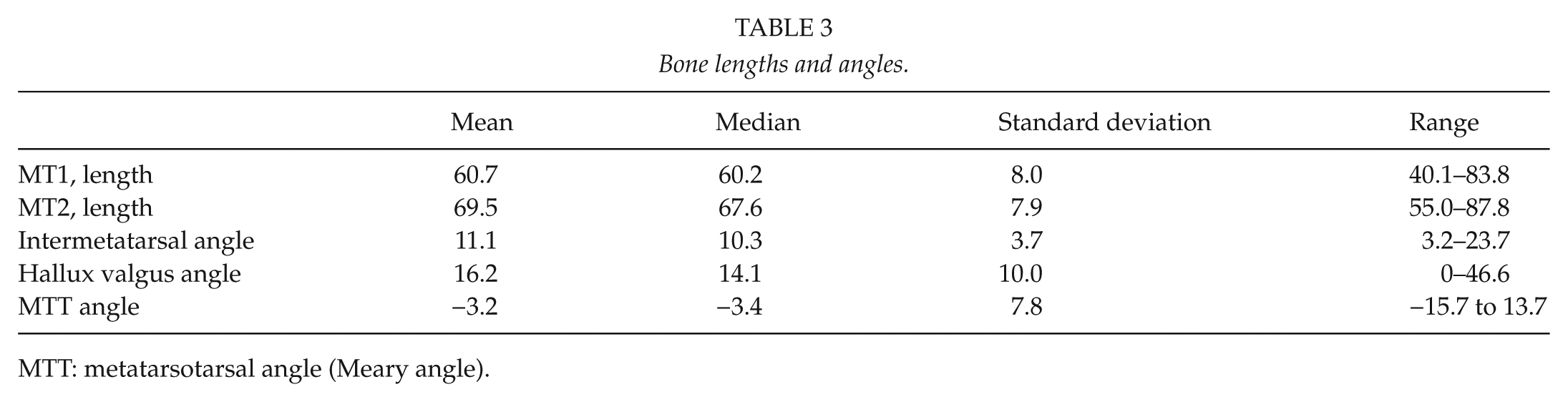
MTT: metatarsotarsal angle (Meary angle).
Discussion
Specially made insoles and insoles with metatarsal pads are commonly used as in the treatment of metatarsalgia. However, reports of this conservative treatment are conflicting (1, 2, 7, 13). The position, size, and material of the pad may be important factors for the success of the treatment (1, 2). There is no standardized manner to determine the best position, size, and material of the pad, so the placing is still based on an approximation by the insole maker. This could be one reason for the varying results reported in studies.
Metatarsalgia affects men infrequently; only 13% percent of our patients were men. Similar proportions have been found in previous studies (2, 14). The use of high-heeled shoes was quite common in our patients—40% had used heels higher than 2 cm most of their lives. Also, doing work standing was common—our patients had been working mainly on their feet 23 years on average. All men in our study had done standing work, which might be the main cause for metatarsalgia in the male population. Their work was also categorized heavier than that of women. The difference in the level of arthrosis in the MTP joints would be an interesting issue too, but our study lacked enough foot X-rays of male patients to enable a discussion. Age and weight had no significant role in the development of metatarsalgia.
In agreement with our working hypothesis, most patients treated with metatarsal pad insoles obtained pain relief. We found a decrease in two or more points on the NRS in 72% and an improvement on the AOFAS pain score in 71% (average 12.9 points, p < 0.001). The AOFAS score for function improved 10 points (p < 0.001), and the overall AOFAS score improved 24.2 points (p < 0.001). Patient satisfaction for the insole treatment was found to be quite good as 48% of the patients were still using insoles at the time of the interview, 4% have had permanent help (no need for insoles anymore), and 68% reported that insole treatment was beneficial. But only 52% would start the metatarsal pad insole treatment again. The compliance for this treatment was surprisingly low despite good results in pain relief. The patients felt insole treatment laborious, and perhaps it restricted choosing fashionable shoes too.
In all, 42% of patients whose X-rays were analyzed had hallux valgus. This result supports earlier findings that hallux valgus is related to first ray instability and metatarsalgia (2–4).
The MT1-MT2 ratio was 0.89 on average; the range was 0.71–1.04 and the standard deviation 0.09. Davitt et al. (15) reported an MT1-MT2 ratio of 0.77 in patients with midfoot arthrosis and 0.82 in the control group. Our patients did not have short first metatarsals as compared to the second metatarsals. The increased pressure under the painful second and third metatarsal heads in metatarsalgia patients is caused by increased mobility of the first ray.
Gong et al. (16) found a positive correlation between metatarsal pain and IMA in patients with hallux valgus. In our study, 42% had hallux valgus and 52% IMA over 10°.
The incidence of first metatarsophalangeal (MTP1) joint arthrosis (Kellgren-Lawrence categories 1–4 (8)) was high in our patients (97.4%). This might be due to increased mechanical stress in the MTP joint line caused by instability and elevation of the first ray, which has been found to be common in metatarsalgia patients (3, 4, 17, 18).
There are certain limitations in this study. First, the study is retrospective, so the patients might not have precisely remembered their pre-treatment symptoms. Not all patients had X-rays, and in some X-rays, the patients might not have been standing as the radiological documentation was sometimes vague. More than half of the patients interviewed had also had other conservative treatments: forefoot muscle exercises and calf stretching.
Further research is needed to determine the optimal positioning of the metatarsal pad and how the pad affects the biomechanics of the foot, leg, and lower back. Another point of interest is why so many of these metatarsalgia patients had hypothyreosis (26.7% vs 3.3% in the Finnish population) and scleroderma (7%), which is a very rare disease. No correlation between metatarsalgia and hypothyreosis has been reported earlier. Hypothyroidism is known to cause arthralgias and arthritis of the small joints of the hands and feet (19). Scleroderma causes synovitis of the joints and joint contractures, which may explain metatarsalgia (20). Metatarsalgia affects mostly women (87%) and is often preceded by extensive use of high heels and standing work. Also, we found a high association of MTP1 arthrosis and hallux valgus with metatarsal pain. We recommend metatarsal padding as a safe and inexpensive alternative in treating metatarsalgia patients.
Footnotes
Acknowledgements
We owe a great deal to our cast technician Raimo Hoffren for pads and insoles and Dr Gerald Netto for doing a language check and correcting our English. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The subjects had given informed consent, and the study protocol was approved by the Ethics Committee of Kuopio University Hospital.
Funding
A research grant from the Kuopio University Hospital was received to support this study.