
Abstract
Background:
Previous studies have suggested that orthoses with different constructions could alter gait parameters in flexible flatfoot. However, there is less evidence about the effect of insoles with proprioceptive mechanism on plantar pressure distribution in flatfoot.
Objectives:
To assess the effect of orthoses with different mechanisms on plantar pressure distribution in subjects with flexible flatfoot.
Study Design:
Quasi-experimental.
Methods:
In total, 12 flatfoot subjects were recruited for this study. In-shoe plantar pressure in walking was measured by Pedar-X system under three conditions including wearing the shoe only, wearing the shoe with a proprioceptive insole, and wearing the shoe with a prefabricated foot insole.
Results:
Using the proprioceptive insoles, maximum force was significantly reduced in medial midfoot, and plantar pressure was significantly increased in the second and third rays (0.94 ± 0.77 N/kg, 102.04 ± 28.23 kPa) compared to the shoe only condition (1.12 ± 0.88 N/kg and 109.79 ± 29.75 kPa). For the prefabricated insole, maximum force was significantly higher in midfoot area compared to the other conditions (p < 0.05).
Conclusions:
Construction of orthoses could have an effect on plantar pressure distribution in flatfeet. It might be considered that insoles with sensory stimulation alters sensory feedback of plantar surface of foot and may lead to change in plantar pressure in the flexible flatfoot.
Clinical relevance
Based on the findings of this study, using orthoses with different mechanisms such as proprioceptive intervention might be a useful method in orthotic treatment. Assessing plantar pressure can also be an efficient quantitative outcome measure for clinicians in evidence-based foot orthosis prescription.
Background
Flexible flatfoot is defined as a condition in which the medial longitudinal arch of the foot collapses during weight-bearing stance. 1 As a result, this situation may affect the normal foot weight-bearing function; thus, abnormal loads will be transferred to the more proximal areas such as knee, hip, and lower back. 2 Furthermore, this situation may alter the biomechanics of the foot and disturb the normal pressure distribution during walking. 3 Ledoux and Hillstrom 4 examined the effect of flatfoot on the plantar vertical force distribution and reported that the forces beneath the hallux were significantly higher than normal subjects. In addition, Queen et al. 5 in a comparative study investigated the influence of flat and normal foot types on force distribution during different athletic tasks. The findings indicated that both contact area and force were significantly higher in medial midfoot in subjects with flatfoot during the side-cut task. 5
In order to correct the abnormal load distribution, foot orthoses are commonly prescribed in patients with flatfoot.6,7 Redmond et al. 8 examined the mechanical effect of customized and prefabricated foot orthoses with longitudinal arch supports on pressure distribution within a group of subjects with flatfoot. Their findings showed that both orthoses had shifted the load from forefoot and rearfoot toward the midfoot area while the midfoot contact area had been increased.
Apart from the mechanical effect of insoles, few studies suggest that the effectiveness of orthotic intervention might also be as a result of proprioceptive mechanism.9,10 Nurse and Nigg11,12 examined the effect of foot sensory feedback alteration on plantar pressure distribution during walking and stated that peak pressure and muscle patterns were changed when sensory feedback was altered. They concluded that sensory feedback is important in modification of gait pattern and it can be considered as an approach in orthotic treatment. Some researchers have examined the effect of textured surfaces as a tactile stimulation on muscle activity and kinetic and kinematic of the lower leg.13–15 Nurse et al. 14 reported that textured foot orthosis could alter the electromyography (EMG) activity of the leg muscle as well as ankle joint kinematics in subjects with pes valgus. Stacoff et al. 10 examined the biomechanical effect of orthoses with different mechanical and proprioceptive mechanisms in patients with pes valgus. Stacoff found that combined effect of posting and molding could alter gait parameters more efficiently. 10
Another type of proprioceptive insole is a flat one with an elevation underneath the first ray with the aim of foot plantar surface stimulation, which was introduced by Rothbart. He proposed that in each step, the elevated area enhances the tactile stimulation of the foot plantar surface, which increases afferent sensory feedback from the cerebellum. As a result, with this effective feedback loop, brain creates altered sensory signals and autocorrects the foot hyperpronation.16,17
There are many studies conducted to assess the mechanical effect of insoles with different constructions on gait parameters in foot disorders.6–8,10,13,14,18
According to the authors’ knowledge, there is little known about the effect of insoles with various mechanisms on plantar pressure distribution in flatfoot. Therefore, the aim of this study was to compare the effect of different orthotic interventions including mechanical and proprioceptive mechanisms on plantar pressure distribution in flatfeet. It was hypothesized that plantar pressure distribution, force, and contact area might be different while wearing the prefabricated longitudinal arch support, proprioceptive insole, and the shoe as control condition in subjects with flexible flatfoot.
Methods
Subjects
Twelve male participants with flexible flatfoot (age 22.25 ± 1.54 year, height 178 ± 3.95 cm, and weight 72.9 ± 6.05 kg) were recruited based on the inclusion criteria. The main inclusion criteria included bilateral flatfoot, normal range of motion and muscle strength, no traumatic injuries or surgeries during last 6 months in lower limbs, no pathologic condition or neurologic disorder in feet, and no leg length discrepancy.
First, musculoskeletal lower limb examination was performed by an orthopedic surgeon, and subjects with the records of any physical or neurological disorders in the lower extremities were excluded from the study. The study protocol was approved by the Human Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, and all the participants filled the consent form before participating in the experiment.
Procedure
Three randomized testing conditions using two different orthoses and wearing only the shoe were carried out. The first orthosis was prefabricated longitudinal arch support that was commercially available in Tehran (Protho). This prefabricated device was full length and made of two layers: ethyl vinyl acetate at the bottom layer and 1-mm-thick leather layer on the top (Figure 1). The second insole was proprioceptive orthosis made of rubber and covered by cloth, which is produced by Posture Dynamics Co. (Olympia, WA, USA) This orthosis was a flat 2-mm-thick insole with no arch support; it had a 3-mm wedge as an elevation area extending from the navicular to the hallux and slopped medial to lateral (Figure 2). A pair of sport shoes that allowed easy replacement of different insoles was used for all participants.

Prefabricated foot orthosis.

Proprioceptive foot orthosis.
Plantar pressure data were measured by Pedar-X system (Novel GmbH, Munich, Germany) at the sampling frequency of 50 Hz. 19 This system has been used in similar studies, and repeatability of the system has been shown.5,20 The system consists of a hardware component and a software component. The hardware includes flexible insoles comprising 99 capacitive sensors, Pedar box (data logger) and battery pack (to be fastened on the waist of the subject), cables to attach the logger to the insoles, and a Bluetooth dongle. The Pedar-X software contains all necessary functions to calibrate sensors, collect and view data online, and to do the step analysis. Three sizes of Pedar insoles were used to accommodate the range of foot sizes in this study. Prior to data collection, insoles were calibrated according to the manufacturer’s manual for each subject.
At first, Pedar insoles were placed inside the shoes, between orthosis and plantar surface of the foot, and participants were asked to walk with shoes only, shoes with prefabricated insoles, and shoes with proprioceptive insoles while the sequence of the tests was assigned randomly. After getting familiar with each test condition, subjects were asked to walk at self-selected gait velocity along a 9-m walkway. Four trials were accomplished for each test, and all participants completed 12 trials.
Data analysis
Plantar pressure data were transferred online to the personal computer via Bluetooth. For each testing condition, 15 steps were selected by using Pedar-X step analysis software. After exporting data with American Standard Code for Information Interchange (ASCII) format to Microsoft Excel, the foot was divided into seven masks: medial heel, lateral heel, medial midfoot, lateral midfoot, first ray, second and third rays, and fourth and fifth rays (Figure 3). According to the output of Pedar system, the following three variables were calculated and analyzed for each mask: peak pressure (kPa), maximum force (N/kg), and contact area (cm2). The maximum force was normalized to the body weight for each subject.
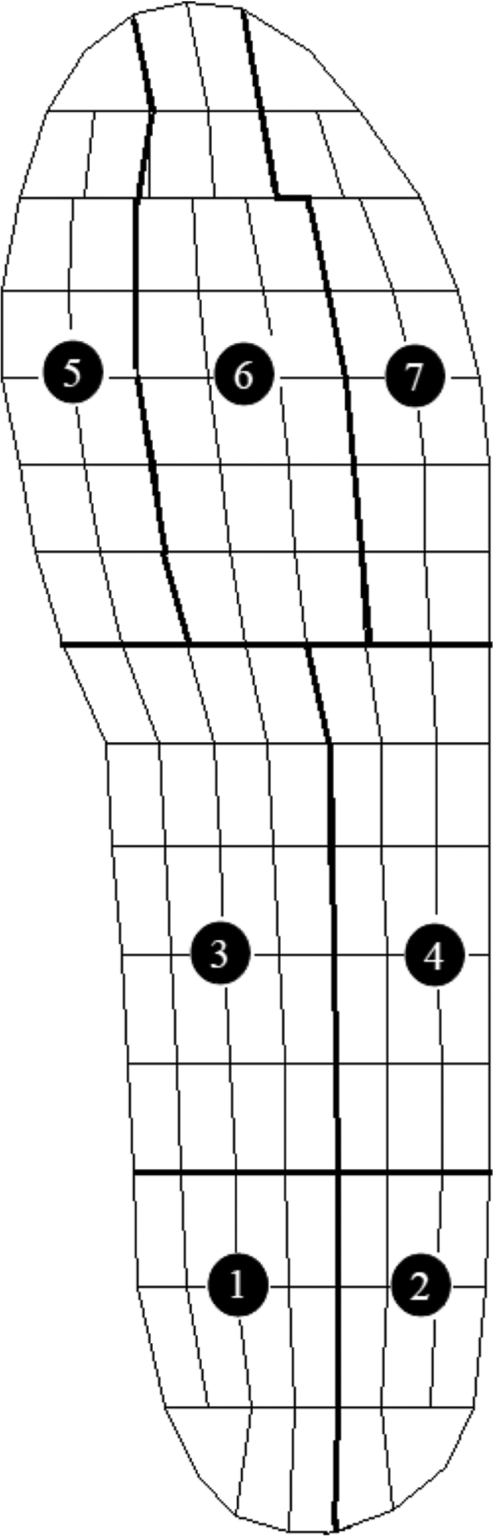
Anatomical division of foot into seven regions.
All statistical analyses were performed by SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test assured the normal distribution of the data (p > 0.05). Independent t-tests were applied to assess differences between right and left feet. One-way repeated measures analysis of variance (ANOVA) with Bonferroni-adjusted post hoc test was used to compare measurement between each condition. Alpha levels were set at 0.05 for all tests.
Results
There was no significant difference between the contact area, peak pressure, and maximum force between the right and left feet, and thus, all analyses were fulfilled for right foot. According to the results, no significant difference was found in contact area between the three conditions in all masks, while contact area was higher in medial midfoot for prefabricated insole in comparison with the other conditions. Moreover, peak pressure was significantly higher in midfoot and first ray for prefabricated insole compared to the shoe only case. However, there were no significant differences in peak pressures between prefabricated and proprioceptive insoles in all masks; it was significantly lower in the prefabricated insole than the shoe only condition in medial heel and second and third rays.
The maximum force was significantly higher in medial and lateral midfoot for prefabricated insole than the shoe only and proprioceptive insole conditions. Tables 1, 2 and 3 show the mean and standard deviation values of contact area, peak pressure, and maximum force in detail.
Mean (SD) values of contact area (cm2) for the three conditions in all masks.
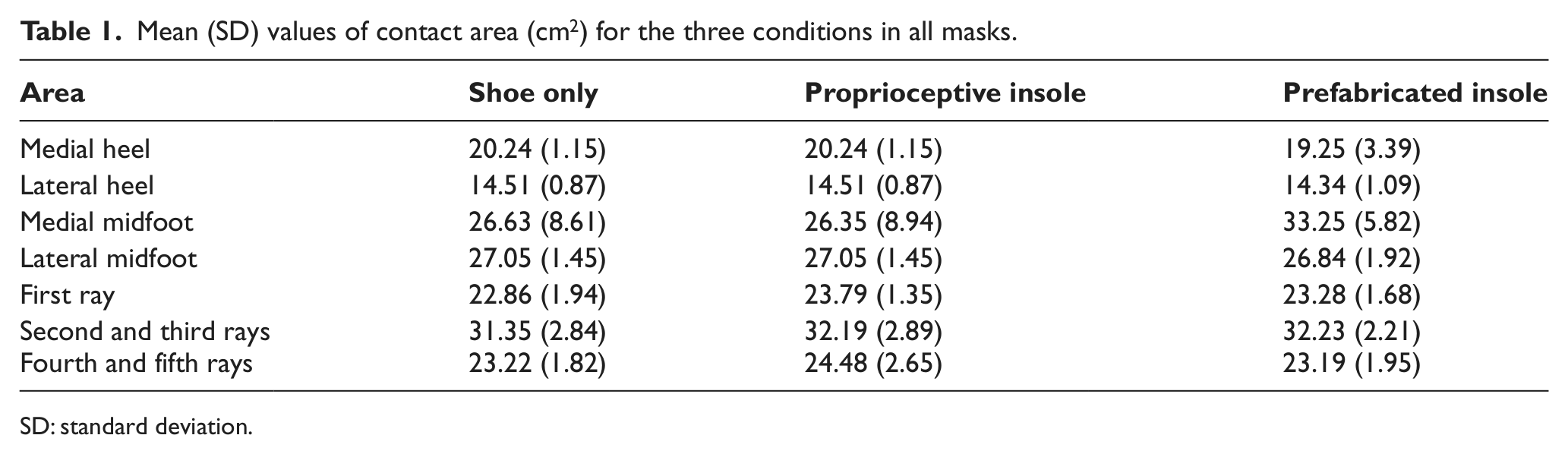
SD: standard deviation.
Mean (SD) values of peak pressure (kPa) for the three conditions in all masks.
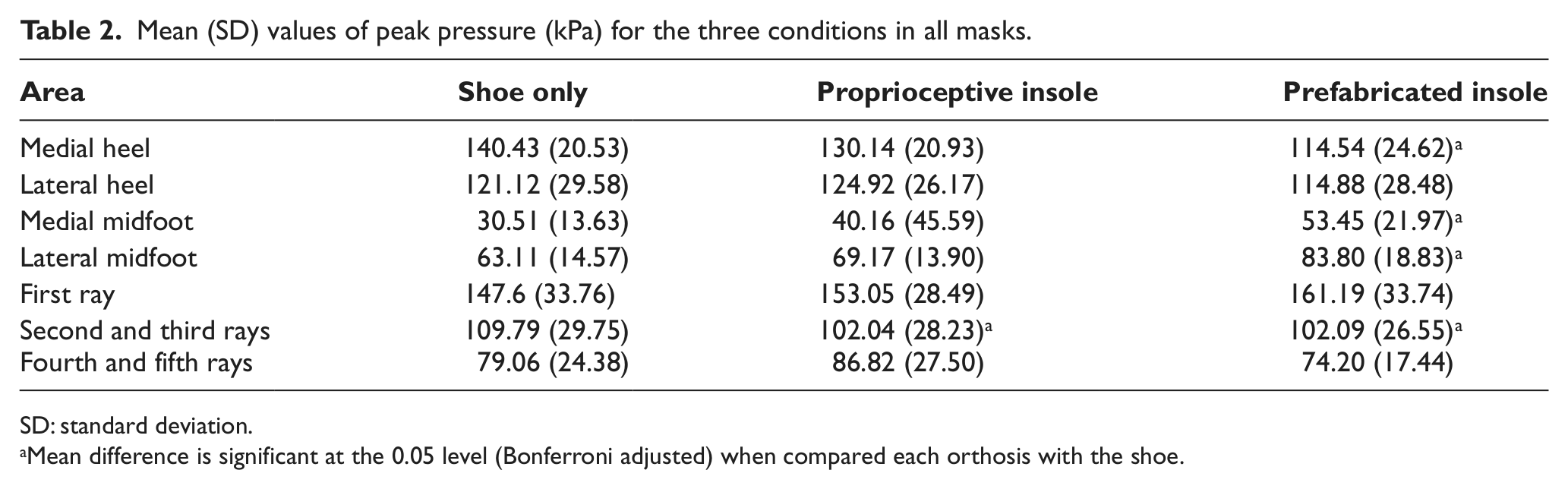
SD: standard deviation.
Mean difference is significant at the 0.05 level (Bonferroni adjusted) when compared each orthosis with the shoe.
Mean (SD) values of maximum force (N/kg) for the three conditions in all masks.
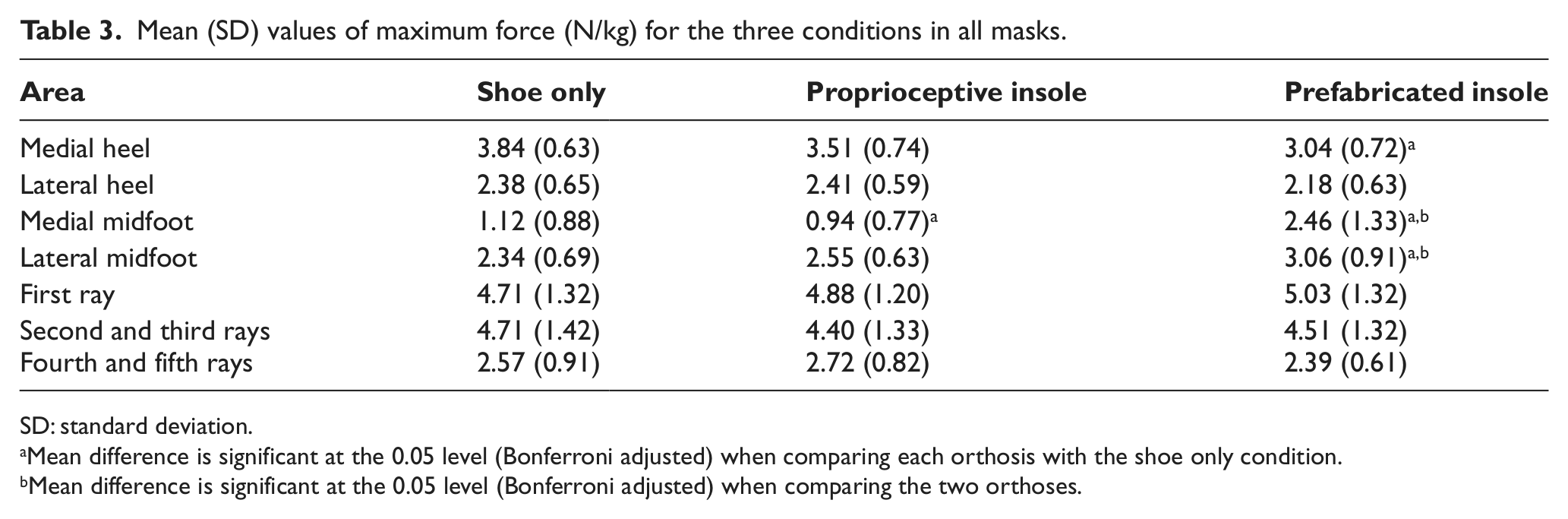
SD: standard deviation.
Mean difference is significant at the 0.05 level (Bonferroni adjusted) when comparing each orthosis with the shoe only condition.
Mean difference is significant at the 0.05 level (Bonferroni adjusted) when comparing the two orthoses.
Discussion
According to the hypothesis of this study, there were some differences in plantar pressure distribution and forces underneath the foot among three conditions of control, namely, shoe only, prefabricated insole, and proprioceptive insole in subjects with flexible flatfoot. However, we did not find any significant differences in contact area between these three conditions.
In the heel area, prefabricated insole reduced peak pressure and force significantly in comparison with shoe only, which is in line with previous studies.8,21 It has been proposed that reduction of pressure in heel area might be as a result of two structural mechanisms: medial arch support that leads to transfer of loads from heel into midfoot area and heel cup structure that realigns the calcaneous to a more normal position and redistributes the pressure in prefabricated orthosis.8,21 Findings of the present study for the proprioceptive insole indicate that this insole did not have any effect on heel pressure and force when compared to the other conditions. This insole has a flat structure with no arch support or heel cup; this enhances the possibility that changes in plantar pressure parameters in the heel area may be due to the structural differences between two orthoses.
Findings for prefabricated insole with medial longitudinal arch support showed an increased plantar pressure and maximum force in midfoot region compared to the proprioceptive insole and shoe only, which were also similar to the findings of previous studies. Redmond et al. 8 and Bus et al. 21 suggested that the arch support mechanism shifts the load from forefoot and hindfoot toward midfoot and causes increased pressure in this area. However, the proprioceptive orthosis had some effects (compared to control and insole conditions) in reducing forces in medial midfoot, indicating that plantar stimulation can alter the biomechanics of the foot during walking. Our finding supports the effectiveness of this insole in reducing hyperpronation.16,17 Indeed, Rothbart 16 as a designer of this proprioceptive insole has explained that the main function of this insole is to create tactile stimulation underneath the medial part of forefoot, which produces altered sensory signals from the brain and causes postural shift in foot twist. Nurse et al. and Hatton et al. suggested that the changes in foot sensory feedback through orthoses with tactile stimulation alter plantar pressure, muscle activity, and gait parameters.11 –15 The concept of using the tactile feedback systems under the foot is based on the foot–brain connection. That is, the tactile stimulation enhances sensory input to the plantar surface of the foot and might modify the foot posture.10,11,17
Similar to the findings of the previous studies, the prefabricated insole reduced the peak pressure in forefoot area significantly compared to the control condition.6,8,21 The proprioceptive insole significantly decreased the pressure beneath the second and third rays compared to the shoe only condition. However, pressure increased underneath the fourth and fifth rays, which has been explained by designer of this new insole as a basic function of this insole to reposition the forefoot into supination. 16
The purpose of this study was to compare the plantar pressure distribution among insoles with different constructions while walking with flatfoot. The findings of the present study revealed that the prefabricated insole with longitudinal arch support could redistribute plantar pressure effectively, which is inconsistent with the results of the previous comparable studies.6,21 Although proprioceptive orthosis could shift forces in the midfoot area effectively, there were no significant changes in plantar pressure distribution by this insole, which might be as a result of the immediate effect of the insole in this study. Therefore, further research is required to define the long-term efficacy of insoles with various sensory stimulation mechanisms in flatfoot patients.
Conclusion
Based on the results of this study, insole construction could have different effects on plantar pressure distribution in flatfeet. With the proprioceptive insole, forces in medial midfoot area was reduced when compared to the prefabricated insole and shoe only conditions; thus, it might be considered that insoles with sensory stimulation may alter sensory feedback of plantar surface of the foot and may lead to some changes in plantar pressure parameters in flexible flatfoot.
Footnotes
Acknowledgements
We would like to thank the Department of Prosthetics and Orthotics of USWR for the valuable help throughout this study.
Conflict of interest
The authors report no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.