
Abstract
Background and Aims:
The open abdomen technique is a standard procedure in the treatment of intra-abdominal catastrophe. Achieving primary abdominal closure within the initial hospitalization is a main objective. This study aimed to analyze the success of closure rate and the effect of negative pressure wound therapy, mesh-mediated medial traction, and component separation on the results. We present the treatment algorithm used in our institution in open abdomen situations based on these findings.
Material and Methods:
Open abdomen patients (n = 61) treated in Tampere University Hospital from May 2005 until October 2013 were included in the study. Patient characteristics, treatment prior to closure, closure technique, and results were retrospectively collected and analyzed. The first group included patients in whom direct or bridged fascial closure was achieved, and the second group included those in whom only the skin was closed or a free skin graft was used. Background variables and variables related to surgery were compared between groups.
Results and Conclusion:
Most of the open abdomen patients (72.1%) underwent fascial defect repair during the primary hospitalization, and 70.5% of them underwent direct fascial closure. Negative pressure wound therapy was used as a temporary closure method for 86.9% of the patients. Negative pressure wound therapy combined with mesh-mediated medial traction resulted in the shortest open abdomen time (p = 0.039) and the highest fascial repair rate (p = 0.000) compared to negative pressure wound therapy only or no negative pressure wound therapy. The component separation technique was used for 11 patients; direct fascial closure was achieved in 5 and fascial repair by bridging the defect with mesh was achieved in 6. A total of 8 of 37 (21.6%) patients with mesh repair had a mesh infection. The negative pressure wound therapy combined with mesh-mediated medial traction promotes definitive fascial closure with a high closure rate and a shortened open abdomen time. The component separation technique can be used to facilitate fascial repair but it does not guarantee direct fascial closure in open abdomen patients.
Keywords
Introduction
The open abdomen (OA) has become a standard salvage procedure for intra-abdominal emergencies to avoid or treat abdominal compartment syndrome (1, 2). The reasons for OA treatment are multifactorial and patients undergoing this treatment are seriously ill. Although the OA strategy can be lifesaving in certain situations, it is also associated with significant complications, such as fluid and protein loss, nutritional problems, formation of enteroatmospheric fistulas, and the development of massive incisional hernias. Conventional treatment includes placement of a skin graft on the granulated OA and repair of the unavoidable hernia later in the second stage. The free skin graft can be safely removed from the bowels when the adhesions from the skin to the bowel have been loosened, usually after 6 months. The skin-grafted bowel is herniated and is at risk for ulcerations and fistula formation. The current aim, therefore, is to achieve primary abdominal closure within the initial hospitalization. This is challenging because patients are still considerably ill at the time of the closure, their nutritional status can be poor, and their wound-healing capacity is compromised. Definitive closure of the abdomen may also be surgically demanding.
A Bogota bag is usually used as a first temporary abdominal closure method, and negative pressure wound therapy (NPWT) is applied as soon as possible (1 –3). NPWT helps to maintain the elasticity and mobility of the abdominal wall by preventing adhesions between the intestines and the abdominal wall and avoids lateralization of the abdominal wall (4). The optimal time for the final abdominal closure is when the distance between the fascial edges is approximately 3–7 cm, the patient’s condition is stable, and nutritional status is good (5). The best result would be direct closure of the fascia and skin. This is not always possible. However, different surgical techniques like component separation (CS) and perforator-saving skin undermining can be used to promote midline closure of the fascia and skin (2, 6). Synthetic or biologic mesh can be used to bridge the fascial defect if the edges of the fascia cannot be directly closed (7, 8). Mesh reinforcement can also be used to strengthen the closure, even after fascial closure is achieved.
In this study, we analyzed various methods used for primary closure of the OA in our institution, and the success rate of the one-stage procedure, that is, reconstruction of the fascial defect. Our aim was to clarify whether individual variables could predict which group of patients would be definitively treated with fascial repair. We also examined the role of CS for closure of fascial defects in the early stage. The CS method is widely used and accepted for the repair of fascial defects in late reconstructions (6, 9). Clinical data regarding its use during primary closure of the OA, however, is limited (10). We also analyzed how often NPWT was used, and whether NPWT treatment with or without mesh-mediated medial traction (MMMT) affected the ability to achieve fascial closure.
Material And Methods
The clinical data of all OA patients treated by plastic surgeons in Tampere University Hospital from May 2005 until October 2013 were collected and analyzed retrospectively. During that period plastic surgeons were involved in treating all OA patients with primary closure. Six patients were excluded from the study since they died before closure of OA could be done. The study was approved by the Ethics Committee of Tampere University Hospital. A total of 61 patients were included in the study. When NPWT was applied, we used vacuum-assisted closure (V.A.C. therapy; KCI, San Antonio, TX, USA). During the last 4 years NPWT was combined with MMMT when possible.
The aim was always to close the fascia directly or by bridging the fascial defect with mesh and then closing the skin. If that was not possible, the skin was mobilized and closed directly on top of the intestines or a skin graft was used. Composite polypropylene meshes were used if a mesh was placed on the intestines. Composite meshes were preferably set inlay whenever possible. Only if there were strong visceral adhesions, the mesh was laid onlay. In cases with strong granulation tissue covering the intestines, a non-composite mesh was used onlay. Re-enforcement of directly closed fascia with a mesh was considered indicated if significant tension existed in the fascial closure line. Meshes were always placed at least with 2–3 cm overlapping of the fascial edge. An absorbable smooth mesh was used in one patient with large traumatic abdominal wall defect in the acute phase. In one patient with significant contamination of the intestines, a biologic mesh was used (Fig. 1).
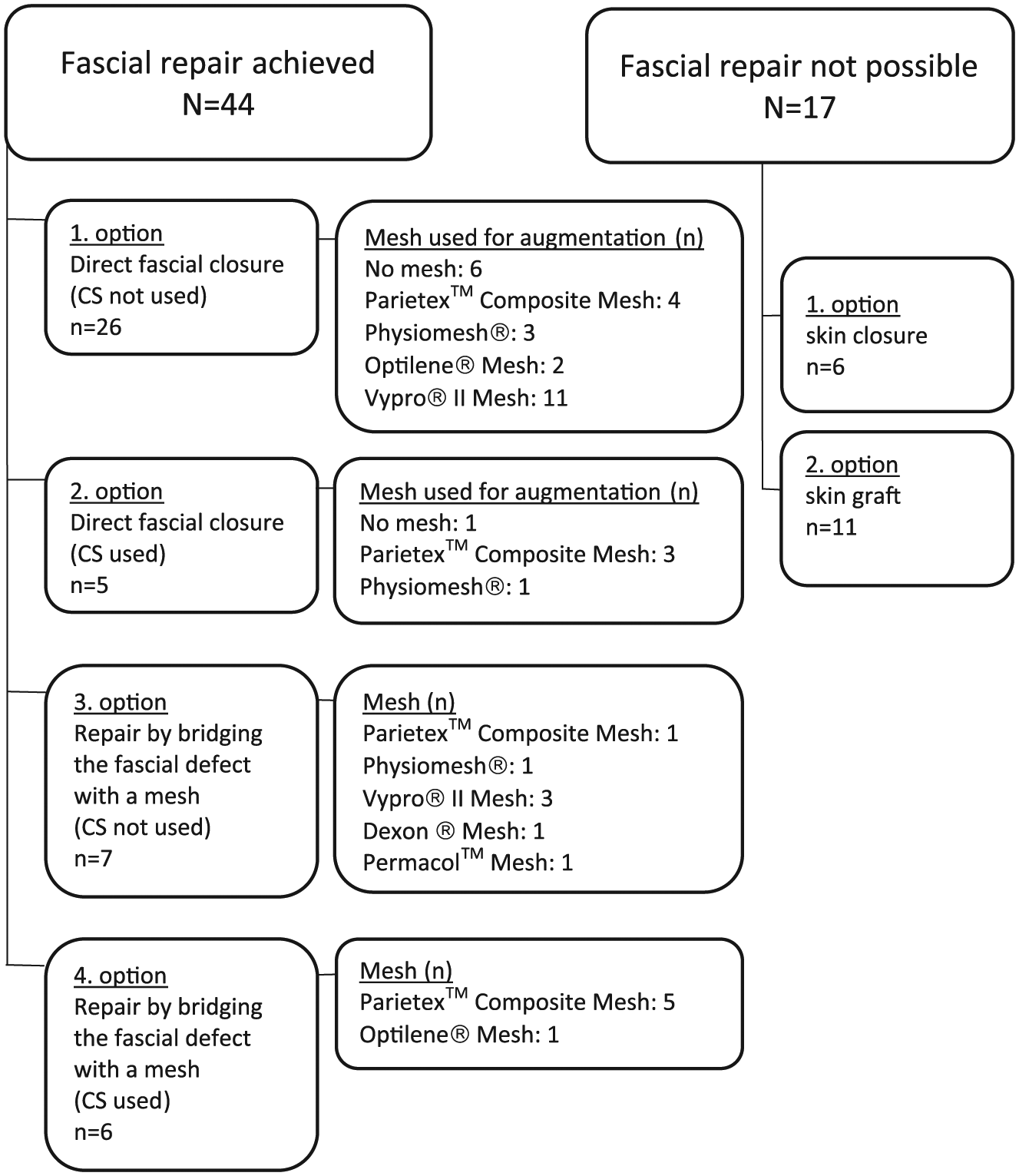
The methods of primary open abdomen closure.
Patient demographic data, treatment prior to abdominal closure, closure technique, and results were collected and analyzed. Mean values, proportions, and other descriptive statistics were presented. Differences between groups using continuous variables were assessed using either a Mann–Whitney test or a Kruskal–Wallis test. Proportion differences between groups were evaluated with Fisher’s exact test. The p-value limit for statistical significance was set to 0.05. Statistical analyses were performed with IBM SPSS Statistics, Version 23.0.
Results
Mean patient age was 64 years and most of the patients were men (Table 1). Peritonitis and postoperative fascial dehiscence were the most common reasons for OA treatment (Table 2). The mean albumin value of patients for whom this value was recorded was 17.2 g/L (range 8–30). During the study period, 15 of the patients died after the primary hospitalization (median = 6.8 months; range = 1.1–60.6 months). One patient died during hospitalization after primary abdominal closure of OA.
Patient characteristics (n = 61).
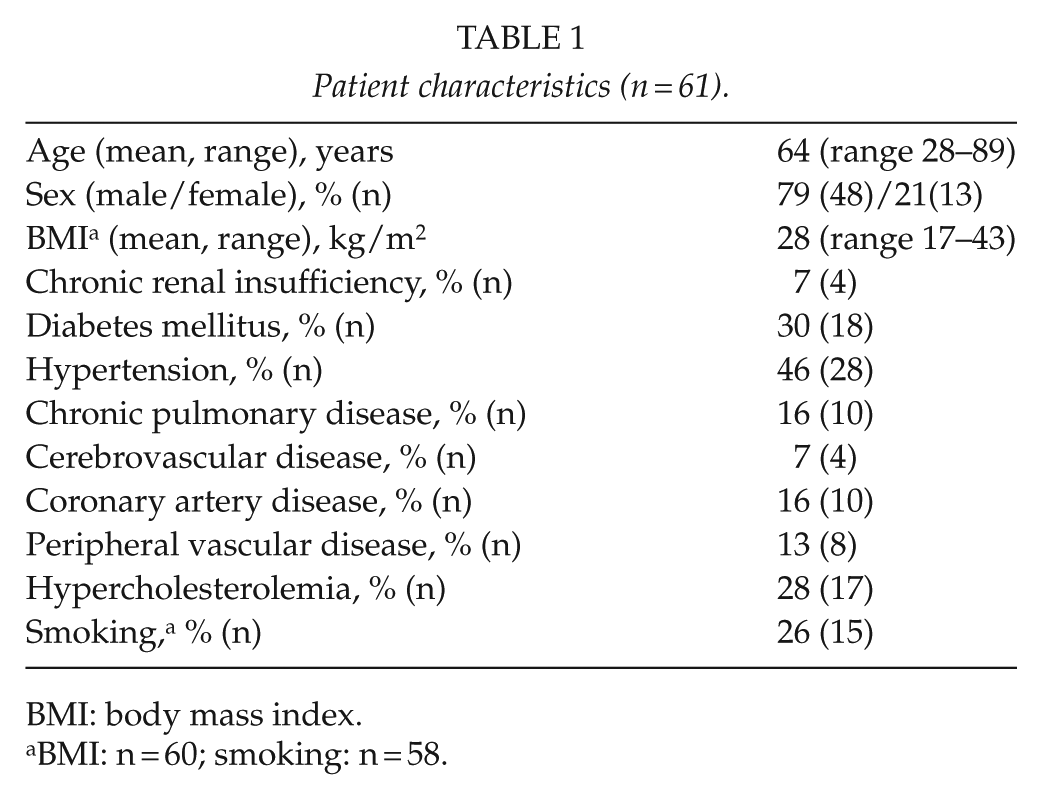
BMI: body mass index.
BMI: n = 60; smoking: n = 58.
Patient diagnoses (n = 61).
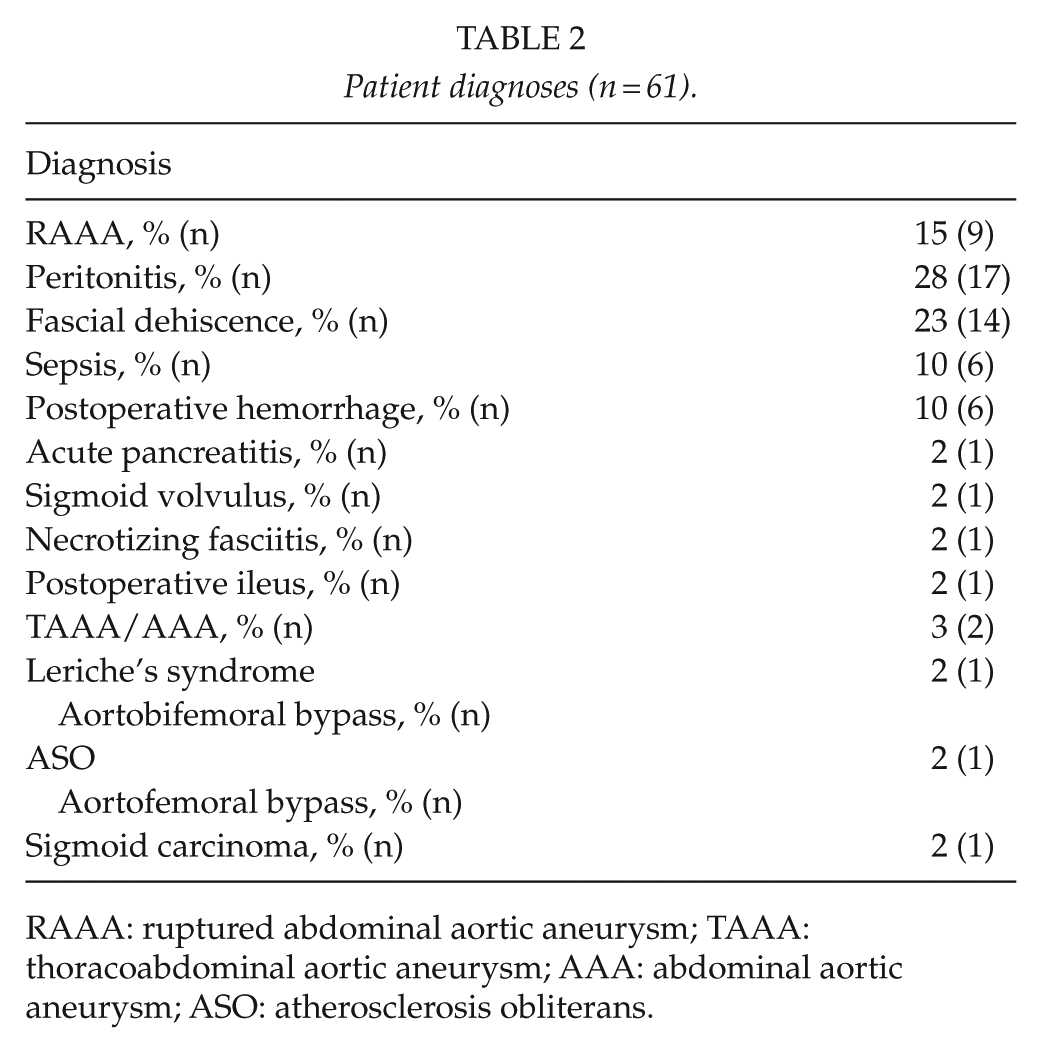
RAAA: ruptured abdominal aortic aneurysm; TAAA: thoracoabdominal aortic aneurysm; AAA: abdominal aortic aneurysm; ASO: atherosclerosis obliterans.
The methods of primary closure are shown in Fig. 1. The patients were divided into two groups based on the method applied. One group (72.1% of the patients) comprised patients whose fascial defect repair was successful either by closing the fascia directly or by bridging the fascial defect with mesh. The other group (27.9% of the patients) comprised patients for whom only the skin was closed or the defect was covered by a free split-thickness skin graft. The fascial repair was not performed in critically ill patients and in patients with extremely poor nutritional status. However, skin was closed whenever possible to avoid skin grafting. There were no statistically significant differences in the basic illnesses between these patient groups. Nevertheless, 41.2% of the patients with only skin closure or skin graft had diabetes compared to the 25.0% in the fascial defect repair group. Although the difference was quite large, it was not statistically significant (p = 0.229). Neither body mass index (BMI; p = 0.252), smoking habit (p = 1.000), nor age (p = 0.251) significantly affected whether or not the patient had a definitive fascial closure. The 22.8-day mean duration of OA was significantly shorter in the patient group with fascial defect repair compared to the 32.3-day mean duration in the group with skin closure only or with skin graft (p = 0.017).
In patient groups with or without successful fascial defect repair, NPWT was applied for temporary closure of the OA in 53 (86.9%) patients. Distribution of different temporary abdominal closure methods, that is, NPWT and MMMT, NPWT only, or no NPWT, in these patient groups is presented in Table 3. NPWT was not used in severely infected wounds or on bowels at risk of perforation. In some of these patients, a delayed NPWT could be started. Direct fascial closure was achieved in 25 (83.3%) of the patients treated with both NPWT and MMMT, and fascial reconstruction by bridging the defect with mesh in 3 (10.0%) of the patients treated with NPWT and MMMT. Direct fascial closure was achieved in only five (21.7%) of those treated with only NPWT, and fascial reconstruction by bridging the defect with mesh in eight (34.8%) of the patients treated with only NPWT. Direct fascial closure was achieved in only one (12.5%) of those treated without NPWT, and fascial reconstruction by bridging the defect with mesh in two (25.0%) of the patients treated without NPWT. The fascial repair rate was highest in the group treated with both NPWT and MMMT, compared to those treated with NPWT and no MMMT, and those treated without NPWT (p = 0.000). There was no difference in the basic illnesses between patients in whom NPWT was or was not used. The number of smokers was significantly higher in the group that was not treated with NPWT (66.7%) compared to those who were treated with NPWT (21.2%; p = 0.034).
The use and timing of NPWT and MMMT in open abdomen patients before final closure (n = 61).
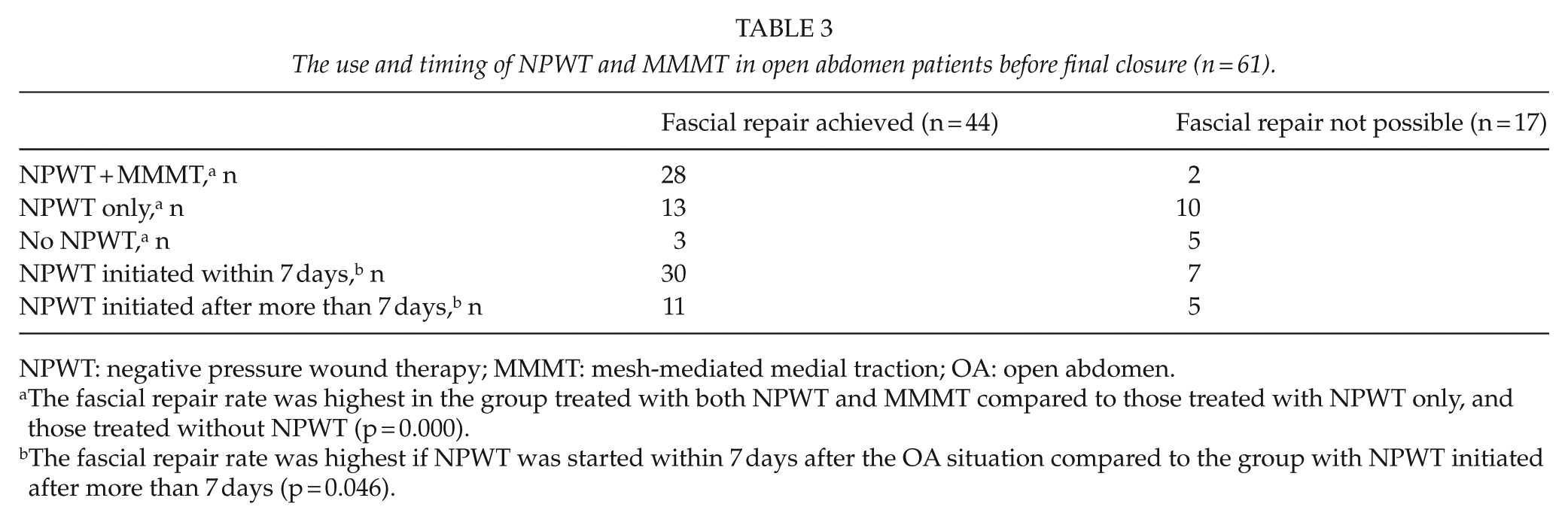
NPWT: negative pressure wound therapy; MMMT: mesh-mediated medial traction; OA: open abdomen.
The fascial repair rate was highest in the group treated with both NPWT and MMMT compared to those treated with NPWT only, and those treated without NPWT (p = 0.000).
The fascial repair rate was highest if NPWT was started within 7 days after the OA situation compared to the group with NPWT initiated after more than 7 days (p = 0.046).
When evaluating the treated OA patients as a whole, the OA lasted an average of 20.6 days (range 9–47) in cases in which NPWT was used in combination with MMMT. When NPWT was used without MMMT, the average number of days of OA was 30.0 (range 4–64) and when NPWT was not used, the average was 30.6 (range 9–61) days. The duration of the OA was shortest in the group treated with both NPWT and MMMT (p = 0.039). The BMI value was lowest in the group without NPWT treatment (23.9) compared to both those with NPWT (28.0) and those with NPWT and MMMT (28.7; p = 0.028).
The policy in our clinic is to start treatment with NPWT within the first week of OA, before the occurrence of a frozen abdomen. Our data included 37 (60.7%) patients whose treatment with NPWT was initiated within 7 days of beginning the OA, 16 (26.2%) patients for whom NPWT was started more than 7 days after beginning the OA, and 8 (13.1%) patients had no NPWT treatment at all. Starting times of NPWT among patient groups with and without successful fascial repair are presented in Table 3. Of those whose treatment with NPWT was initiated within 7 days, fascial repair was accomplished directly in 21 (56.8%) cases and by bridging the defect with mesh in 9 (24.3%) cases. The skin was closed directly without fascial repair in five (13.5%) cases and a skin graft was used for two (5.4%) patients. These results were significantly different from those in the group in which NPWT was started more than 7 days after the OA (p = 0.046). In that group, the fascia was closed directly in nine (56.3%) cases and by bridging the defect with mesh in two (12.5%) cases. A skin graft was used for five (31.3%) patients and none of the patients underwent skin closure only without fascial repair. The mean OA time of the group treated with NPWT within 7 days of the OA was significantly shorter than that of the group treated with NPWT more than 7 days after the OA (21.6 vs 31.8 days; p = 0.011).
In 44 patients (72.1%), the fascial defect was repaired during the primary hospitalization (Fig. 1). Of these patients, 31 (70.5%) underwent direct fascial closure. Among these 31 patients, the CS technique was performed in 5 and additional support was provided by mesh in 4. Additional support was provided with mesh in 24 (77%) of the patients in the direct fascial closure group. In 13 patients (29.5%) in the fascial repair group, mesh was used to bridge the fascial defect, and among these 13 patients, the CS technique was used in 6.
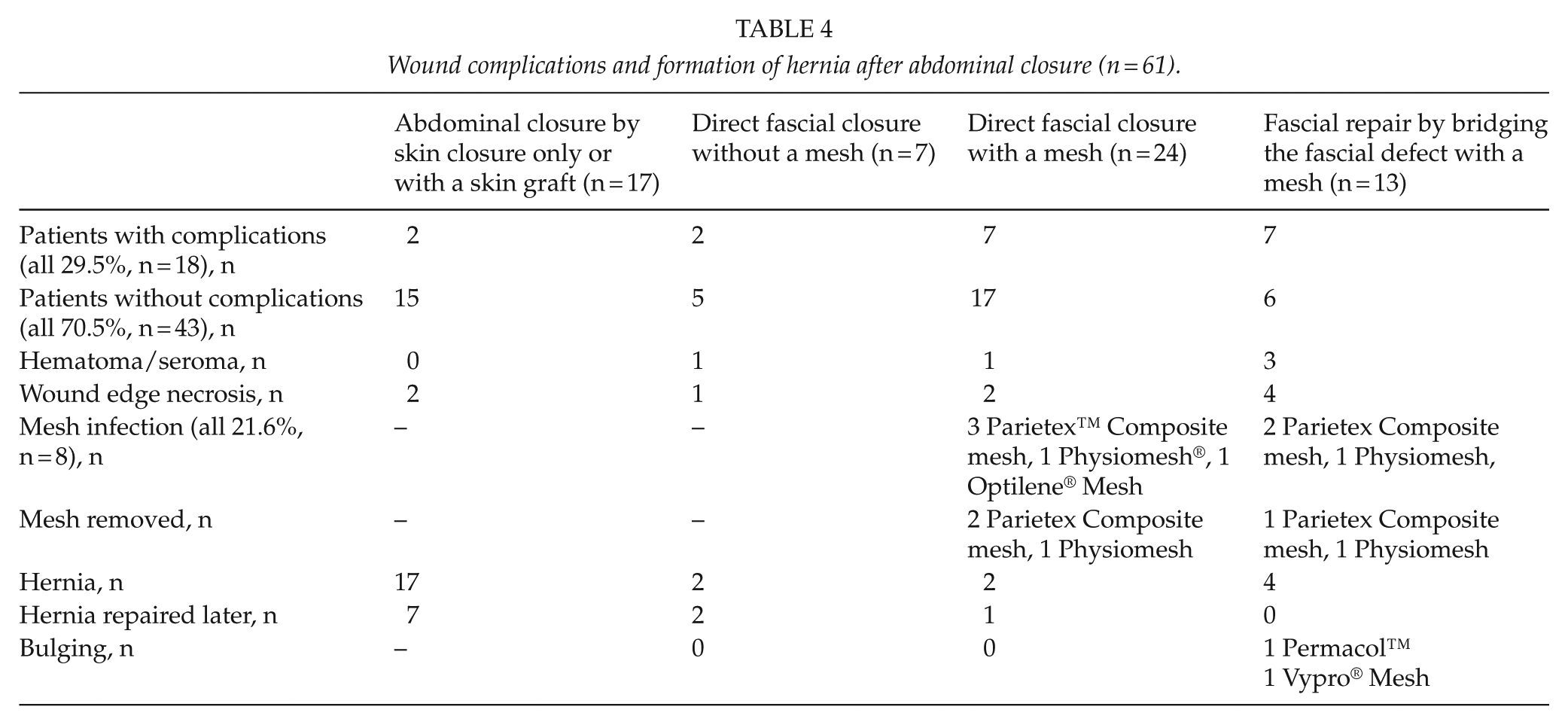
In eight patients (21.6%), a mesh infection was detected. Five meshes were removed totally and two partially. Seven hernias in a patient group without primary fascial repair were corrected later. In the patient group with primary fascial repair, eight hernias were detected later on and three out of them have been repaired (Table 4). The rate of hernia formation in direct fascial closure group without mesh was 33.3% (n = 2) and correspondingly in patient group with direct closure with a mesh it was 10.0% (n = 2). In a patient group by bridging the fascial defect with a mesh, the rate of hernia formation was 30.8% (n = 4).
Wound complications and formation of hernia after abdominal closure (n = 61).
Discussion
OA has become increasingly applied as a treatment for complex abdominal problems. Complications related to OA, especially when managed using the traditional two-stage system, are major burdens for the patients. Early definitive closure of fascial defects is a key factor in the prevention of these complications (1). Attempts toward definitive closure of the abdominal wall during the initial hospitalization, however, might be hampered by the medical instability, poor nutritional status and wound-healing, acute edema, and inflammation of the wound bed (11).
Closure of the fascial defect was achieved during the primary hospitalization in more than two-thirds of OA patients in this study. The fascial defect was repaired by direct fascial closure in nearly three-quarters of the patients, and by bridging the fascial defect with synthetic mesh in the remaining patients. This number of patients achieving direct fascial closure is consistent with earlier reports (5, 12, 13). Most of the patients underwent NPWT as a temporary fascial closure method. The research data collection period was quite long in this study. NPWT was first used without MMMT, but during the last 4 years NPWT was always combined with MMMT when possible. Otherwise, the treatment protocol was the same during the study period. Closing method and indications to use mesh and to choose which mesh to use were decided with same principles. Our results indicated that use of NPWT increases the definitive fascial closure rate either by direct fascial closure or by bridging the defect with mesh. Based on our findings, the closure rate was further increased up to 90% when NPWT was combined with MMMT. In addition, most of the patients treated with NPWT in combination with MMMT achieved direct fascial closure.
Our results demonstrated that NPWT combined with MMMT significantly shortens the OA time compared to that of patients treated with NPWT only or without NPWT. This finding is consistent with previous studies (5, 12, 14). The mean duration of OA was less than 3 weeks. This is important because closing the fascia is highly unlikely if NPWT treatment exceeds 3 weeks (15, 16). If closure is delayed, the OA progresses to a frozen abdomen (15 –18). NPWT combined with MMMT extends the window of opportunity for delayed primary closure of the fascia, even up to 1 month (5). It also delays the onset of a frozen abdomen as it delays the formation of adhesions between the anterolateral abdominal wall and visceral contents and creates medial traction on the abdominal wall (4, 5, 13). In our protocol, the aim is to start NPWT treatment within 1 week. The OA time is significantly shorter when that aim is reached.
Use of the CS technique for late ventral hernia reconstructions is well described in Ramirez et al. (6) and Ko et al. (9). Rasilainen et al. (10) studied the benefits of the CS technique in facilitating primary fascial closure after OA. They found that CS was a feasible method for assisting primary fascial closure in critically ill surgical patients treated for OA. Their recommendation is to use the CS technique at the end of the OA treatment. In our study, the CS technique was always used at the time of OA closure. We also found the CS technique beneficial to promote fascial closure, either by direct fascial closure or by closing the fascial defect partly with bridging mesh. Contrary to results of Rasilainen et al. (10), the use of the CS technique did not guarantee the success rate of direct fascial closure in our study. Only 45% of the patients for whom the CS technique was used achieved direct fascial closure. Edema, inflammation, adhesions, and visceral swelling may impair the motility and sufficiency of the musculo-fascial flap achieved by fasciotomy and release of the external abdominal muscle. On the other hand, if the fascia were not directly closed, closure was achieved using bridging mesh, which contributes to prevent late hernia formation.
Our findings did not demonstrate a significant association between a specific basic illness and the success of the definitive fascial repair. Smoking status, age, and BMI also did not affect the closure result. The number of diabetes patients tended to be higher among the OA patients with only skin closure or skin graft. This may be an indication of the poorer healing capacity in this patient group. The recorded mean albumin value at the time of closure was very low among all patients. This finding likely reflects the poor nutritional status, which will certainly affect the surgical success. An interesting finding was that, BMI was significantly higher when NPWT was used, and there were more smokers in the group in which NPWT was not used. One reason for this could be that OA and a loose abdominal wall might be easier to manage with NPWT, especially in obese patients. One-fourth of the patients had some healing problems such as wound edge necrosis or hematoma and/or seroma formation. In addition, one-fifth of the meshes used were infected. One-fifth of the patients in fascial repair group had later hernia formation. The amount of complications was in line with the previous literature (5, 13).
A routine use of a synthetic mesh in patients with bridging the fascial defect is in our opinion justified. Infections of the mesh occurred in 3/13 cases and hernia formation rate in this group was 30.8%. The use of absorbable or biologic mesh would have led to an inevitable hernia formation and a need for a secondary correction in all bridged cases later on. In our series, 9 out of 13 patients in bridging group healed without complication (i.e. mesh infection/hernia) resulting in permanent healing of the abdominal wall. The mesh infections in our series did not lead to major problems and could be handled with total or partial removal of the mesh or by conservative means. However, in patients with mesh augmentation of a directly closed fascia with tension, a permanent composite mesh seams not to be justified. In all, 5 out of 24 meshes were infected in this group and 4 of 5 infections occurred in composite mesh group. The mesh serves as a temporary augmentation for direct healing of fascia during the initial period of tension and thus theoretically an absorbable or biologic mesh could be considered in these cases to control mesh infection.
In summary, our results together with those of previous studies support the beneficial role of NPWT combined with MMMT, to promote definitive fascial closure in the treatment of OA patients (5, 12, 13). A very high fascial closure rate can be reached and the OA time can be shortened by combining these techniques. The CS technique can be used to facilitate definitive closure but it does not significantly increase the direct fascial closure rate. The retrospective nature of the study has limitations, since the gathered data may be incomplete.
Based on our experience and the present results, the following algorithm is used in our clinic: the OA is initially covered with a Bogota bag allowing constant visual attention of the intra-abdominal situation and rapid reaction for possible complications. The Bogota bag is replaced with NPWT within 1 week, and MMMT is started immediately. After recovery of the patient and treatment with combined NPWT and MMMT, the fascia is closed directly whenever possible. If direct closure is not achieved, CS is considered. If fascia closure is not achieved even after CS, a bridging mesh repair is performed. Only in critically ill patients who do not tolerate extensive surgery, the fascia is left open and direct skin closure attempted. If this is not possible, a free skin graft is applied. A synthetic mesh is used routinely in patients with bridged fascial repair. However, the risk of mesh infection should always be considered carefully. In patients with augmentation of a directly closed fascia, an absorbable or semi-absorbable mesh is considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Details
The study was approved by the Ethics Committee of Tampere University Hospital.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.