
Abstract
Background and aims:
The goal after open abdomen treatment is to reach primary fascial closure. Modern negative pressure wound therapy systems are sometimes inefficient for this purpose. This retrospective chart analysis describes the use of the ‘components separation’ method in facilitating primary fascial closure after open abdomen.
Material and methods:
A total of 16 consecutive critically ill surgical patients treated with components separation during open abdomen management were analyzed. No patients were excluded.
Results:
Primary fascial closure was achieved in 75% (12/16). Components separation was performed during ongoing open abdomen treatment in 7 patients and at the time of delayed primary fascial closure in 9 patients. Of the former, 3/7 (43%) patients reached primary fascial closure, whereas all 9 patients in the latter group had successful fascial closure without major complications (p = 0.019).
Conclusion:
Components separation is a useful method in contributing to successful primary fascial closure in patients treated for open abdomen. Best results were obtained when components separation was performed simultaneously with primary fascial closure at the end of the open abdomen treatment.
Keywords
Introduction
Open abdomen (OA) is increasingly used in critically ill surgical patients (1–3). The initial laparostomy procedure is simple to perform and often results in improved organ functions in patients with abdominal compartment syndrome (ACS) or intra-abdominal hypertension (IAH) (4, 5). The potential problems develop later during the OA treatment and are mostly associated with prolonged temporary abdominal closure (TAC) treatment and delay in fascial closure. The longer the duration of the TAC treatment, the more common are the complications, (6).
The methodology of TAC treatment has evolved during the last decades. Plain plastic sheet (Bogota bag) has been mostly replaced by systems creating topical negative pressure conditions into the open abdominal cavity (7–9). Primary fascial closure rates of higher than 90% have been reported with the combination of commercial vacuum-assisted closure system and polypropylene mesh (VACM) generating continuous fascial traction (10–12).
The components separation (CS) technique has mostly been used in elective reconstructive surgery of the abdominal wall (13–15). Especially in the repair of complex midline ventral hernias, this technique offers increased flexibility of the abdominal wall and enhances its mobility toward midline to cover the defect (16). This technique has been reported to result in superior improvement of the functionality of the abdominal wall and quality of life (17). Furthermore, Saulis and Dumanian (18) showed that CS decreases significantly postoperative recurrence of complex ventral hernias.
This study was designed to investigate the role of CS as a part of primary fascial closure in critically ill surgical patients treated for OA. The association with specific complications of OA and mortality were analyzed.
Material and Methods
The study was performed as a single institution retrospective chart analysis of 16 consecutive critically ill surgical patients undergoing CS to facilitate delayed primary closure of the OA. All patients were admitted and treated at the Helsinki University Central Hospital between April 2007 and May 2013. During this time period, 136 patients were treated with OA which in 94% was associated with nontrauma emergency surgery conditions such as severe acute pancreatitis or secondary peritonitis. The CS procedure was performed either during the TAC treatment or simultaneously with the primary fascial closure at the end of the OA treatment. No patients were excluded.
Temporary Abdominal Covering
For temporary abdominal covering, the ‘vacuum and mesh mediated fascial traction’ technique was used for 14 patients, commercial VAC (V.A.C.® Abdominal dressing system; KCI, San Antonio, Texas, USA) was used for 1 patient and plain Bogota bag without topical negative pressure therapy for 1 patient.
Vacuum and Mesh Mediated Fascial Traction
This method has been previously described in detail (10, 12). In brief, the commercial VAC (V.A.C.® Abdominal dressing system; KCI, San Antonio, Texas, USA) was used. The intra-abdominal contents were first covered by a polyethylene sheet followed by suturing of an oval-shaped polypropylene mesh to the fascial edges. A polyurethane sponge was placed on the mesh and finally covered with occlusive sheets. The system was connected to a suction apparatus creating continuous topical negative pressure. TAC changes were performed every 2 to 3 days in the operating theater or bedside at the intensive care unit (ICU). During the TAC changes, fascial edges were approximated by tightening the mesh by suturing it in the midline.
Components Separation
The indication for using the CS procedure was the anticipated inability to achieve safe and timely primary fascial closure. The CS procedure was performed either during the TAC treatment or at the time of primary fascial closure. Due to the limited previous experience of using CS with this indication, both approaches were used to confirm the feasibility of the procedure. The aim of performing CS prior to actual closure was to decrease the tension between the fascial edges and thus facilitate the mesh mediated traction effect enabling earlier closure. In these 7 patients, fascial closure was not possible at the time of the CS procedure due to the wide gap between the fascial edges. In the remaining 9 patients, CS was performed at the time of primary closure to lower the tension at the suture line and thus decrease the risk of fascial dehiscence. In 12 patients, CS was performed using a minimally invasive approach via short bilateral transverse skin incisions at the level of umbilicus and in 4 patients through a subcutaneous route. In the minimally invasive techniques, the skin incisions were made at the lateral margin of the rectus abdominis muscle and the aponeurosis of external oblique muscle was identified. In the subcutaneous approach, the aponeurosis was located via sharp subcutaneous dissection from midline laterally adjacent to the fascial surface over the rectus abdominis muscle. In both techniques, the aponeurosis of external oblique muscle was incised vertically 2 cm laterally to the edge of the rectus muscle and the incision was continued cranially over the costal margin and caudally to the level of the arcuate line. For 1 patient, the incision was limited to lower abdomen with cranial margin at the umbilicus. Finally, blunt dissection was used to create space between external and internal oblique muscles to optimize the mobility of the abdominal wall. When done at the end of TAC treatment, the fascia was finally closed at midline with either interrupted 1-Vicryl (Ethicon, Johnson&Johnson, Somerville, New Jersey, USA) or continuous 1-PDS suturing (Ethicon, Johnson&Johnson).
Statistical Analysis
Statistical analyses were performed using IBM® SPSS® Statistics version 19 for Windows® (Armonk, New York, USA). Fisher’s exact test was used for comparison of subgroups.
Results
Patients
A total of 16 consecutive critically ill surgical patients treated for OA who had a CS performed during or at the end of the TAC treatment were analyzed. The indications for laparostomy were manifest ACS or IAH, prophylaxis of IAH, or inability to close the abdomen. The duration of OA treatment before CS varied from 5 to 41 (mean 15) days. Detailed patient characteristics are summarized in Table 1.
Patient characteristics, N = 16.
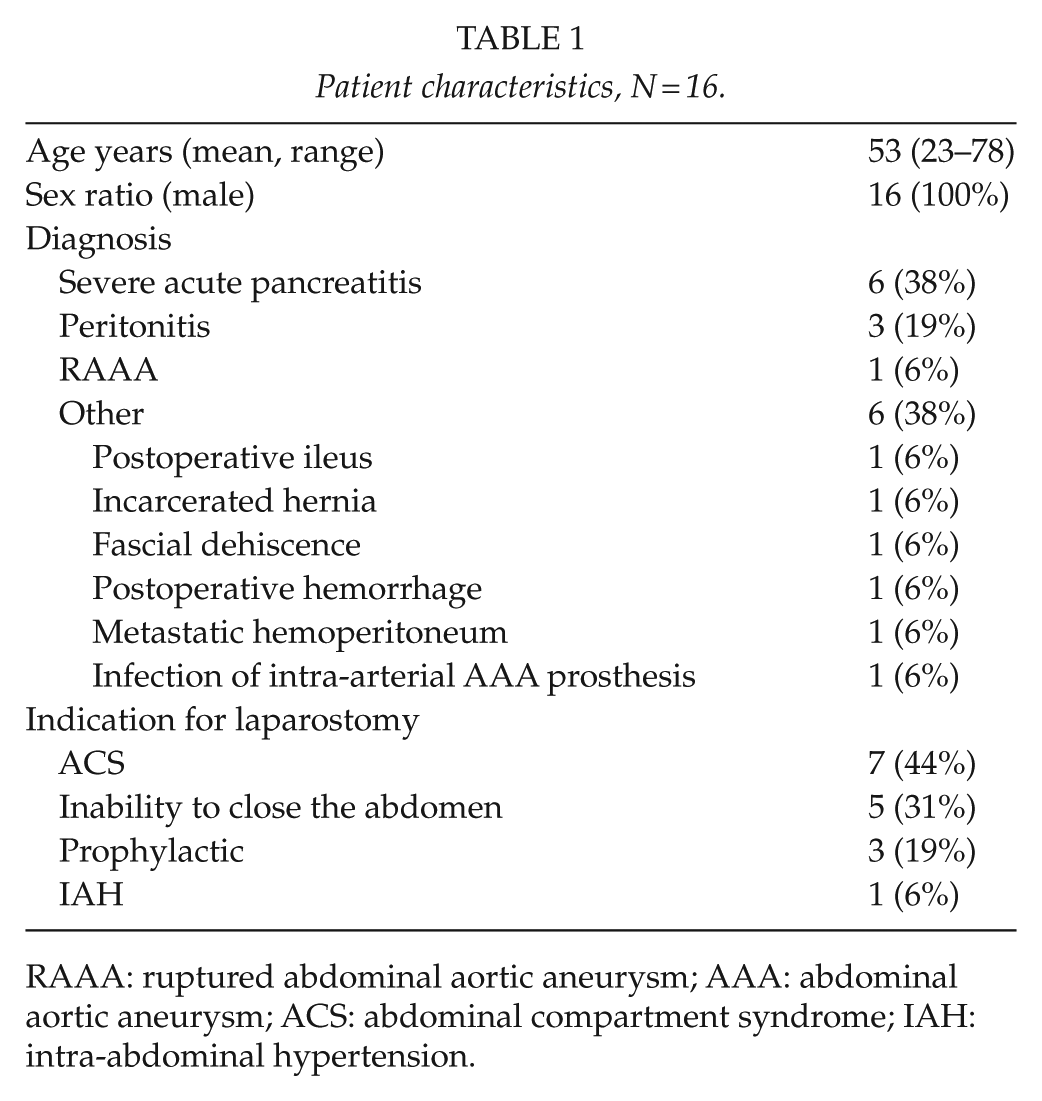
RAAA: ruptured abdominal aortic aneurysm; AAA: abdominal aortic aneurysm; ACS: abdominal compartment syndrome; IAH: intra-abdominal hypertension.
Fascial Closure
Primary fascial closure was achieved in 75% (12/16) of the patients. CS was performed during the TAC treatment in 7 patients and at the time of fascial closure in 9 patients. The duration of OA treatment before CS was 15 (5–41) days in the first group and 15 (6–34) days in the second. Among the latter group, 2/9 patients went through relaparostomy after the initial fascial closure and the CS procedure was performed only at the time of the final fascial closure. All 9 patients with simultaneous CS and fascial closure got along without fascial rupture. In contrast, only 3/7 (43%) of the patients with CS during the TAC treatment reached primary fascial closure (p = 0.019). The detailed characteristics of the 4 patients with unsuccessful closure are presented in Table 2.
Patients with unsuccessful primary fascial closure.
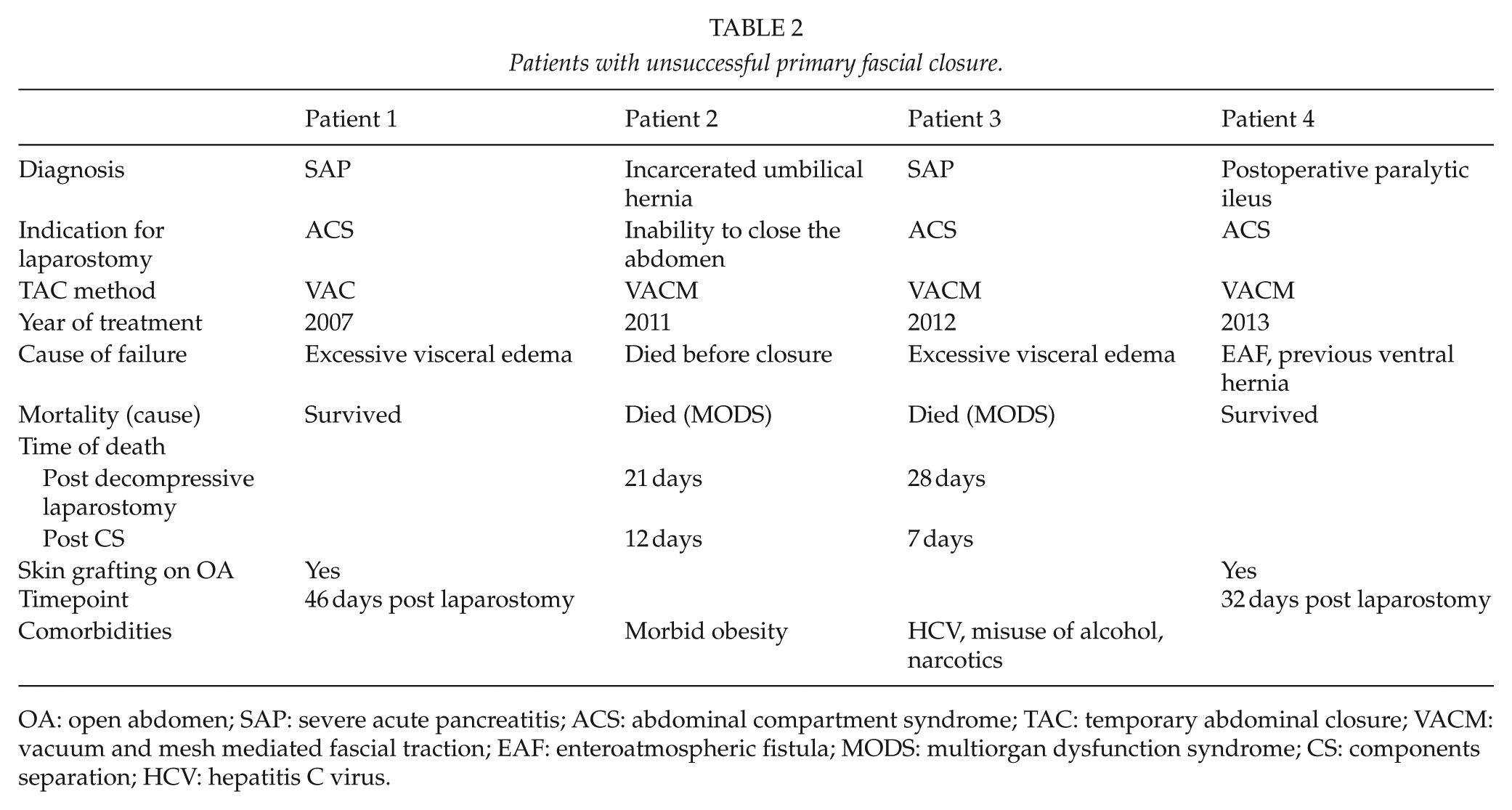
OA: open abdomen; SAP: severe acute pancreatitis; ACS: abdominal compartment syndrome; TAC: temporary abdominal closure; VACM: vacuum and mesh mediated fascial traction; EAF: enteroatmospheric fistula; MODS: multiorgan dysfunction syndrome; CS: components separation; HCV: hepatitis C virus.
Complications Related to OA and CS
Postoperative Hemorrhage and Seroma
Four patients had postoperative subcutaneous hemorrhage in the area where CS was performed (in 3/12 with minimally invasive and 1/4 of patients with subcutaneous CS technique). All underwent evacuation of the hematomas. Two patients developed a seroma into the CS space during the primary hospitalization period, both of these patients after minimally invasive CS.
Wound Infections
A wound infection was detected in 2/12 (17%) and 1/4 (25%) patients with mini-invasive versus subcutaneous CS, respectively.
Enteroatmospheric Fistulae and Planned Hernia
Three out of 16 patients (19%) were diagnosed with an enteroatmospheric fistula (EAF), all fistulas developed before the CS procedure was performed. Two out of these 3 reached delayed primary fascial closure, although 1 of them died 2 weeks after fascial closure. The third patient was treated with a planned hernia strategy. Overall, there were 4 patients with unsuccessful primary fascial closure managed with the planned hernia strategy (Table 2) with 2 survivors (including the one mentioned above).
Mortality
The overall in-hospital mortality rate was 31% (5/16). Two patients (2/5) died of multiorgan dysfunction and 2 (2/5) drifted into prolonged ICU care and interrupted healing. One patient (1/5) died only 6 months later acutely at ward at a follow-up care unit. The deaths did not coincide either with the CS procedure or its complications. There was no difference in mortality between patients with CS during the TAC treatment (2/7; 29%) or at time of primary fascial closure 3/9 (33%). Overall, 2/16 (13%) patients died with OA.
Long-Term Follow-Up
Of the 16 patients, 11 survived through the hospitalization period, but 1 patient died later on during follow-up period that varied depending on the time point of OA treatment from 16 to 89 months. Of the long-term survivors, 8/10 had successful fascial closure and 2/8 (25%) of them developed a ventral hernia. The remaining 2 survivors with the planned hernia strategy are scheduled for reconstructive surgery later on. No other CS-related symptoms or complications were detected during follow-up visits.
Discussion
This is the first report focusing on the utilization of CS in assisting delayed primary fascial closure during OA treatment in critically ill surgical nontrauma patients. In 2007, Kushimoto et al. (19) used bilateral anterior rectus abdominis sheath turnover flaps for similar purpose in nine nontrauma patients with good results . Our results show that CS technique can be safely used to complement delayed primary fascial closure with low complication rate, and it results in high delayed primary fascial closure rate. Notably, these were selected patients in whom traditional OA management was considered inadequate to reach successful delayed primary closure. In the past, a planned hernia strategy was often the only option available when it was not possible to approximate the fascial edges together.
CS is widely used in elective reconstructive surgery of the abdominal wall. The technique was originally described by Albanese (20) in 1951 and later refined by Ramirez et al. (21) in 1990 with the aim of closing the abdomen without prosthetic material. Although the prosthetic materials have significantly developed during the recent years, including the evolution of biological products, their indications and benefits are still controversial (22, 23). This is important especially when operating in contaminated surgical fields (24). To reach a satisfactory and enduring outcome, CS is often used in combination with either synthetic or biological mesh when repairing large ventral hernias in elective patients (25, 26).
According to the original method, the lateral margin of the rectus sheet is bilaterally exposed via a dissection requiring extensive mobilization of skin and subcutaneous tissue (19). This predisposes the patient to hemorrhage and seroma formation. To avoid these adverse effects, minimally invasive techniques have been developed. Maas et al. (27) reported in 1999 a technique with bilateral local incisions lateral to the lateral margins of the rectus abdominis muscle in patients with enterostomae. This approach had the advantage of preserving the musculocutaneous perforators of the deep epigastric circulation especially important in patients with interrupted intercostal blood supply, for example, due to enterostomae. In the present study, both subcutaneous and mini-invasive techniques were used. Four patients were treated with the subcutaneous approach and three (3/4) of these represent the first patients in our series (2007–2009). Only one subcutaneous dissection was performed later (2013) reflecting the development of the mini-invasive technique during the study period.
Although new topical negative pressure TAC systems are effective and associated with very high fascial closure rates, at times the abdominal wall, in particular with an ongoing critical illness, remains immobile and the fascia laterally retracted. In these situations, adjunctive measures are needed to reach primary fascial closure. Our study population represents these difficult situations and was thus managed with TAC and CS but without foreign materials.
The timing of the CS procedure is important. In elective surgery, CS is usually performed at the time of the definitive ventral hernia repair. A follow-up period of 6 months to 2 years after the immediate illness leading to the defect of the abdominal wall is recommended before any reconstructive surgery is attempted (28, 29). In this study, the CS procedure was performed in order to reach delayed primary fascial closure and avoid ventral hernia. We observed that the best outcome is achieved when CS is performed at the time of the primary fascial closure. The reasons for worse results with earlier approach during the TAC treatment are multiple. As mentioned earlier, in our series 57% of patients treated with this approach failed to reach primary fascial closure. Although the ongoing negative pressure TAC therapy and especially VACM treatment offering constant fascial traction are considered very effective in reaching primary fascial closure, it sometimes fails in the most critically ill patients. The four patients in this series with this disappointing end result well represent such challenging conditions, as described in Table 2.
In conclusion, this study demonstrates CS to be a feasible method for assisting delayed primary fascial closure in critically ill surgical patients treated for OA. The timing of CS is critical and should be performed at the end but not during the OA treatment.
Footnotes
Declaration of Conflicting Interests
No conflicts of interest.
Funding
This study was financially supported only by a Helsinki University Hospital research grant for emergency abdominal surgery.