
Abstract
Background and Aims:
Esophageal perforation is a life-threatening disease. Factors impacting morbidity and mortality include the cause and site of the perforation, the time to diagnosis, and the therapeutic procedure. This study aimed to identify risk factors for morbidity and mortality after esophageal perforation.
Patients and Methods:
This retrospective study analyzed data collected from all patients treated for esophageal perforation at the Department of Surgery, University of Schleswig–Holstein, Luebeck Campus, from January 1986 through December 2011.
Results:
Altogether, 80 patients (52 men, 28 women; mean age 65 years) were treated. The cause of perforation was intraluminal in 44 (55%) (group A) and extraluminal in 2 (3%) (group B). Spontaneous perforations were observed in 12 (15%) (group C). Perforations were due to a preexisting esophageal disease in 22 (28%) (group D). The survival rate was higher for group A (82%) than for groups B (50%), C (57%), and D (59%). The distal third of the esophagus had the highest prevalence of perforations (49, 61%) independent of the cause. Mortality, however, was independent of the perforation site. Perforations were diagnosed within 24 h in 57% (n = 46) of patients, associated with a statistically significant lower mortality rate (p = 0.035). Altogether, 40 patients underwent non-operative treatment, and among those 27 had endoscopic treatment. Emergency thoracic surgery was performed in 40 patients: direct suture of the defect (n = 26), partial esophageal resection (n = 11), other (n = 3). Significantly higher morbidity (p = 0.007) and prolonged hospitalization (p < 0.0001) was observed among patients who underwent emergency surgery. Mortality was higher in the surgical group (14/40) than in the non-operative treatment group (9/40) but without statistical significance.
Conclusion:
Intraluminal perforations, rapid initiation of therapy, and non-operative treatment were associated with favorable outcomes. The perforation site did not have an impact on outcomes. Esophageal resection was associated with high mortality.
Introduction
Esophageal perforation is known to be a rare but life-threatening event. Mortality rates of up to 44% were previously reported (1–4).
Ingestion of foreign bodies, tumor-associated perforation, and iatrogenic perforations are the most common causes of perforation. Although perforations associated with blunt trauma or vomiting (e.g. Boerhaave’s syndrome), those that occur during surgery, spontaneous perforation, or those due to previous injury to the esophagus are rare, they must be considered during the diagnostic and therapeutic workup of the patient (5, 6).
The patients’ clinical symptoms at admission and during the course of treatment are highly heterogeneous. This heterogeneity may be the reason for a delayed diagnosis of perforation if the initial clinical presentation is almost asymptomatic. A delay in the onset of treatment and consecutive bacteremia and fungiemia may result in a substantial inflammatory reaction of the surrounding tissue and rapid development of the systematic inflammatory response syndrome, mediastinitis, and sepsis (4, 7, 8).
It has been shown previously that the site and extent of the esophageal perforation have a statistically significant impact on patient survival. In addition, the therapeutic algorithm applied in these patients has a major impact on patient survival. Benefits herein were shown for endoscopic procedures, as trans-oral stent application (5, 7). The present report on 80 patients with an esophageal perforation who were treated at a single center over the course of 25 years aimed to investigate the influence of potential risk factors on the morbidity and mortality of the patients.
Patients and Methods
A total of 80 patients with an esophageal perforation were treated at the Department of Surgery (University Hospital of Schleswig-Holstein, Luebeck Campus, Germany) during a period of 25 years (January 1986 through December 2011).
Perforation was identified either during endoscopy or upper gastrointestinal radiography and thoracic computed tomography (CT). Emphysema of the mediastinum that was visible on plain chest radiography was regarded as indirect evidence of a perforation. Bronchoscopy was performed in patients with suspicion of an esophageotracheal fistula. Co-morbidities caused by a perforation, for example, mediastinitis, mediastinal emphysema, pneumonia, and pleural empyema, were evaluated regarding their extent and the need for therapeutic measures using conventional thoracic radiography and CT.
The site of the perforation was defined as to whether it was in the proximal, middle, or distal third of the esophagus. The etiology of the perforation was classified into four groups according to Attar et al. (9): group A, perforation with intraluminal (endoscopic measures, foreign bodies, etc.) pathology; group B, perforation with extraluminal pathology (iatrogenic); group C, spontaneous perforation (Boerhaave’s syndrome); and group D, perforation associated with a preexisting esophageal disease (malignant disease, severe esophagitis).
The patient cohort was further divided into three therapeutic groups: (a) patients with conservative treatment, (b) patients with endoscopic treatment (stent application), and (c) patients who underwent surgery. Patients who switched from initially conservative therapy to surgery were allocated to the surgical treatment group for statistical analysis. The conservative and endoscopic groups were combined in a non-operative group for statistical analysis. The two patients in group B were excluded from the analysis because of the small size of the group.
For endoscopic therapy, full covered self-expandable stents with expanded length of 80–140 mm (medwork, Höchstadt/Aisch, Germany) were used. Major complications were defined as the need for treatment on intensive care unit or the need for re-intervention. After the local ethics committee accepted the clinical trial, patient data were reviewed and entered into an electronic database followed by a retrospective evaluation.
Statistical analysis was performed with the Statistical Package for Social Sciences for Windows (SPSS 18.0, SPSS Inc., Chicago, IL, USA). Pearson’s χ2 test was used to compare categorical variables. The Mann−Whitney U test was used to compare continuous variables because of the size of the patient groups. Statistical significance was indicated at p < 0.05.
Results
During the investigational period, we treated 80 patients (52 men, 28 women) with an esophageal perforation. Clinical symptoms were documented for 66 patients (82%) at admission to the emergency room. The most common initial symptoms were thoracic pain (n = 38, 58%), dyspnea (n = 20, 30%), dysphagia (n = 16, 24%), vomiting and nausea (n = 14, 21%), coughing (n = 6, 9%), and hypovolemic shock (n = 7, 11%).
Table 1 gives an overview of the four patient groups according to Attar et al. (9). Group A (intraluminal pathology) was the largest group, with 55% (n = 44) of all patients. Most frequently, these patients had perforations after diagnostic or endoscopic procedures (diagnostic endoscopy n = 13, dilatation n = 8, stent implantation n = 4, dilatation and stent implantation n = 6, foreign body ingestion n = 13). Group C (spontaneous perforation) and group D (perforations associated with preexisting esophageal disease) included 12 (15%) and 22 (27%) patients, respectively. In group D, the underlying pathologies of the perforation were malignant disease in 14 patients and a severe esophagitis (post-radiogenic, eosinophilic esophagitis) in 8 patients. Group B included 1 patient whose perforation occurred during laparoscopic hemifundoplication and 1 patient who had undergone graft replacement of the infradiaphragmal descending aorta because of an aneurysm.
Categorization of esophageal perforations into groups (A–D) according to etiology with demographic and patient history data.
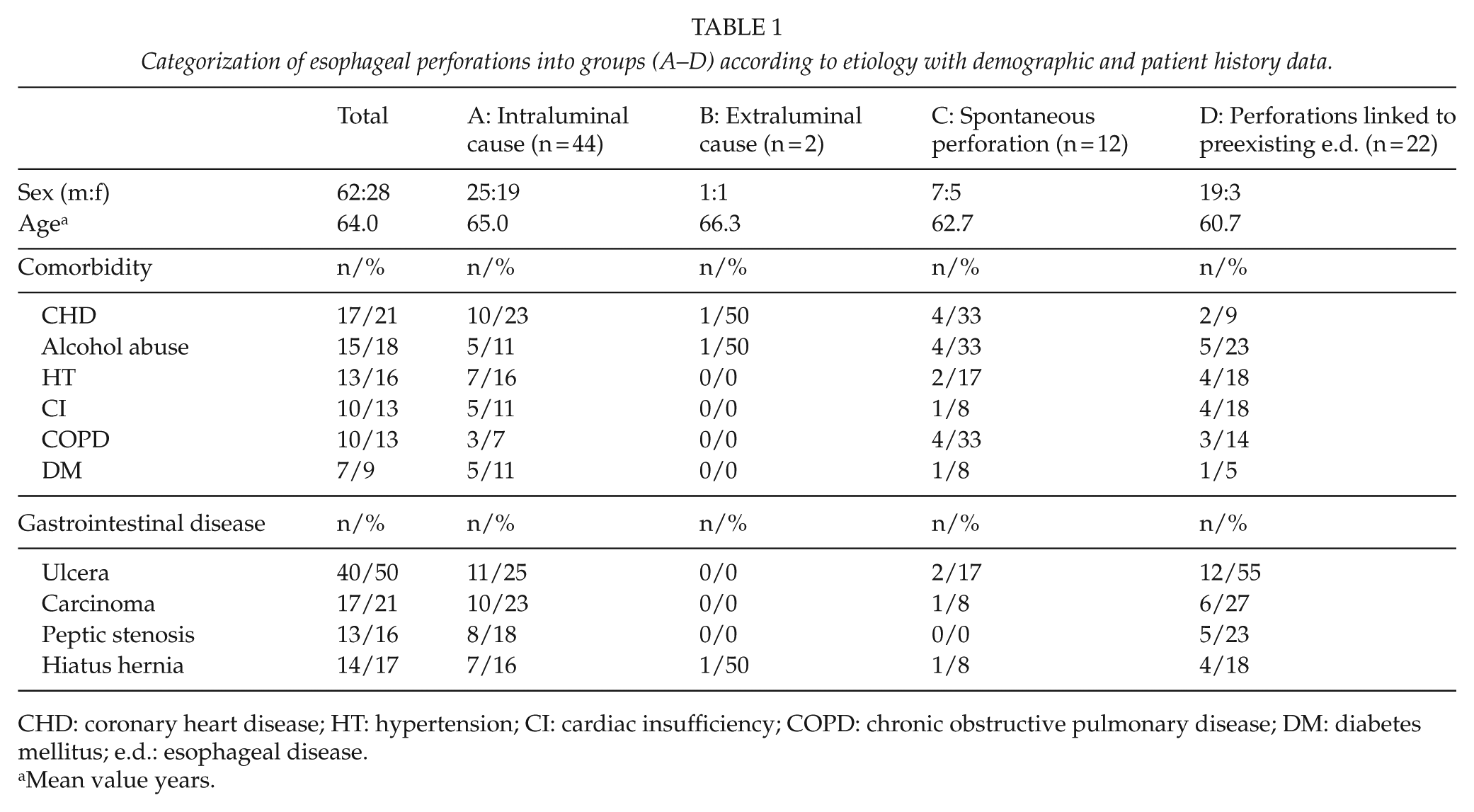
CHD: coronary heart disease; HT: hypertension; CI: cardiac insufficiency; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; e.d.: esophageal disease.
Mean value years.
There were no statistically significant differences between groups concerning demographic parameters or co-morbidities. Group B was excluded from the analysis because of its small size (two patients). Throughout the remaining groups, multiple co-morbidities (e.g. chronic heart disease, alcohol consumption) were observed. Only in a small group of patients with perforations due to foreign body ingestion we were unable to find a correlation with a preexisting gastrointestinal disease or diagnostic procedures.
In all groups, the distal third of the esophagus was associated with the highest incidence of a perforation, independent of the underlying pathology (group A 57%, group C 83%, and group D 59%) (Table 2). The time interval between the perforation and the start of any treatment was less than 24 h in 57% (n = 46) of patients: 35 (80%) patients in group A, 7 (58%) in group C, and 4 (18%) in group D.
Groups (A–D) according to location of perforation, time to diagnosis, therapeutic group, and survival data.
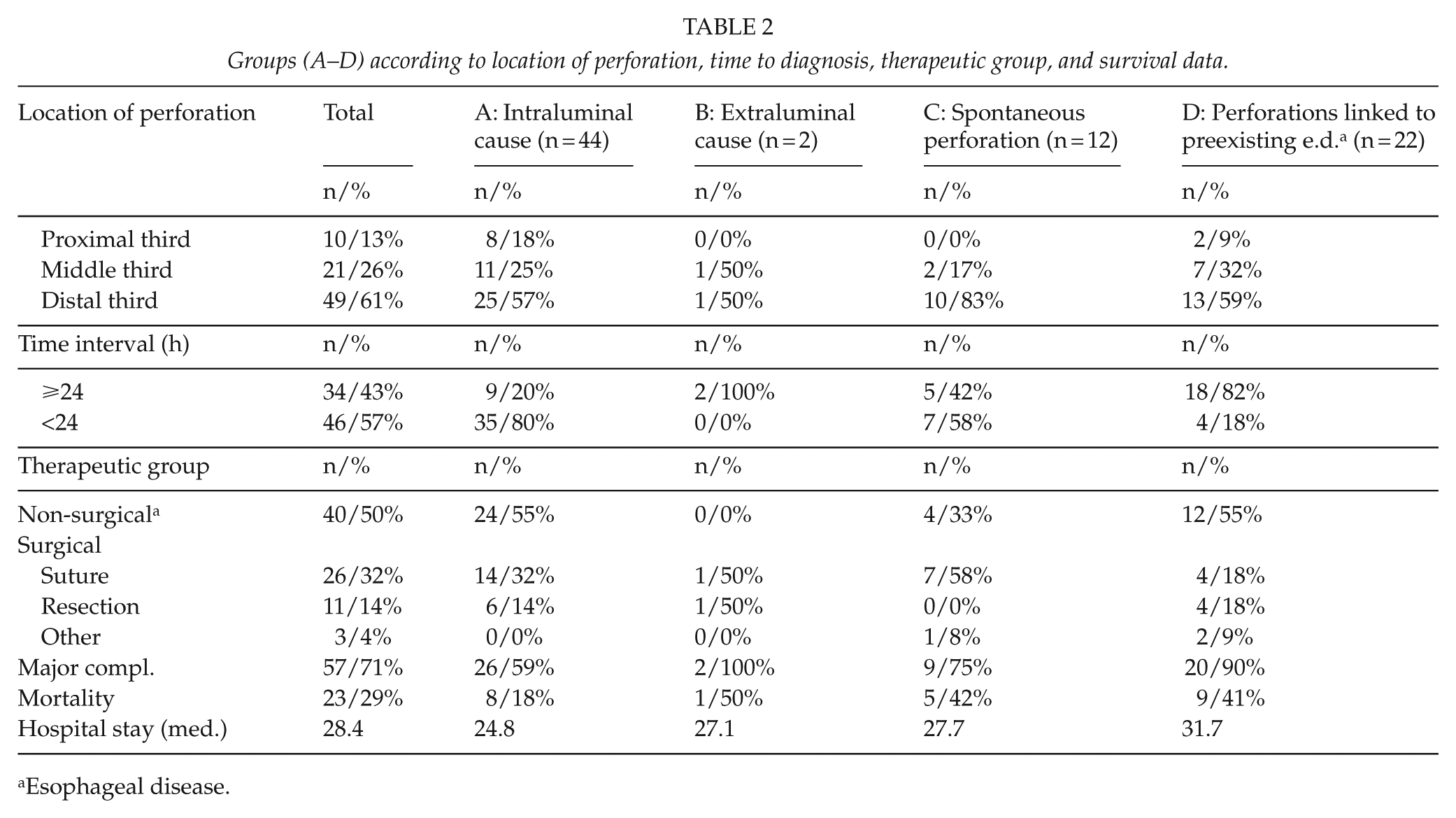
Esophageal disease.
No significant differences were found between the three groups with regard to therapeutic interventions. Irrespective of the etiology, nearly half of all patients were treated non-surgically. The other half required surgery. Analysis of the therapeutic modalities showed that the extent of the perforation and the underlying pathology were decisive when choosing the appropriate therapy.
Conservative treatment with no additional endoscopic intervention was undertaken in 13 patients (16%). A puncture lesion was present in these 13 patients but without mediastinitis or any other complications. In four of these patients, thoracic CT simply showed small collections of air in the mediastinum with no signs of disruption of the continuity of the esophageal wall. Conservative therapy was combined with an endoscopic procedure in 27 patients (34%). Indications for endoscopy included (a) detection of a longitudinal lesion of all layers of the esophageal wall with no wound margin dehiscence and (b) inflammatory reactions in the surrounding tissue (e.g. mediastinitis).
A total of 40 patients underwent surgery (50% of the overall patient population). In all, 26 patients (33%) underwent exploratory thoracotomy or laparotomy and a primary esophageal suture. Seven of these primary sutures were reinforced with fundoplication, four with a pleural flap, and one with a pedunculated peritoneal flap. Subsequent esophageal resection was necessary in two of the patients after the primary esophageal suture proved insufficient.
Primary esophageal resection was performed in 11 patients (14%). Indications for esophageal resection were (a) perforations that resulted in the destruction of more than one-third of the esophageal circumference and (b) long perforations with partial destruction of the esophagus. After the initial discontinuity resection in the 11 patients, the enteric continuity was restored with an esophagogastrostomy in 6 patients and colonic interposition in 2 patients. Five patients died before continuity could be restored because of multiorgan failure. Three patients were treated with individual concepts in extremis (mediastinoscopy and drainage, gastrotomy to remove an arodated stent, palliative collar esophagostomy).
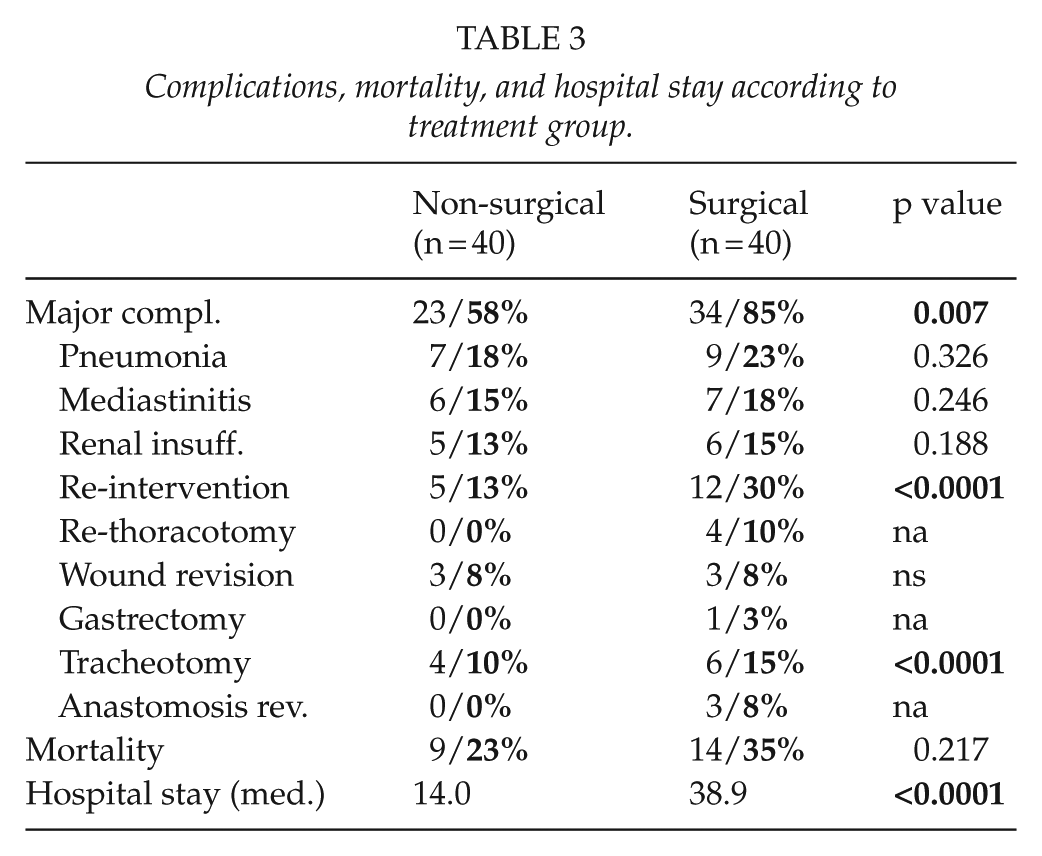
The incidence of major complications in the surgical therapy group was significantly higher than in the group of patients treated conservatively or who underwent endoscopic treatment (Table 3): non-operative (n = 23, 57%) versus surgical (n = 34, 85%) (p = 0.007). Particularly, re-interventions differed among groups (p = <0.0001). A comparison of major complications over the course of treatment showed that group C (75.0%, n = 9) and group D (90.9%, n = 20) had higher complication rates than group A (59.1%, n = 26). The results of group B are shown in Table 2 but were not included in the statistical analysis due to small group size. The length of hospitalization was significantly longer for patients who underwent surgery (14 vs 40 days, p < 0.0001).
Complications, mortality, and hospital stay according to treatment group.
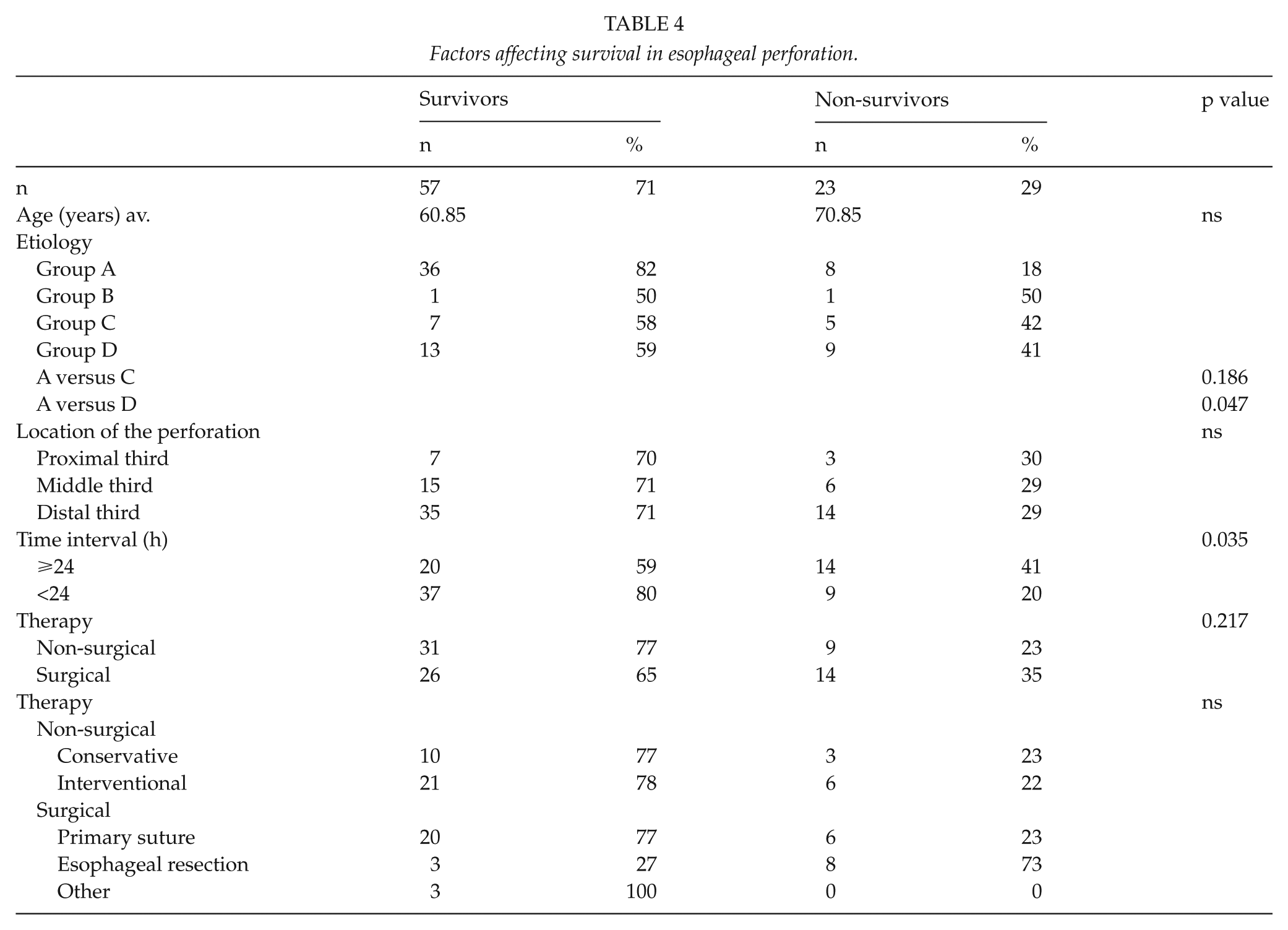
Because of the high 30-day mortality rate for the total patient cohort (29%, n = 23), we performed a subgroup analysis (Table 4). With respect to overall mortality, we found statistically significant differences for the four etiological groups. There was a statistically significant difference in overall survival between groups A and D (p = 0.047). There were no statistically significant differences, however, in regards to the perforation locations. A statistically significant advantage for survival was observed if the diagnosis was secured within 24 h after perforation (p = 0.035). Analysis of the various therapeutic options showed a lower mortality for the non-surgical approach, but the difference did not reach statistical significance. The survival rate among patients with the non-surgical approach was 77% (n = 31), whereas survival in the surgical approach group was 65% (n = 26). In a further subgroup analysis, the results showed a worse outcome especially for those who underwent esophageal resection (n = 11) and individualized surgical measures (n = 3).
Factors affecting survival in esophageal perforation.
Discussion
Despite major advances in diagnostic and therapeutic procedures, esophageal perforation remains life-threatening. Poor outcome is a result of complex interactions of factors that include complex co-morbidities, delayed treatment, and management of the perforation. These factors determine the fate of the patients. Minimal invasive options as endoscopic stenting and laparoscopy are at hand nowadays and have to lead to an improved outcome after esophageal perforation.
The aim of this study was to analyze mortality differences between treatment methods and varying timing of treatment.
Various diagnostic procedures have been established for patients with a suspected esophageal perforation. Some provide only indirect signs of an esophageal perforation (e.g. thoracic radiographic detection of a pleural effusion or free air). Others allow direct visualization of the perforation. Traditionally, the upper gastrointestinal radiographic series has been promoted as a diagnostic tool for direct detection of perforation. Currently, however, this technique has been completely replaced by contrast-enhanced high-resolution thoracic CT. Together with precise identification of the perforation site, thoracic CT provides information about the soft tissue of the mediastinum and pleural space (10–12). The most important observations with relevance for therapeutic decisions at an early stage are evidence for mediastinitis, pneumonia, or pleural empyema.
This study supports implementation of thoracic CT as the gold standard for diagnosing esophageal perforation and especially its co-morbidities (30% of patients present with pneumonia and 35% with mediastinitis at admission to our department). Contrast-enhanced high-resolution thoracic CT thus appears to be the diagnostic method of choice for primary diagnosis of perforation.
Gastrointestinal endoscopy is not the diagnostic method of choice, despite the opportunities for a direct diagnosis and endoscopic therapeutic options. A major disadvantage of gastrointestinal endoscopy is that it does not allow assessment of potentially associated disease. High intraluminal pressure due to gas inflation may also contribute to spreading pathogens, thereby worsening the disease (13, 14). Although endoscopy is therefore an option of second-level importance, it is indicated to retrieve foreign bodies and to place esophageal stents in combination with thoracic lavage (15, 16). An exception is perforation due to a preexisting esophageal disease. In these patients, a biopsy is often required initially to determine the further course of treatment.
Another pivotal risk factor is the interval before starting therapy. According to the literature, the survival rates in patients with onset of therapy within or after 24 h (4) are significantly different. Among our patient cohort, early start of therapy enhanced the chances of survival (p = 0.035). Also, subgroup analysis of groups A and D showed that group A (with 80% of patients having been treated within 24 h) had a significantly lower mortality rate than the patients in group D (only 18% of patients with early start of treatment) (p = 0.047). Preexisting disease resulted in delayed start of treatment compared with patients presenting with an acute perforation. Patients with preexisting disease had a negative selection bias because of advanced inflammatory reactions in the surrounding tissue. The general chronic nature of the primary disease in group D resulted in tissue dystrophy in the region of the perforation, which was accompanied by a chronically attenuated immune system, particularly in catabolic patients with malignant disease. This negative selection led to a higher incidence of complications during hospitalization in this group. These factors accumulate to a significantly elevated mortality rate (6, 17).
A major second bias of the study was the inhomogeneity of group A. The most common causes for perforation were iatrogenic injuries after endoscopy or endoscopic intervention (n = 24, 55%)—flexible endoscopy (n = 8), rigid endoscopy (n = 5), dilatation (n = 8), endoluminal stenting (n = 3)—together with the ingestion of foreign bodies (n = 13, 30%). The development and implementation of flexible instead of rigid endoscopic instruments has resulted in a substantially reduced risk of perforation over time. Silvis et al. (18) observed perforation rates of 0.1%−0.4% for rigid endoscopy, and Fernandez et al. (19) found frequencies of 0.006%−0.01% for flexible endoscopy. A variety of research groups have described perforation rates of up to 7% for pneumatic dilation of esophageal stenoses, endosonography, or the placement of feeding tubes (20–22).
In this study, the diagnosis was rarely delayed in patients with an iatrogenic perforation. Direct visualization of the perforation was frequently obtained and only 20% of the group A patients had a treatment interval of more than 24 h.
The therapeutic procedure itself also had a statistically significant impact on morbidity and mortality (6, 8). Conservative therapy was described as a combination of parenteral nutrition, calculated antibiotic therapy, and adequate drainage (23, 24). Generally, conservative therapy was possible only in patients without septic parameters. A conservative treatment may be combined with endoscopic placement of covered esophageal stents in patients with large perforations and the risk of persistent leakage (25). Also, in cases where a thoracic collection is present, thoracoscopy or even thoracotomy to debride and drain the site of inflammation could be necessary (26).
Endoscopic treatment also should be preferred in instable patients if source control is sufficiently achievable. Moreover, conservative treatment in general is a therapeutic alternative with low mortality compared to surgical therapy in patients with delayed diagnosis, spontaneous perforation, or preexisting esophageal disease. These results are supported by this study and the results of other research groups (27). Conservative treatment is also indicated in a palliative situation. With regard to localization, it has been reported that patients with perforation in the middle third of the esophagus obtain the greatest benefit from conservative or endoscopic treatment (28).
Modern techniques of endoluminal vacuum drainage over the last years have enhanced the armamentarium of endoscopic treatment even more so a former major drawback of conservative or endoscopic therapy, the inability to obtain adequate source control is diminished.
Concerning the surgical repair of esophageal perforations, direct closure of a perforation with single sutures after limited debridement was the therapeutic standard in patients with older iatrogenic or spontaneous perforations. This approach was supported by several previous publications (4, 6). In contrast, Flynn et al. (29) recommended direct closure with a suture only in patients with fresh perforations to exclude the potential damage to the suture and suture failure in infected tissue. We had four cases of suture insufficiency in the surgical group. All patients had initially delayed diagnosis and wound margins that were infected and needed local limited debridement. The patients were cured after reoperation and placement of an additional fundoplication. In our opinion, a single suture without additional reinforcement is not sufficient in patients who undergo surgical revision of a prior endoscopic or surgical therapy. Various techniques for reinforcing the suture have been recommended in the thoracic region (e.g. pericardial and pleural flap plasties). Depending on the site of the perforation, fundoplication in the gastroesophageal transition zone or a pericardial or pleural flap in the thorax should be therapeutic standard.
Primary resection should be avoided if any possible. It is indicated only in patients with larger esophageal destruction and peri-esophageal inflammatory reactions such as abscess formation, mediastinitis, or the development of complex fistulas (17). If possible, the patient must be stabilized in the intensive care unit before an emergency operation. Due to negative selection, there was a high mortality rate (73%) in this patient group in our study. This poor outcome is often accompanied by extensive co-morbidities in these patients at the time of admission to the hospital (pneumonia, mediastinitis, and septic conditions). Our mortality rate is comparable to other research groups (9, 24). Ohri et al. (30) reported significantly higher mortality and morbidity rates after esophageal resection in the presence of pneumonia underlining our conclusion to reserve this as the last possible option in the treatment of these patients. Esophageal resection must be considered an ultima ratio. The question of primary discontinuity resection as an alternative procedure cannot be addressed definitively by the results of our study because only few patients have undergone such treatment. Discontinuity resection in the emergency situation might be indicated in some patients as an individual therapeutic decision.
We were able to show that both the time to initiation of diagnostic procedures and therapy had a highly significant impact on patients’ outcomes. Patients with a suspicion of esophageal perforation need rapid diagnostic progression with thoracic CT as the standard. Because of the heterogeneity of the patient groups and the underlying causes of perforation, an individual diagnostic and therapeutic approach is required in each case. Because of the major advancements in the treatment of systematic inflammatory response syndrome and endoscopic stent placement, conservative or endoscopic therapy should be preferred to surgery. For clinical practice, the results of this study imply the need to provide a short time to therapy, adequate diagnostic measures to evaluate the extent of the perforation and co-morbidities, and adequate and immediate therapy that is as minimally invasive as possible.
Footnotes
Acknowledgements
M.Z. and M.H. contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.