
Abstract
Background:
In 2009, a classification system for the open abdomen was introduced. The aim of such a classification is to aid the (1) description of the patient’s clinical course; (2) standardization of clinical guidelines for guiding open abdomen management; and (3) facilitation of comparisons between studies and heterogeneous patient populations, thus serving as an aid in clinical research.
Methods:
As part of the revision of the definitions and clinical guidelines performed by the World Society of the Abdominal Compartment Syndrome, this 2009 classification system was amended following a review of experiences in teaching and research and published as part of updated consensus statements and clinical practice guidelines in 2013. Among 29 articles citing the 2009 classification system, nine were cohort studies. They were reviewed as part of the classification revision process. A total of 542 patients (mean: 60, range: 9–160) had been classified. Two problems with the previous classification system were identified: the definition of enteroatmospheric fistulae, and that an enteroatmospheric fistula was graded less severe than a frozen abdomen.
Results:
The following amended classification was proposed: Grade 1, without adherence between bowel and abdominal wall or fixity of the abdominal wall (lateralization), subdivided as follows: 1A, clean; 1B, contaminated; and 1C, with enteric leak. An enteric leak controlled by closure, exteriorization into a stoma, or a permanent enterocutaneous fistula is considered clean. Grade 2, developing fixation, subdivided as follows: 2A, clean; 2B, contaminated; and 2C, with enteric leak. Grade 3, frozen abdomen, subdivided as follows: 3A clean and 3B contaminated. Grade 4, an established enteroatmospheric fistula, is defined as a permanent enteric leak into the open abdomen, associated with granulation tissue.
Conclusions:
The authors believe that, with these changes, the requirements on a functional and dynamic classification system, useful in both research and training, will be fulfilled. We encourage future investigators to apply the system and report on its merits and constraints.
Keywords
Introduction
The evidence available on how to define and treat the abdominal compartment syndrome (ACS) and intra-abdominal hypertension (IAH) has increased over time. An important step in understanding this evidence was the publication of Consensus Documents regarding definitions (1) and guidelines (2) for ACS/IAH in 2006–2007. Consensus was achieved on how to define these conditions, which patient groups were at high risk of developing, and which non-surgical and surgical methods to use to prevent and treat these conditions. Implicit in the consensus process was a commitment to regularly review and update the guidelines. It was thus noted that there remained a need to reach consensus also on how to classify the open abdomen (OA).
The need of a classification system was based on the fact that there are many ways to manage the OA, and that patient cohorts are quite different depending on the epidemiology of the population that an individual center serves. Comparing results between centers is impossible without standardized nomenclature. To address this, a comprehensive classification system was developed in 2009, published by Björck et al. (3). The system was inspired by a previous publication by Swan and Banwell (4), and was developed during two consensus conferences.
There were two aims of that classification system. First is to create uniform reporting standards, facilitating comparisons of groups of patients, studies, as well as meta-analyses. Second is to serve as an educational aid, assisting in defining the aims of different treatment modalities, and in defining strategies. It was concluded that such a classification system needed to be dynamic, allowing the patient to move between different categories, during an often prolonged treatment. The suggested classification system in the 2009 publication is given in Table 1, left half.
Open abdomen classification system.
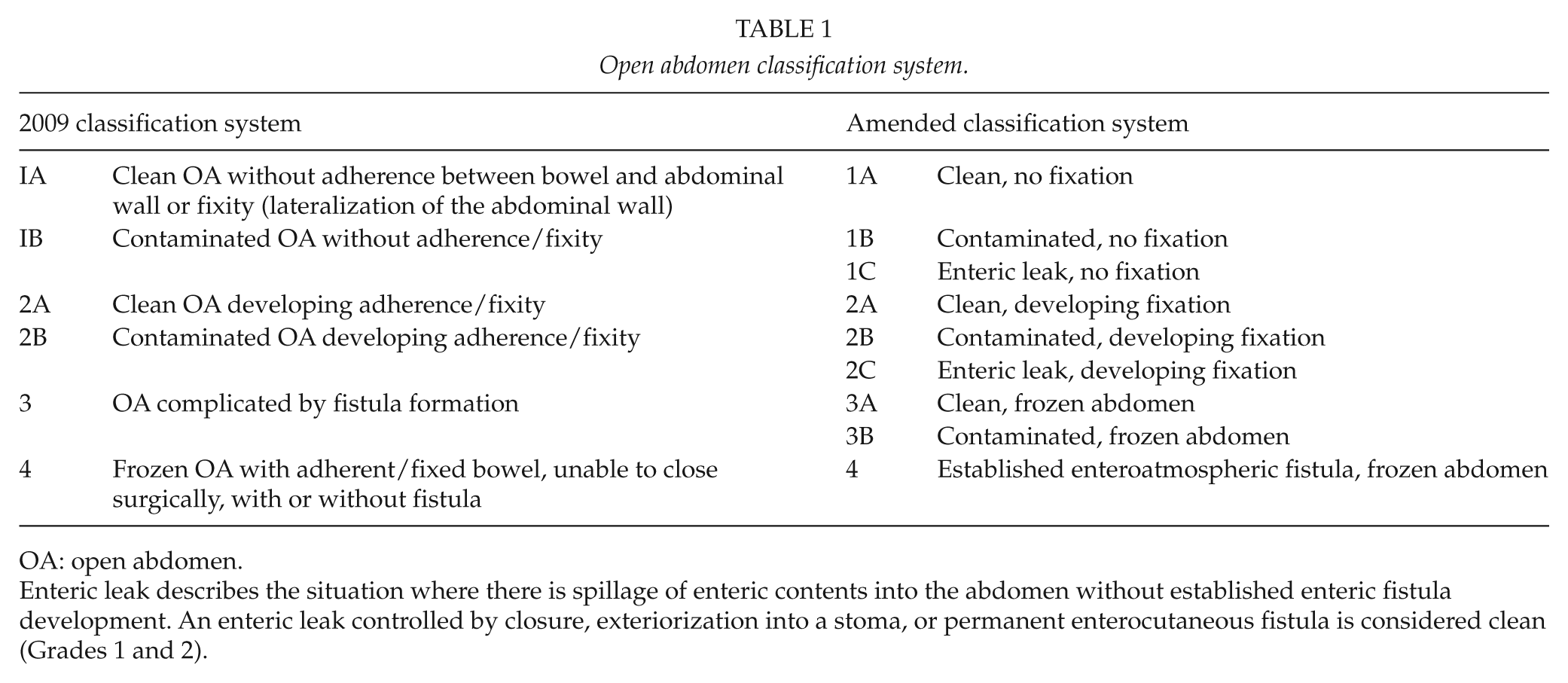
OA: open abdomen.
Applying the Classification System
Although the classification system was published recently, it has already been used in several publications reporting experiences of different types of cohorts of patients treated with OA. Among those, 12 were review articles discussing problems related to IAH/ACS and OA treatment (5–16).
Nine cohort studies with a total of 542 patients (mean: 60, range: 9–160) classified their patients according to the 2009 Björck classification system (17 –25), and they were reviewed as part of the classification revision process. The remaining eight articles were animal research, correspondence, and one case report.
A classification system should be able to adequately and reproducibly characterize the complexity of the OA, in which there are two major aspects to cover. First, the mechanical properties of the abdomen: Adhesions between the abdominal wall and contents and the fixity of the abdominal wall, both precluding movement toward the mid-line. Second is the degree of contamination, as well as the possibility to control it. Ideally, the classification system should characterize the complexity of the whole situation, taking both these aspects into consideration, and a higher grade should be associated with a more adverse outcome. It is also important that every patient can be classified at all times.
The classification system can also be used as a guideline for the management of the OA. Prevention of deterioration of the grade is important and should be avoided. In addition, the system can be used to emphasize the need for early closure in order to prevent a more complex grade with higher risk of complications.
Thus, the classification must be practical to use both in teaching and in science. Those are rather tough requirements, and no one is surprised that we are experiencing some difficulties trying to define the most optimal classification system. Like most of science, the current revision should be regarded as a refinement since there is no fundamental change.
Seternes et al. (17) and Padolini et al. (18) were the first investigators to apply the classification system on two small cohorts each with nine patients requiring OA treatment. Acosta et al. (19) published the first experience trying to apply a classification system in a large prospective cohort of OA patients treated using a previously described system of vacuum and mesh-mediated traction. This method combines negative topical pressure and plastic layer to prevent adhesions to form between the bowel wall and the intestines (V.A.C. Abdominal Dressing System; KCI, San Antonio, Texas, USA) with mesh-mediated fascial traction to prevent lateralization of the bowel wall (26). Among 111 patients included in the study, 67 (60.4%) were classified using the original Björck system (3) as Grade 1A, 42 (37.8%) as Grade 1B, and one patient each (0.9%) were classified as 2A and 3. During the course of treatment, the highest grade recorded was 1A in 53 patients (47.7%). Thus, approximately half the patients had a clean and OA throughout the treatment period, and as could be expected those patients were closed without any complications. In 32 patients (28.8%), however, Grade 1B developed as the most serious grading during the course of treatment, and three had 2A abdomens. Regarding the most severe cases, fistulae were present in 15 (13.5%) and 8 (7.2%) developed a Grade 4, frozen abdomen. At the end of treatment (i.e. abdominal closure or death) 75% were Grades 1A, 8% 1B, 3% 2A, 7% 3, and 7% Grade 4. In validity and reliability analysis, Bjarnason et al. (27) showed that the Björck classification system from 2009 showed good correlation with worse clinical outcomes, and that the inter-rater and test–retest reliabilities were good.
The most serious classification problem was encountered among those who had some kind of leakage or fistula. Only 8 of the 15 patients had a true enteroatmospheric fistula (EAF), a chronic situation with granulation. The other seven patients experienced urinary or pancreatic fistula, bile leakage from a hepatojejunostomy or a gastrostomy, or leakage of stool from a staple line, a result of ischemia of the rectal stump. The overall classification was prognostic for outcome. The grade of the OA at the end of treatment was associated with failure of fascial closure and in-hospital mortality (both p < 0.001). A change to a worse OA grade and the highest OA grade recorded in each patient were associated with failure of fascial closure (both p < 0.001) and with in-hospital mortality (p = 0.002 and p = 0.007). Rasilainen et al. (24) used the classification system when comparing the results of treating 50 patients with vacuum and mesh-mediated traction, with a cohort of 54 historical controls. The two cohorts were almost identical in their pretreatment classification (72–74% Grade 1A, 26–26% Grade 1B, and 0–2% Grade 2B), thus strengthening the conclusions of the study.
Kafka-Ritsch et al. (22) reported on 160 patients treated with OA, mainly due to abdominal sepsis (78%). They used a similar technique combining negative pressure wound therapy with dynamic retention sutures preventing lateralization and had similar results, 87% closure rate among survivors. The grading according to the Björck classification correlated strongly with the primary delayed fascial closure rate (p = 0.002).
Navsaria et al. (25) used the classification system in a prospective study evaluating a newly developed OA treatment system (RENASYS AB Smith and Nephew). The 20 trauma patients all had OA Grade 1 or 2 at the start of OA treatment.
Revision of the Classification System
As an integral part of the World Society of the Abdominal Compartment Syndrome (WSACS) review of the literature and update of their proposed 2006 consensus definitions and 2007 management statements, the need of a classification system of the OA was confirmed (28). The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system for clinical practice guidelines developers was used (29, 30) to provide consistency in identifying and rating the quality of available evidence, and the strength of management recommendations (31). The present classification system was published in an identical form as part of the updated consensus definitions and clinical practice guidelines from the WSACS (28). However, in order to emphasize the differences of the amended classification system, highlight the rationale for the amendments, and improve the relative poor adherence to the classification system noted in the literature, the authors felt that it is important to republish the amended classification system in a specific and concise form.
When the classification system (3) was reviewed, two problems were verified: The aforementioned definition of fistula or EAF, and the fact that the system graded a frozen clean abdomen as a more serious condition (Grade 4) than the established EAF in an OA, which is a highly lethal condition. A sub-group of the working group of the WSACS updated consensus definitions and clinical practice guidelines was created to amend the classification system, that is, the authors of this article, and reached the consensus described in Table 1.
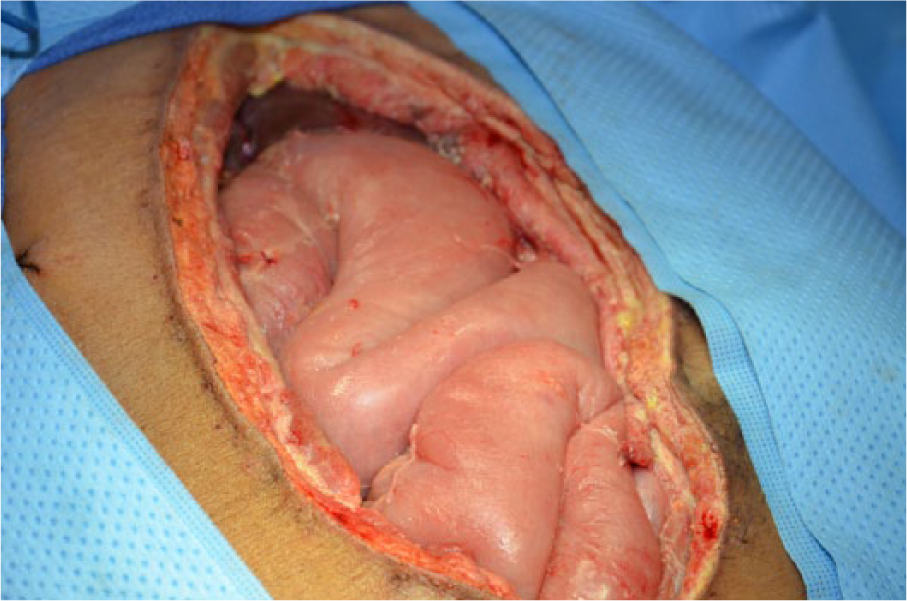
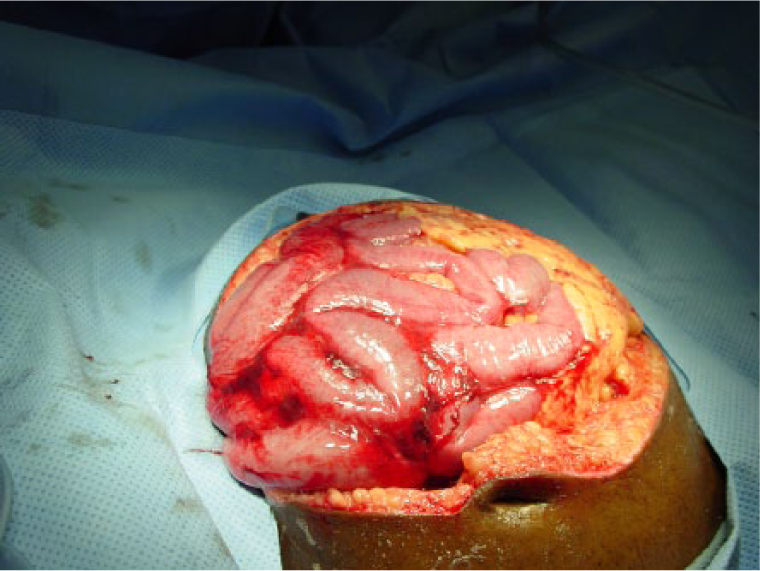
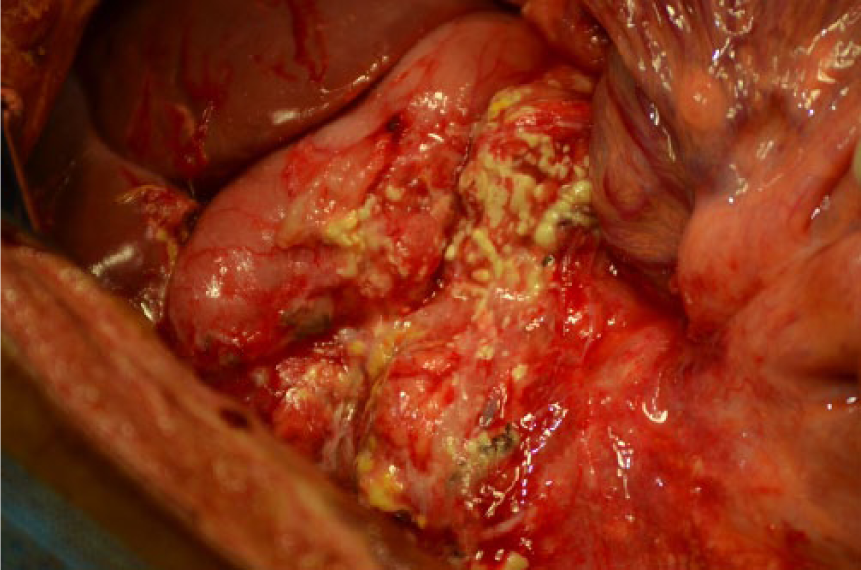
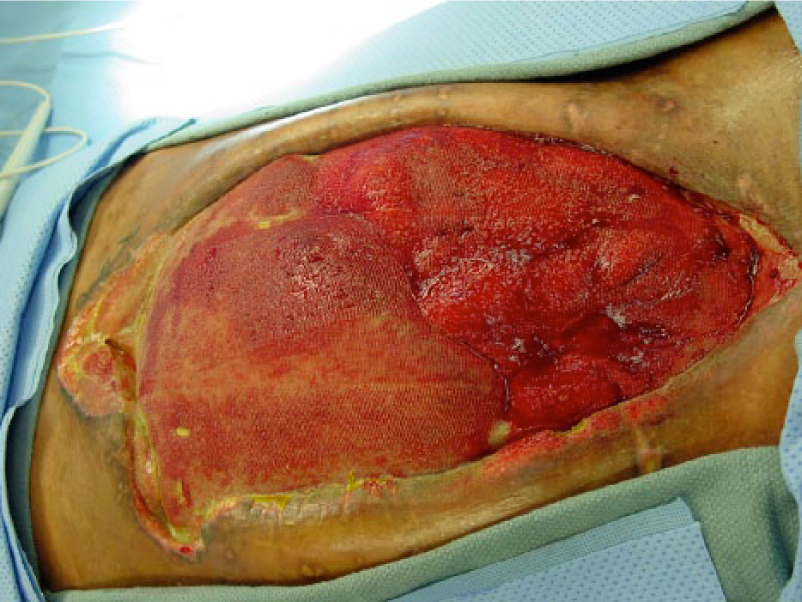
When comparing both classifications in Table 1, the reader will find that both the identified problems have been addressed in the amended classification system. An enteric leak (Grades 1C or 2C) has been separated from an established EAF (Grade 4), and the frozen abdomen (Grades 3A or B, clean or contaminated) without EAF has been separated from the more serious condition of an established EAF. A formal definition of EAF was also added: a permanent enteric leak embedded in granulation tissue. It is important to distinguish this critical situation from the situation when an enteric leak that is controlled by closure, exteriorization into a stoma, or if the patient has a permanent enterocutaneous fistula, which can be drained in a controlled way. The devastating effect of an EAF in an OA is explained by the difficulties to achieve source control, often resulting in sepsis and death. In Fig. 1A–4, the different grades are exemplified. The pictures (Grades 1–3) were supplied by Mark Kaplan, and are from patients treated at Albert Einstein Medical Center, Philadelphia, Pennsylvania, USA.
As was pointed out in the previous classification system (3), it must be remembered that the focus is the patient, not the abdomen. Nutrition, ambulation, mental health, control of infection, and inflammatory reaction are all important for the prognosis of the OA. Early enteral nutrition is beneficial (32). When evaluating different temporary abdominal closure devices, these issues should also be addressed and reported appropriately.





Conclusion
In summary, with these rather small changes, we believe that the requirements on a functional and dynamic classification system, useful in both research and training, will be fulfilled. We encourage future investigators to apply the system and report on its merits and constraints.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The World Society of the Abdominal Compartment Syndrome supported the process leading to this publication (website: ![]() ). M Björck’s institution received an unrestricted (unconditional) research grant from Kinetic Concepts Incorporated (KCI) in 2006 and has received speaker’s honorarium from KCI. A W Kirkpatrick’s institution received an unrestricted grant from the KCI to conduct a prospective randomized trial of Open Abdomen management (ClinicalTrials.gov Identifier: NCT01355094). M Cheatham’s institution received an unrestricted grant from the KCI to conduct a prospective observation trial of open abdomen management (ClinicalTrials.gov Identifier: NCT01016353). M Kaplan has received consultant and speakers honorariums from the KCI. A Leppäniemi, no disclosures. J J De Waele performed consultancies for both KCI and Smith and Nephew, suppliers of open abdomen devices.
). M Björck’s institution received an unrestricted (unconditional) research grant from Kinetic Concepts Incorporated (KCI) in 2006 and has received speaker’s honorarium from KCI. A W Kirkpatrick’s institution received an unrestricted grant from the KCI to conduct a prospective randomized trial of Open Abdomen management (ClinicalTrials.gov Identifier: NCT01355094). M Cheatham’s institution received an unrestricted grant from the KCI to conduct a prospective observation trial of open abdomen management (ClinicalTrials.gov Identifier: NCT01016353). M Kaplan has received consultant and speakers honorariums from the KCI. A Leppäniemi, no disclosures. J J De Waele performed consultancies for both KCI and Smith and Nephew, suppliers of open abdomen devices.