
Abstract
Background:
Intraoperative testing of gastrointestinal anastomosis effectively ensures anastomotic integrity. This study investigated whether the routine use of methylene blue intraoperatively identified leaks to reduce the postoperative proportion of clinical leaks.
Methods:
This study retrospectively analyzed consecutive total gastrectomies performed from January 2007 to December 2014 in a university hospital setting by a general surgical group that exclusively used the methylene blue test. All surgeries were performed for gastric or junctional cancers (n = 198). All reconstructions (Roux-en Y esophagojejunostomy) were performed using a stapler. The methylene blue test was used in 108 cases (group 1) via a nasojejunal tube. No test was performed for the other 90 cases (group 2). Intraoperative leakage rate, postoperative clinical leakage rate, length of hospitalization, and mortality rate were the outcome measures.
Results:
The intraoperative leakage rate was 7.4% in group 1. The postoperative clinical leakage rate was 8.6%. The postoperative clinical leakage rate was 3.7% in group 1 and 14.4% in group 2 (p = 0.007). There were no postoperative clinical leaks when an intraoperative leak led to concomitant intraoperative repair. The median length of hospital stay was 6 days in group 1 and 8 days in group 2 (p < 0.001). One death occurred in each group. No test-related complications were observed.
Conclusion:
The methylene blue test for esophagojejunostomy is a safe and reliable method for the assessment of anastomosis integrity, especially in cases with difficult esophagojejunostomic construction.
Introduction
Gastric cancer is frequently observed worldwide. In particular, the incidence of cancers originating from the proximal part of the stomach and cardia is increasing (1, 2). The fundamental option for cure is based on the surgical removal of all cancer foci. Total gastrectomy (TG) and dissection of lymph nodes are widely used to achieve this outcome. The most encountered and most feared complication of TG is anastomotic leak. The reported incidence of leakage from Roux-en-Y esophagojejunostomies (REJs) after TG for cancer ranges from 0% to 15.8% in the literature (3–7). The development of automatic suturing devices markedly reduced leaks from REJ, but anastomotic leakage remains a serious complication (8–10). An effective method to address anastomotic leakage during surgery is lacking. The methylene blue test is traditionally used to control for the anastomotic integrity of REJ, but there is no published study on this topic to our knowledge. Most studies that investigated the use of methylene blue or other techniques to examine anastomosis integrity during surgery were conducted during colorectal surgery, gastric bypass surgery, and bariatric surgery (11–14). However, the most cost-effective method to ensure and protect anastomosis integrity is not known. We hypothesized that the use of methylene blue intraoperatively to test anastomosis integrity would identify leaks that could be mended to reduce the postoperative proportion of clinical leakages.
Patients/Methods
Design
We performed a retrospective review of consecutive REJs from data collected in a prospective manner from January 2007 to December 2014. All REJ surgeries were performed for gastric cancers and cancers located at the esophagogastric junction by one surgical group. This group has exclusively used methylene blue to test anastomosis integrity in a referral university hospital since 2000, and this group uses a 25-mm or 28-mm circular stapler (Covidien Ilc, Mansfield, MA, USA) for all REJs for anastomosing. No further tests or interventions were performed after end-to-side anastomosis if no problems arose, and the surgery was performed on Monday or Tuesday. However, tests were performed if any conflict existed regarding the anastomosis integrity (e.g. incomplete doughnuts or other technical difficulties) or the surgery was performed on Wednesday or Friday. Surgery day was entirely dependent on the completion of preoperative work-ups. No surgeries were performed on Thursday at our institution because Thursdays are education and seminar days. Most tests were performed because of the surgery day (Wednesday or Friday) rather than technical problems, which resulted in a random allocation of cases. Patients were classified into two groups based on methylene blue test status: group 1 included cases in which the test was performed, and group 2 included cases in which the test was not performed.
The following inclusion criteria were used: patients who underwent TG for gastric cancer and REJ between 2007 and 2014, and patients whose surgical and demographic data were reported and reliable. Subtotal gastrectomies that included an esophagogastrostomy or gastrojejunostomy were excluded. And total gastrectomies with additional organ resections (two cases: one non-anatomic hepatic resection and one splenectomy) were excluded. Basic demographic details, surgical details, and surgical results were collected. We defined an intraoperative leak as visualization of methylene blue on a gauze pad wrapped around the REJ or obvious visual leakage from anastomoses (Fig. 1). Postoperative clinical leakages were defined in accordance with the definition proposed by the UK Surgical Infection Study Group (SISG) (15). Therefore, an anastomotic leak was considered when the patient presented fever, abdominal pain, leukocytosis, an elevation of C-reactive protein (CRP), and leakage on radiographs (e.g. water-soluble contrast solution passage graphs or computed tomography) or drainage of intestinal contents from the surgical site or drains that were placed during surgery. Drains were removed if no evidence of anastomosis leaks was observed by X-ray and the patient began liquid feeding.
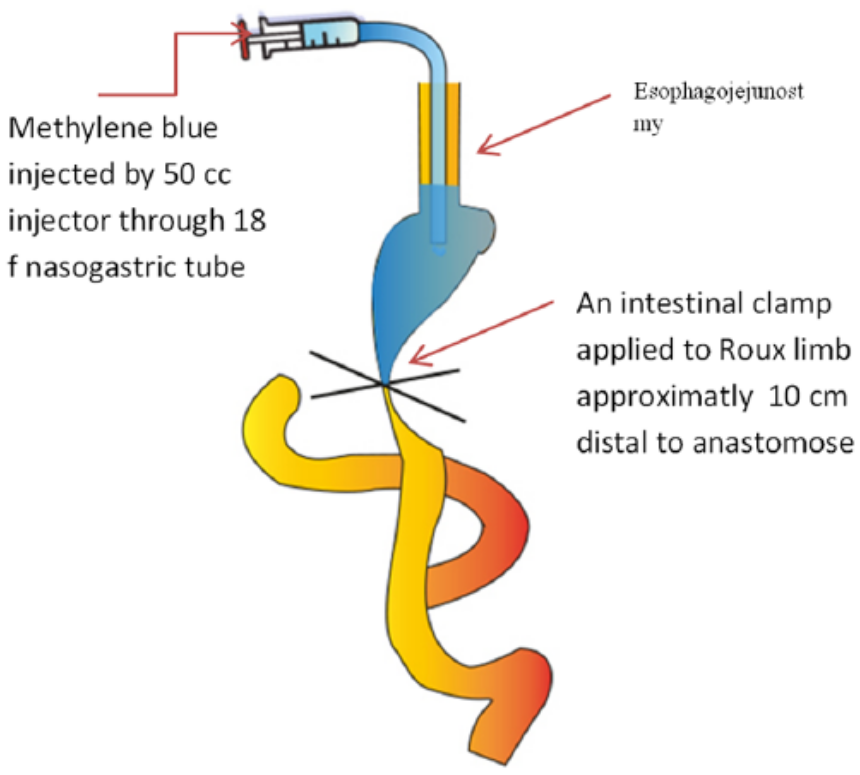
Schematic representation of technical method of methylene blue test.
We routinely used a green-colored naso-esophagojejunal suction tube until postoperative day 2. The suction tube was removed before X-ray examination. Tube removal was not coordinated with postoperative X-ray anastomosis examination.
Radiologically diagnosed postoperative leakage (which were routinely performed using passage graphs on postoperative day 3 or 4) with no clinical symptoms was defined as subclinical leakage (SCL). All files were evaluated for up to 30 postoperative days.
The primary endpoints were intraoperative and postoperative clinical leakage. Length of stay (LOS) in the hospital and hospital mortality related to anastomosis were our secondary endpoints.
Methylene Blue Test Technique
The required materials for this method include a nasojejunal tube (of any size, but we generally prefer 18F), a 50-cm3 tipped pine injector and 500 mL of normal saline containing 5 mL of methylene blue dye (final concentration of 0.01%). The nasojejunal tube was inserted after anastomosis completion and placed approximately 2–3 cm distal to the anastomosis line. The anastomosis was surrounded with clean sponges and an intestinal clamp that was applied to the Roux limb approximately 10 cm distal to the anastomosis. The occluded part of the intestine was filled with the methylene blue solution. The injector was removed when the surgeon was satisfied with the anastomotic integrity, and the nasojejunal tube was lowered to a waste container to allow gravity drainage. This application was repeated multiple times as needed (Fig. 1). An objective finding of leakage was obtained if any blue dye was observed on the sponges wrapped around the anastomosis, and the leakage area was strengthened with full-thickness simple suture and reinforced with Lembert sutures. The methylene blue test was repeated to verify the successful repair and water tightness of the anastomosis before the surgery was completed.
Statistical Analyses
All statistical analyses were performed using the SPSS program (IBM SPSS Statistics for Windows, Version 20.0; IBM Corp., Armonk, NY, USA). Normally distributed continuous variables are reported as the means and standard deviation, and results were compared between two groups using independent t-tests. Non-normally distributed variables are reported as medians and minimum–maximum ranges, and the results were analyzed using the Mann–Whitney U-test. Leakage rates were analyzed as frequency tables and percentages. Proportions were analyzed using the Chi-square test or Fisher’s exact test when appropriate. A p-value less than 0.05 was considered statistically significant.
Results
A total of 198 patients underwent TG and REJ for gastric or junction cancers from January 2007 through December 2014. A total of 133 of the 198 cases were in the cardia (including junction tumors), 55 cases were in the fundus, and 10 cases were in the antrum that had invaded the entire gastric wall, and TG was applied. A total of 100 cases were male, and 98 cases were female. Table 1 lists patient demographics and some tumor characteristics. Table 1 shows that there were no significant differences in demographics or tumor characteristics between group 1 (test performed group) and group 2 (test not performed group).
Demographics and tumor characteristics of patients according to whether methylene test was performed or not.
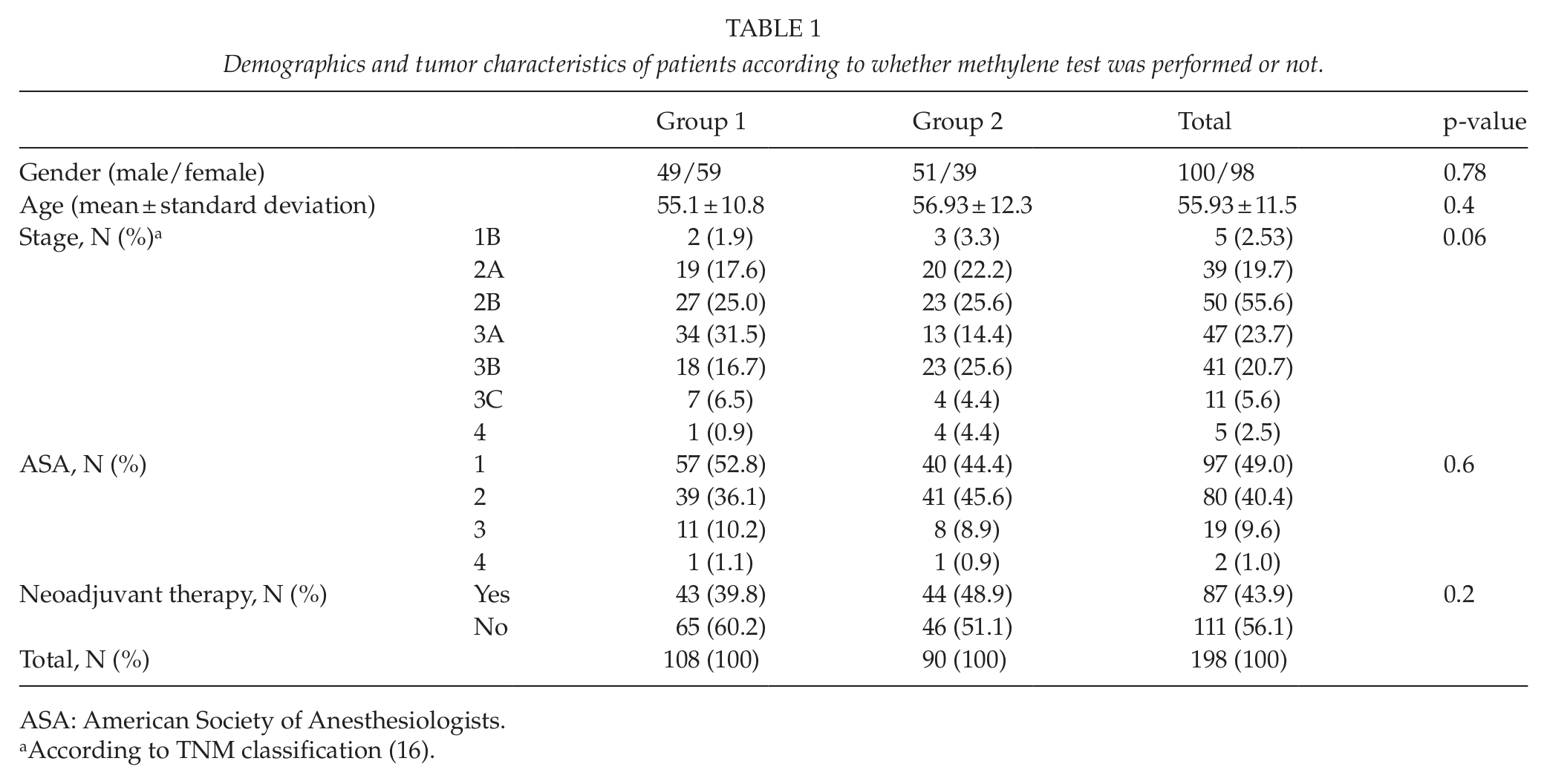
ASA: American Society of Anesthesiologists.
According to TNM classification (16).
Intraoperative Findings
Fig. 2 shows that 108 cases intraoperatively underwent the methylene test and 90 cases were never tested because of operation day, and in addition, they did not have any technical concerns. Of all the 108 patients tested, 98 were due to day of operation and merely 10 (5.1%) due to additional technical difficulties. The following technical difficulties were observed: issues with doughnuts (a fully incomplete ring after dividing the locking suture or complete ring but lacking full wall thickness (n = 5)); tears in esophageal musculature or mucosal tissue when performing purse-string sutures or during anvil placement (n = 2); short esophagus (intra-thoracic anastomosis, n = 2); and greater resistance during stapler firing, likely because of the wall thickness of the distal esophagus or stapler dysfunction (n = 1). Intraoperative leakage occurred in 8 of the 108 tested cases (7.4%). Five of these eight cases had technical difficulties during anastomosis. All eight leaks occurred in the posterior or posterolateral part of the anastomosis. Reinforcement sutures were used in these cases as mentioned above. The leak test was repeated (once for all cases) after reinforcement sutures were placed in the eight identified intraoperative leaks, and no leaks were identified during the second check. A drain was placed near to the anastomosed region in all cases (tested or not tested groups). There were no complications due to methylene blue during or after surgery.
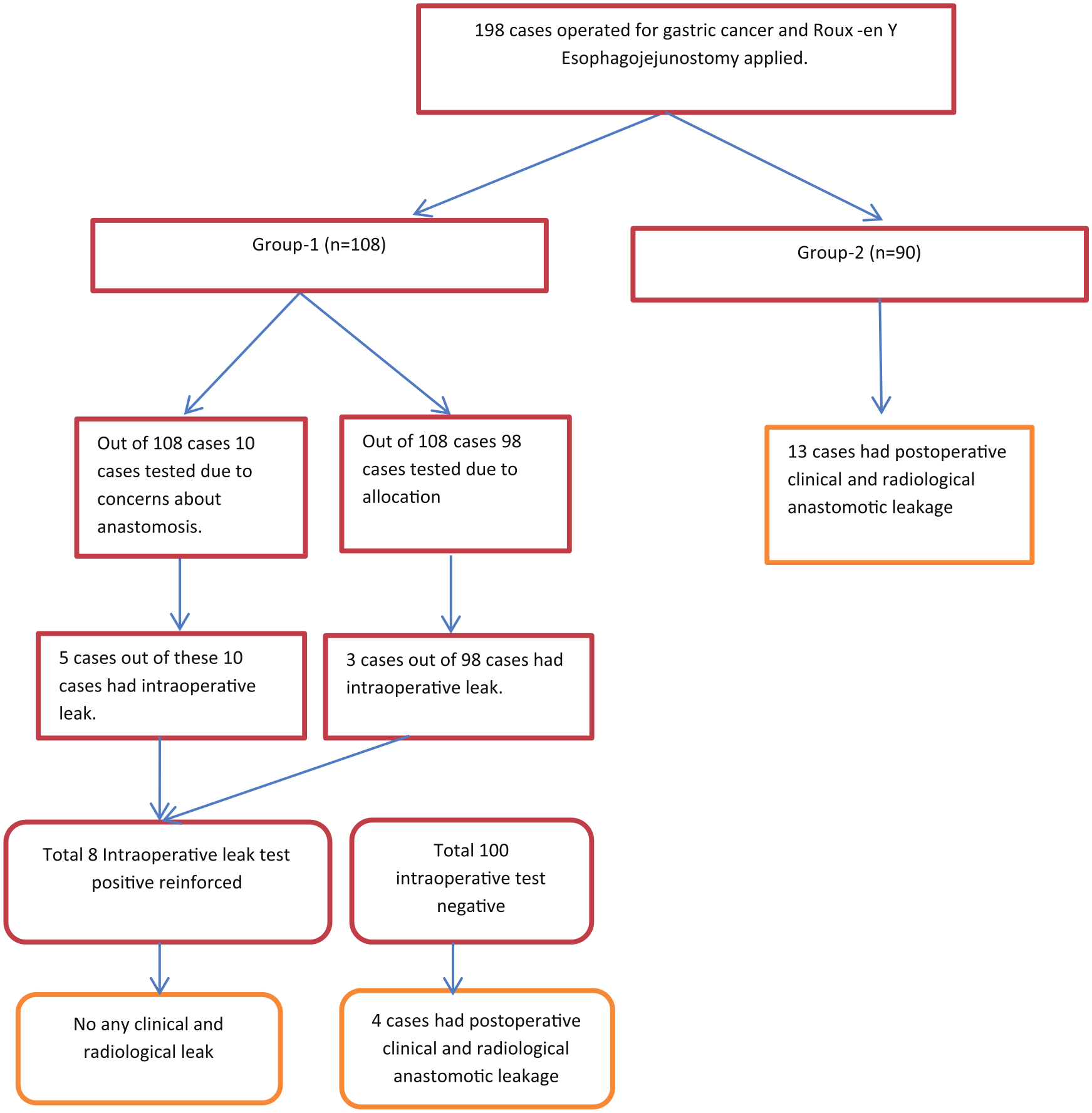
Schematic representation of study protocol and results.
Postoperative Outcomes
Four (3.7%) cases had clinical leakage in group 1 (the intraoperative methylene blue test failed to detect any defects), and 13 (14.4%) cases had clinical leakage in group 2 (p = 0.007). The pretest probability of a leak being identified in cases in our study with a technically complicated anastomosis was significantly greater (5/10 vs 3/98) than that of uncomplicated anastomoses. Therefore, a comparison of only patients with technically uncomplicated anastomoses (13/90 vs 4/98) revealed a significant difference (p = 0.013). The use of methylene blue to assess intraoperative leaks was associated with a lower postoperative leak rate, which was likely due to identification and repair.
One case with clinical leakage in group 1 died. The other three clinical leakage cases were hospitalized for a mean of 19 days. One case was discharged with a catheter for intra-abdominal abscess, and the other two cases were discharged without issues.
The following prognosis was observed in cases with clinical leakage (13 cases) in group 2: 1 case died, and the other 12 cases were hospitalized for an average of 23.8 days. Out of these 12 cases, 6 were discharged with a drain or catheter, and the other 6 cases were discharged without problems.
A total of 17 clinical leakages were observed (8.6%), and no reoperation was performed. Eight patients received indwelling drains, and one of these cases died. Seven patients required percutaneous interventions. Two patients were handled only using a controlled fistula, and one of these cases died. Fever and CRP elevation were alarming signs of leakage.
Patients in both groups who were diagnosed with clinical leakage were fed central total parenteral nutrition (TPN) until they could take oral feeding. Both groups took proper antibiotics and had proper interventions, if needed, for any collections or for abscesses.
Radiological leakage considered SCL was only observed in three cases. Two of these three cases were in group 1, and one case was in group 2. These three cases were uneventfully discharged.
No patients, except for patients with clinical anastomotic leakage, died postoperatively. Postoperative mortality (30-day follow-up, in hospital) was observed in two cases (1%): one case was in group 1 and the other was in group 2. The case in group 1 was a 50-year-old female who was diagnosed with abdominal sepsis and died on postoperative day 24. The case in group 2 was a 68-year-old female. This case was diagnosed with anastomotic leakage and controlled fistula on postoperative day 8. She died on postoperative day 30 due to myocardial infarction.
The median LOS for all patients was 8 days in group 2 (minimum: 5 days and maximum: 36 days) and 6 days in group 1 (minimum: 4 days and maximum: 26 days) (p < 0.001). However, the LOS was 19 days for the cases with a leak in group 1 versus 23.8 days for cases in group 2, but this difference was not significant (p = 1.00).
Discussion and Conclusion
There is a wide range of reported anastomotic leakage rates of esophagojejunostomy in the literature, but there is consistent agreement on the importance of the technical aspect of anastomosis (5, 7, 9). The technical evolution from hand-sewing to the use of stapler devices is accepted and implemented worldwide. These techniques decrease leaks from REJ (17), but technical errors are a major risk factor for leakage from esophagojejunostomy (5, 6). Our study detected intraoperative leaks using the methylene blue test in 50% of cases who had technical or surgical concerns for anastomosis, which is similar to previous studies. Therefore, we think that intraoperatively testing anastomosis is very important, especially when problems are encountered during anastomosis. Three patients had no technical issues (3/98) with anastomosis but had a positive intraoperative leak test. This finding was important because these patients were “saved” by the leak test, and these patients would likely have gotten sick because the leak would have been missed if the leak test was not performed. Three studies on the technical approaches examined esophagojejunostomy anastomosis integrity intraoperatively in the literature (Table 2). Two of these studies used intraoperative endoscopy (IOE) and the air test, and the other study used the air test via a nasojejunal tube, and the air test was safe and reliable (14, 18, 19). The air–water test cannot delineate the exact focus of the leakage but the quadrant of leakage. Kanaji et al. (19) recently reported that the postoperative leakage rate was 4.9%, despite the use of the air–water test in all cases. The air–water test is easier to perform and is perhaps the more prevailing method. However, the use of the air–water test alone without endoscopy is not sufficiently precise. It is not always easy to find endoscopy equipment in operating rooms, and it is not easy to find an experienced endoscopist, as reported in Nishikawa et al., in which IOE was not performed in eight patients because of the lack of an endoscope or an endoscopist. In contrast, our study used the methylene blue test in all patients easily, quickly, and safely when needed.
Current studies that evaluate esophagojejunostomy anastomosis integrity intraoperatively.
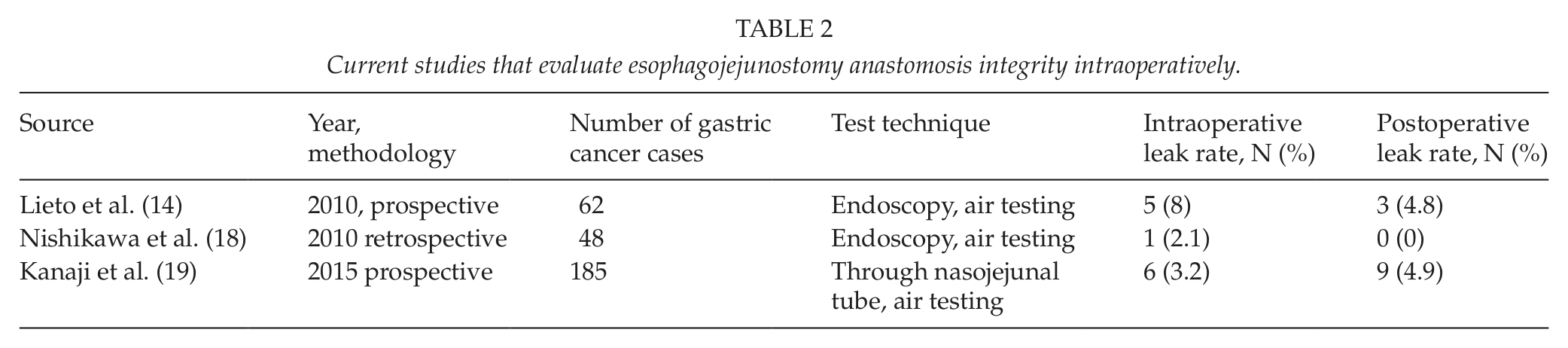
The systematic review of Bruce et al. (20) reported a lack of consensus on what exactly defined an anastomotic leak in the literature. A UK multidisciplinary group (SISG) (15) proposed a standard definition for anastomotic leakage, which was used in our study, but this definition was not used or referred to in the mentioned studies. Therefore, the lack of leaks in the studies of Lieto et al. and Nishikawa et al. is questionable. Nevertheless, the use of the methylene blue test significantly reduced the leakage rate in our experience, and the leakage rate (3.7%) in the tested group was similar to previous studies (14, 18).
Smith et al. (11) performed an important study on the methylene blue test and determined the efficacy of methylene blue enemas as an intraoperative test in colonic anastomosis. Smith et al. indicated that the methylene blue test was flawless in the prevention of postoperative leaks in a patient with an intraoperative leak, which is consistent with our results. However, a negative result on the methylene blue test does not guarantee that a postoperative leak will not follow. Many factors potentially affect the postoperative leakage rate (e.g. patient factors, sufficient blood supply, and anastomotic tension). Therefore, it may be impossible to predict leakage using the methylene blue test alone. The methylene blue test alone was not sufficient to prevent postoperative leaks, which was demonstrated in our four patients who underwent a methylene blue test and had postoperative clinical leakage.
The location of the leakage area of the anastomosis, which was somewhat problematic when tested using the air–water test, was precisely detected on the gauze that was wrapped around the anastomosis during the methylene blue test. A little blue staining on the gauze was sufficient to locate and reinforce the leakage area. Another important consequence of the test was the LOS, which was shorter in group 1 compared to all patients. However, LOS was the same in both groups in cases with leak. This result may be that physicians made discharge decisions more easily and more comfortably with the tested group. This subjective decision may have shortened the hospitalization period in group 1.
This study had limitations because it was not a randomized controlled study. Patients were allocated according to surgery day using a non-randomized intervention study, but this was not a proper randomization. There was also a substantial crossing over because “troublesome anastomoses” were tested regardless of calendar day. A prospective study comparing other intraoperative testing techniques with the methylene blue test would provide more powerful evidence on gastrointestinal anastomosis integrity. We are planning a prospective study with at least 145 patients per group (statistical power 80% with a 95% confidence interval) that compares a tested group with a not tested group.
Consequently, the results from this study suggest that intraoperative methylene blue test might be associated with fewer leaks, and it can be used to check esophagojejunostomy anastomoses. However, it is important to be aware that a negative test does not definitely exclude all potential problems.
Footnotes
Acknowledgements
We thank Prof. Dr M. Çetin Kotan for his supervision and intellectual support during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Standards
Written informed consent was obtained from all patients. The study was conducted in accordance with the Helsinki Declaration of the World Medical Association (1964) under the approval of the Ethics Committee of Van Training and Research Hospital (number: 2015/5; date: 17 September 2015).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.