
Abstract
Background and Aims:
Associating liver partition and portal vein ligation for staged hepatectomy may increase the possibility of radical resection in the case of liver malignancy. Concerns have been raised about the high morbidity and mortality associated with the procedure, particularly when applied for diagnoses other than colorectal liver metastases. The aim of this study was to analyze the initial experience with associating liver partition and portal vein ligation for staged hepatectomy in cases of non-colorectal liver metastases and primary hepatobiliary malignancies in Scandinavia.
Materials and Methods:
A retrospective analysis of all associating liver partition and portal vein ligation for staged hepatectomy procedures performed at two Swedish university hospitals for non-colorectal liver metastases and primary hepatobiliary malignancies was performed. The primary focus was on the safety of the procedure.
Results and Conclusion:
Ten patients were included: four had hepatocellular cancer, three had intrahepatic cholangiocarcinoma, one had a Klatskin tumor, one had ocular melanoma metastasis, and one had a metastasis from a Wilms’ tumor. All patients completed both operations, and the highest grade of complication (according to the Clavien-Dindo classification) was 3A, which was observed in one patient. No 90-day mortality was observed. Radical resection (R0) was achieved in nine patients, while the resection was R2 in one patient. The low morbidity and mortality observed in this cohort compared with those of earlier reports on associating liver partition and portal vein ligation for staged hepatectomy for diagnoses other than colorectal liver metastases may be related to the selection of patients with limited comorbidity. In addition, procedures other than associating liver partition and portal vein ligation for staged hepatectomy had been avoided in most of the patients. In conclusion, associating liver partition and portal vein ligation for staged hepatectomy can be applied to primary hepatobiliary malignancies and non-colorectal liver metastases with acceptable rates of morbidity and mortality.
Keywords
Introduction
Primary hepatobiliary malignancies, hepatocellular cancer (HCC), intrahepatic cholangiocarcinoma (IHCC), perihilar cholangiocarcinoma (PHCC), and non-colorectal liver metastases (nCRLM) often have a worse prognosis than that for CRLM. This notion holds true particularly for large/many tumors in combination with a small future liver remnant (FLR). Until recently, the only means to increase the possibility of radical (R0) resection without the risk of posthepatectomy liver failure (PHLF) due to a small FLR has been preoperative portal vein embolization (PVE) followed by 4–8 weeks of waiting before resection. This approach is limited by failures of the FLR to grow and disease progression during the interval after the PVE. In 2011, a novel method to increase the volume of the FLR, associating liver partition and portal vein ligation for staged hepatectomy (ALPPS), was presented, and the method was further established in a multicenter report in 2012 (1, 2). The growth in the FLR achieved in one week exceeded that of PVE in 1 month, and the method could potentially eliminate the main disadvantage of conventional methods to increase the volume of the FLR. Unfortunately, the morbidity and mortality levels reported in the initial and some of the subsequent studies exceeded those of the levels associated with PVE (2–6). Furthermore, the high rate of complications and mortality seems to be related to primary hepatobiliary malignancies more than to CRLM (7–9). These findings have caused hesitation concerning ALPPS in settings other than CRLM; thus, the patients with the greatest need for this novel method may not be suitable for treatment. In addition, advanced age has been found to be associated with increased complications, and some authors have suggested limiting the procedure to patients younger than 70 or even 60 years of age (6, 9). The aim of this study was to evaluate the safety and short-intermediate oncological outcomes of initial ALPPS performed for primary hepatobiliary malignancies and nCRLM at two Swedish hepatobiliary centers.
Material and Methods
All ALPPS performed for malignancies other than CRLM at the Karolinska University Hospital, Stockholm, Sweden and the Linköping University Hospital, Linköping, Sweden between October 2012 (the first reported ALPPS in Scandinavia) and the end of April 2015 were included in this retrospective analysis. All included patients were subjected to multidisciplinary evaluation by liver surgeons, radiologists, and oncologists prior to surgery and were found to be non-resectable by conventional means. Some of the patients reported herein have been previously included in a multicenter analysis of the ALPPS registry, and one of the patients has been separately reported (9, 10).
Volumetric analysis was performed on computed tomography (CT) scans or magnetic resonance imagings (MRIs), and the estimated total liver volume (eTLV) was calculated from the body surface area using an established formula (11).
The study was approved by ethical boards in Stockholm and Linköping, and informed consent was not required.
Statistics
Data are presented as the median (range) if nothing else is stated. The statistical analyses were performed using IBM Statistical Package for Social Sciences (SPSS) Statistics version 22 (IBM Corporation, Armonk, NY, USA).
Results
Ten patients, five male and five female, with an average age of 69 years (22–83) were identified. The diagnoses were HCC (4), IHCC (3) and PHCC, metastases from Wilms’ tumor, and metastases from ocular melanoma (1 each) (Table 1). All patients with primary hepatobiliary malignancies had one tumor identified by preoperative radiological work-up, while the patients with metastases from ocular melanoma and Wilms’ tumor had two and four tumors identified on preoperative radiological work-up, respectively. The tumor size was 74 mm (34–140), and no extra hepatic spread was found in any of the patients. Four (40%) of the patients (three with HCC and one with IHCC) had been previously treated with PVE.
Details of 10 patients treated with ALPPS for malignancies other than CRLM.
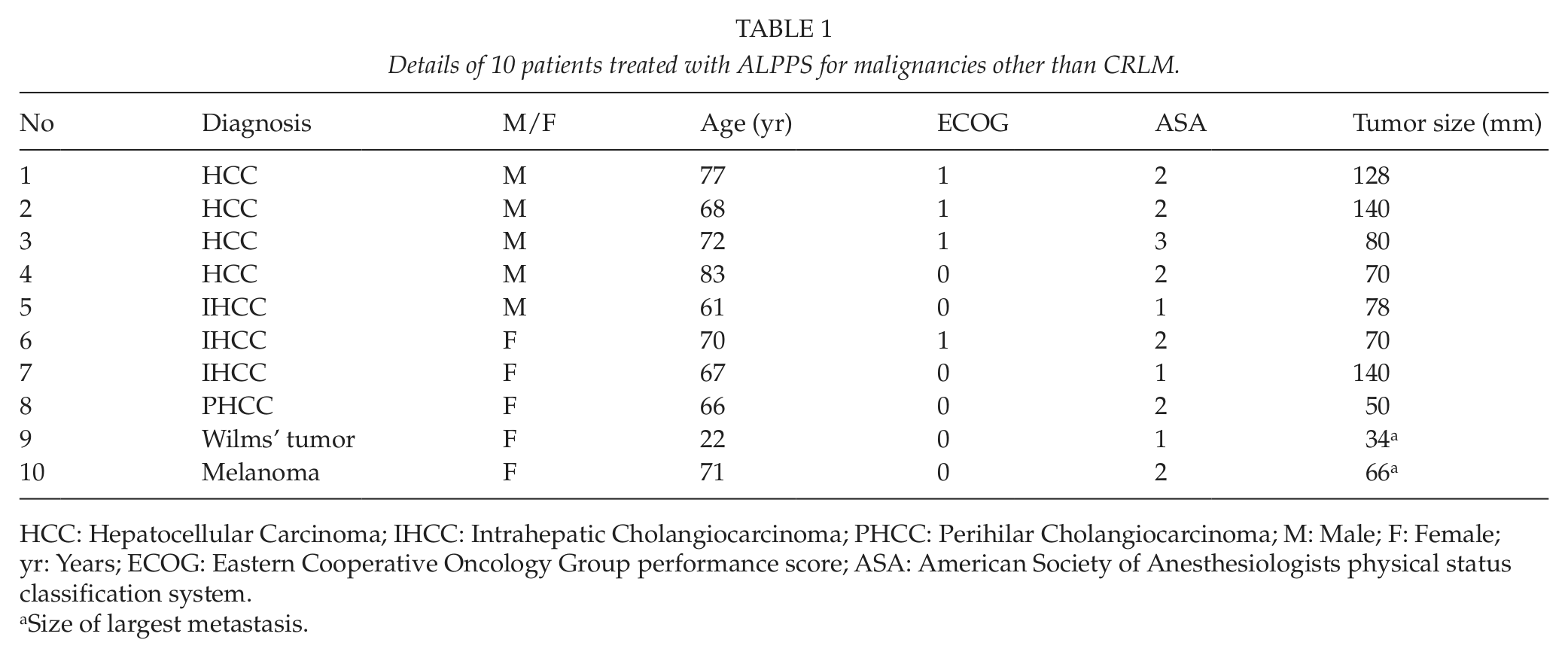
HCC: Hepatocellular Carcinoma; IHCC: Intrahepatic Cholangiocarcinoma; PHCC: Perihilar Cholangiocarcinoma; M: Male; F: Female; yr: Years; ECOG: Eastern Cooperative Oncology Group performance score; ASA: American Society of Anesthesiologists physical status classification system.
Size of largest metastasis.
The preoperative work-up included, in addition to the complete blood count, electrolyte status, and liver function tests, cardiopulmonary testing in three (30%) patients where the physical status was initially considered questionable. The preoperative hemoglobin level was 138 g/L (114–165), the preoperative total bilirubin level was 10 µmol/L (3–20), and the international normalized ratio (INR) was 1.1 (0.9–1.2).
Details of FLR growth are presented in Table 2. One patient with HCC but without signs of cirrhosis had a FLR <40% of eTLV at the time of the stage 2 operation.
Details of the volumetric data for 10 patients treated with ALPPS for malignancies other than CRLM.
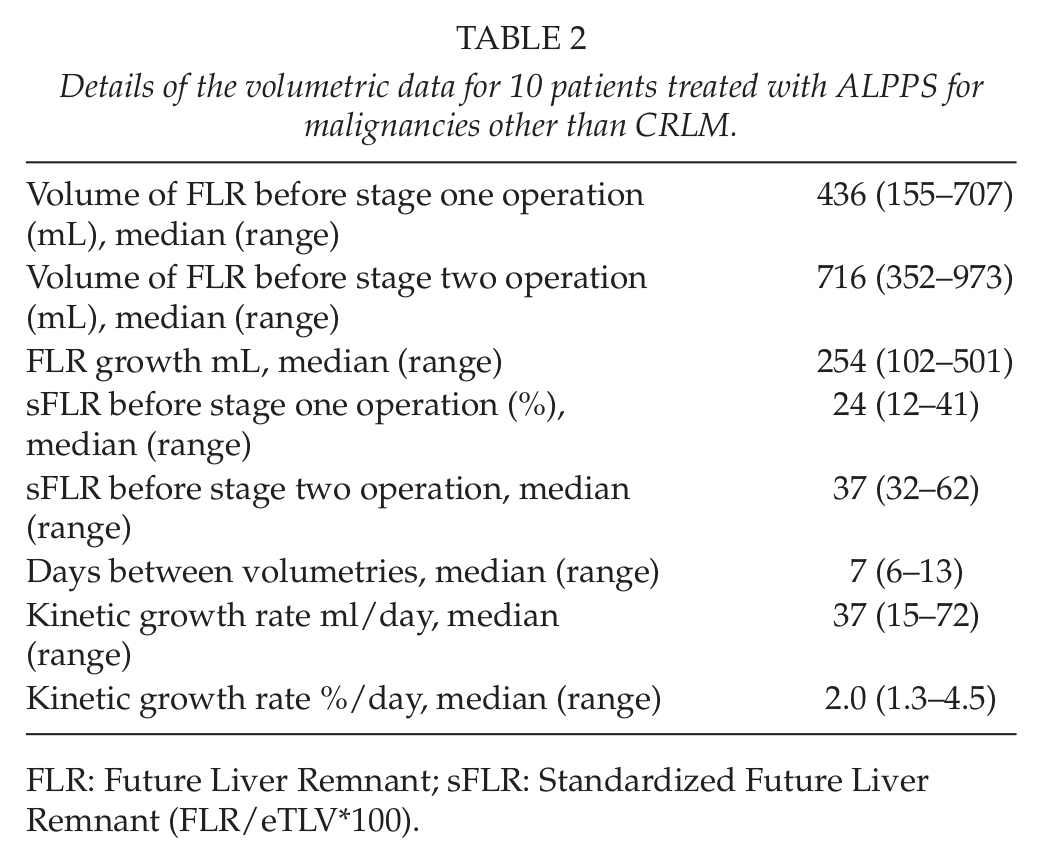
FLR: Future Liver Remnant; sFLR: Standardized Future Liver Remnant (FLR/eTLV*100).
One patient with HCC exceeded the 40% margin recommended for patients with liver cirrhosis before the stage 1 operation (12). Despite normal preoperative liver function tests, because of the small margin and uncertainty about the extent of resection needed, an ALPPS procedure was chosen.
Abdominal drains were placed at the first operation in all patients, and no drains were removed before the stage 2 operation. No additional procedures were performed other than resection in the FLR in one patient. After an interval of 8 days (7–15), a second operation was performed. Hilar lymphadenectomy and resection of the bile duct were performed in two patients who also underwent hepaticojejunostomy, and a small diaphragm resection was performed in one patient during the second operation. Table 3 shows the operative details.
Operative data for 10 patients treated with ALPPS for malignancies other than CRLM.
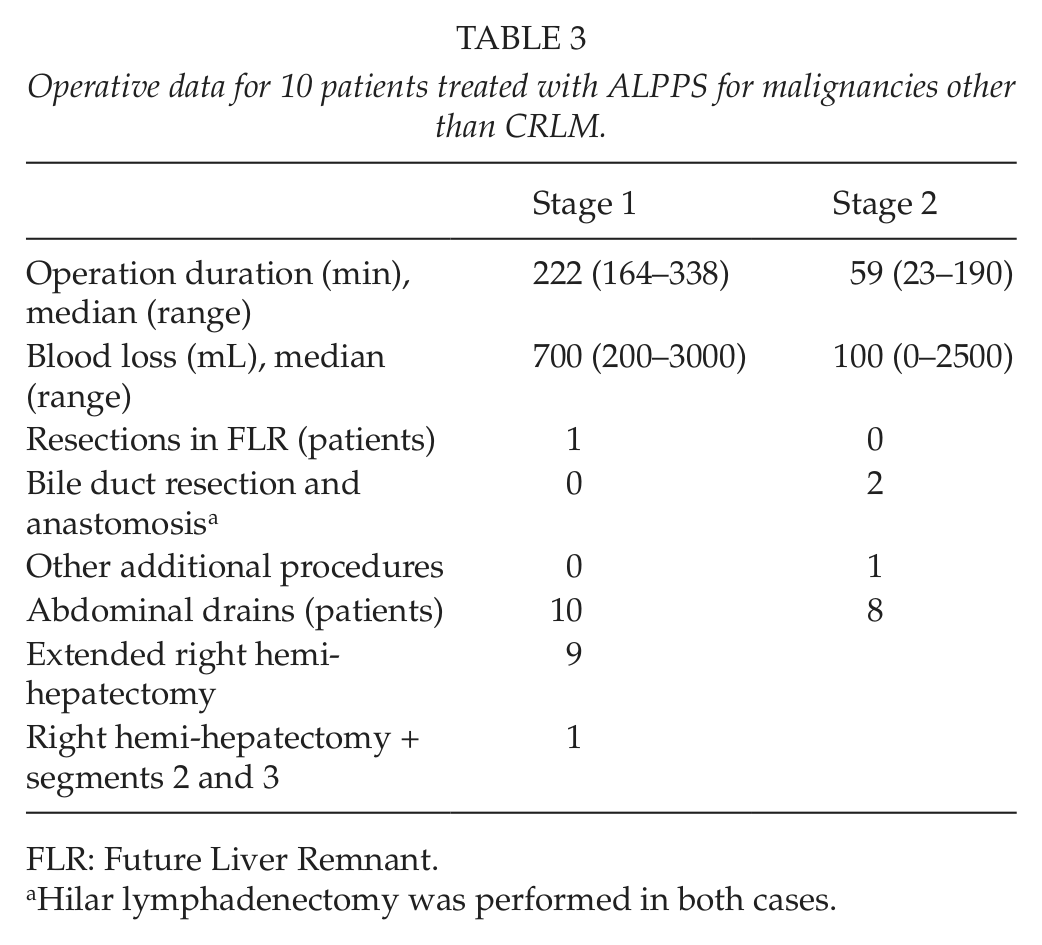
FLR: Future Liver Remnant.
Hilar lymphadenectomy was performed in both cases.
All patients had postoperative complications; six were grade 1 according to the Clavien-Dindo classification, three were grade 2, and one showed pleural effusion requiring percutaneous drainage (grade 3A) (13). No patient had severe complications, that is, grade ⩾3B. The postoperative hospital stay after the stage 2 operation was 13.5 days (5–20). No 90-day mortality occurred.
Nine patients underwent macroscopic radical operation and microscopic radical operation (R0) as well. One patient did not undergo a macroscopic or a microscopic radical operation (R2). The size of the tumors (largest for metastases) according to the final PAD was 80 mm (20–180).
No patient was lost in the follow up; seven are alive, and three are deceased. Table 4 shows the details of the follow-up and recurrent disease.
Details of the follow up of 10 patients who underwent ALPPS for malignancies other than CRLM.
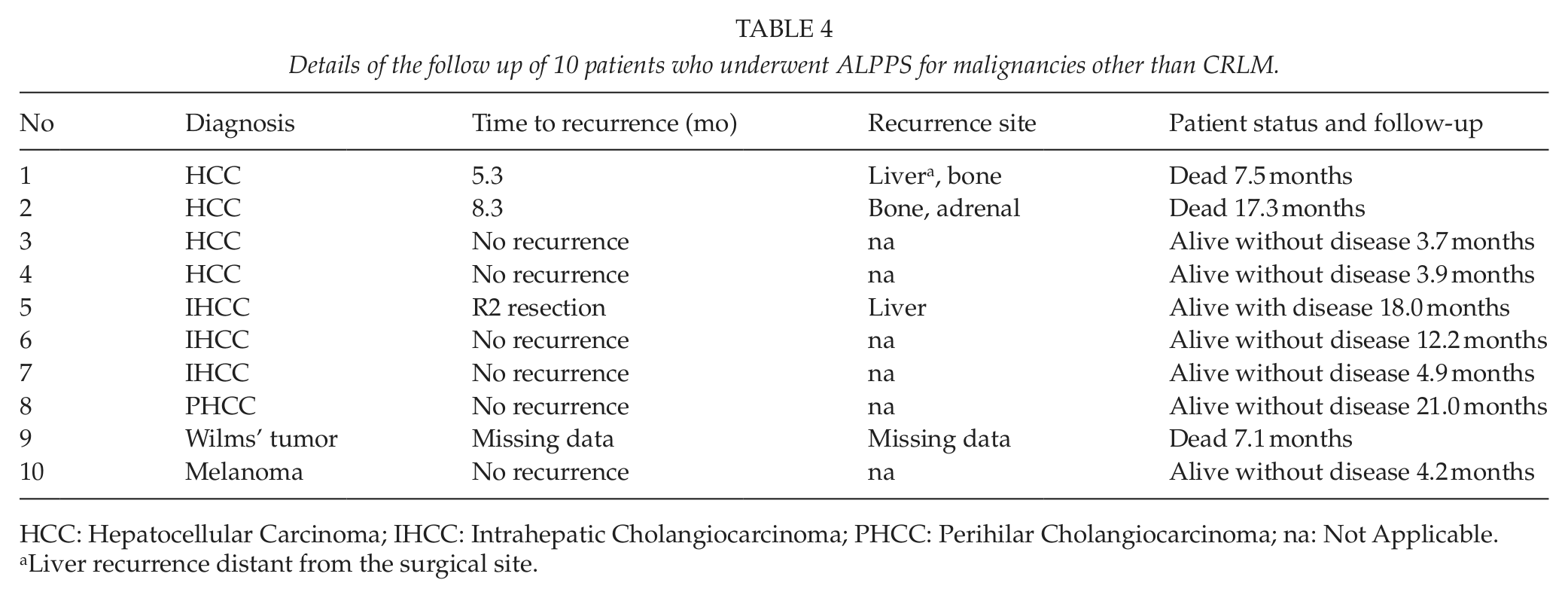
HCC: Hepatocellular Carcinoma; IHCC: Intrahepatic Cholangiocarcinoma; PHCC: Perihilar Cholangiocarcinoma; na: Not Applicable.
Liver recurrence distant from the surgical site.
Discussion
This is the first report on ALPPS to focus solely on malignancies other than CRLM. Contrary to previous reports (3–6, 9, 14), no 90-day mortality was observed in this study. In addition to primary hepatobiliary malignancies, age was suggested in the recent literature on ALPPS as a possible contraindication to the procedure. The current cohort has the highest median age (70 years for primary hepatobiliary malignancies) compared with other reports on ALPPS procedures. Therefore, this simple contraindication does not seem to apply without modifications. However, advanced age liver surgery for CRLM was shown to be safe for carefully selected patients (15). This finding may very well apply to ALPPS as well, although a reduction in physiological condition in ALPPS patients may be limiting compared with non-ALPPS liver resection patients. In our study, a selective cardiopulmonary work-up was applied whenever it was indicated after physical examination. It is also likely that these favorable outcomes can, to some extent, be attributed to other factors. Apart from the first report of the international ALPPS registry, the largest multicenter experience available is a recent publication of 62 patients from France and Belgium (6, 9). The 62 operations reported included all patients from nine different hospitals during the period studied. This study represents a subgroup of over 30 patients who underwent ALPPS at the two hospitals; therefore, some of the differences may be due to the learning curve associated with a new procedure, although some of the cases presented herein were treated early in the ALPPS experience in Sweden. The French-Belgian study included four (6.5%) patients with gallbladder cancer and 14 (22.6%) with venous reconstructions. Half of the hepaticojejunostomies were performed at ALPPS stage 1. In addition, digestive procedures, including the Whipple procedure, were included (6). Furthermore, the bile duct of the side to be resected was ligated in two patients, a procedure that probably will lead to bile leakage if adequate drainage is missing (16). Furthermore, this study does not include any cases of gallbladder cancer because early experience reported by others with this diagnosis was discouraging. In our study, venous reconstruction would have been necessary in one patient to achieve R0 resection. The patient, however, had insufficient growth of the FLR after 6 days as well as signs of liver failure. At the second-stage operation (performed after 15 days), tumor invasion of the left liver vein was noted. A decision was made not to challenge the patient with resection of the vein, and R2 resection was performed. Two of our patients required resection of the extra hepatic bile duct, one with a Klatskin tumor and one with secondary extension of IHCC to the liver hilum. The strategy decided upon was to postpone resection and reconstruction until stage 2, as complications to the procedure performed at stage 1 could interfere with the regenerative capacity of the FLR. This reasoning is supported by the findings in the Franco-Belgian cohort (6).
Multiorgan resections involving the liver and pancreas have been associated with significant morbidity and mortality (17, 18). Combining extended hepatectomies with the Whipple procedure (hepatopancreaticoduodenectomy) has been associated with up to 20% mortality, although series with better results have been reported when PVE is applied if the FLR is less than 50% of the total liver volume (19, 20). Combining major pancreatic surgery with ALPPS, which necessarily involves a small FLR volume, is probably not wise.
In a German series with a high proportion of primary hepatobiliary malignancies, portal vein resections were performed in two patients with Klatskin tumors, and three of the four patients who died postoperatively had American Society of Anesthesiologists (ASA) class 3 (4). In that study, one-third of the patients had ASA class 3 compared with one patient in our study. Although the median age in the German study was slightly lower (67 years) and separation between CRLM and other malignancies was not conducted, the relatively high ASA class and poor outcome compared with our study suggest a more restrictive/careful patient selection.
Unfortunately, this study could not include patients who were evaluated for ALPPS but found unfit for surgery or unresectable; therefore, intention to treat analysis is impossible.
The limited size of this study makes meaningful statistical analysis of survival data difficult. In Sweden, the median survival of patients diagnosed with HCC who receive no treatment or only medical treatment is approximately 6 months, and the 18-month survival is approximately 10% (21). Of the four patients with HCC included in this study, two are deceased, both with survival longer than 6 months, and the other two had a shorter follow up. This could reflect a treatment benefit with ALPPS but patient selection as well as a low number of patients in the study could also explain these findings. The prognosis of patients with cholangiocellular carcinoma (IHCC and Klatskin) who receive only medical treatment or no treatment at all is even worse, with a median survival <6 months (21). Three of the four patients with cholangiocellular carcinoma in this study are alive after more than 6 months, while the fourth has a shorter follow-up. Again, selection bias cannot be ruled out, although a treatment benefit seems more likely.
In conclusion, this study shows that ALPPS can be carried out for primary hepatobiliary malignancies and nCRLM with acceptable morbidity. Patient selection with a focus on “primum non nocere” is prudent for this complex surgery. Long-term follow up is lacking but the available data suggest a survival benefit for treated patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the regional ethic boards, Linköping, Stockholm and Oslo.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.