
Abstract
Background and Aims:
The increase in liver surgery and the proportion of resections done on the margin to postoperative liver failure make preoperative calculations regarding liver volume important. Earlier studies have shown good correlation between calculations done with ImageJ and specimen weight as well as volume calculations done with more robust systems. The correlation to actual volumes of resected liver tissue has not been investigated, and this was the aim of this study.
Material and Methods:
A total of 30 patients undergoing well-defined liver resections were included in this study. Volumes calculated with ImageJ were compared to volume measurements done after the retrieval of resected liver tissue.
Results and Conclusions:
A strong correlation between calculated and measured liver volume was found with sample concordance correlation coefficient (ρc) = 0.9950. The knowledge on the nature of liver resections sets liver surgeons in a unique position to be able to accurately predict the volumes to be resected and, therefore, also the volume that will remain after surgery. This becomes increasingly important with the evolvement of methods to extend the boundaries of liver surgery. ImageJ is a reliable tool to preoperatively assess liver volume.
Introduction
With the increase and improvement of liver surgery, more and more extensive operations are being performed and the boundaries for resections are pushed forward. Despite this, there is a limit to how much of the liver can be removed or rather how little can be left to avoid liver failure. This limit is not well defined and may be assessed with a number of different methods. Methods to assess the liver function include the indocyanine green-15 (ICG-15) clearance test as well as galactose breath test (GBT). The volume of the future liver remnant (FLR) may be measured radiologically and the ratio FLR/total estimated liver volume (TELV) or total (measured) liver volume (TLV) can then be calculated. For a healthy liver, this ratio should not be less than 0.2 if postoperative liver failure is to be avoided (1). Another way to assess the adequacy is to calculate FLR/body weight, and when this ratio is less than 0.5, the risk of postoperative liver failure is greatly increased.
There are numerous methods to assess liver volume radiologically. Already in 1979, a method to measure liver volume with computed tomography (CT) was described, and in 1983, a good correlation was found between CT volumetry and water displacement of organs (2, 3). Today, the methods that are based on CT can be divided into two main categories: those that require special radiological skills and equipment and those that can be performed on a personal computer with limited radiological skills. The more complex software generally offer the advantage of requiring less manual work and have been developing over more than 20 years (4). In comparison to manual volumetry, automated volumetry has been shown to be faster when TLV is measured (5). It has been shown that volumetry may be performed with software without specialized radiological skills, but in some cases, this requires editing of the original films that is cumbersome (6). ImageJ is a software, developed by the National Institutes of Health (NIH) that belongs to the category of “user-friendly” software. The software can be freely accessed at http://rsb.info.nih.gov/ij/. Volumetry using ImageJ has previously been compared to the weight of liver tissue surgically removed measured at the pathology department, and a good correlation was reached although the study was somewhat limited by the small number of patients (7). The software has also been compared to more sophisticated programs requiring specialist radiological skills, and in this setting, good correlation was shown (8). The aim of this study was to compare the results of volumetry using ImageJ to the actual volume of liver tissue removed at surgery and thereby test the hypothesis that ImageJ used for volumetry by liver surgeons in clinical practice yields accurate information regarding liver volume.
Material and Methods
Patient Selection and Surgery
A total of 30 patients undergoing well-defined anatomical liver resections at the University hospital of Linköping were included in the study popula-tion. The resections included and were restricted to resection of segments 2 and 3, left-sided hemi-hepatectomy, extended left-sided hemi-hepatectomy, right-sided hemi-hepatectomy, and extended right-sided hemi-hepatectomy. All liver transections were performed with cavitron ultrasonic surgical aspirator (CUSA). Indications for resections were both metastatic diseases (from colorectal primary) and primary liver tumors, hepatocellular carcinoma and cholangiocarcinoma. Most of the patients with colorectal liver metastases received preoperative chemotherapy, while none of the patients with primary liver tumor did. Patients with previous liver surgery were excluded, while patients with previous portal vein embolization (PVE) and patients treated with associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) were included (Table 1).
Indications for liver resection in 30 patients.
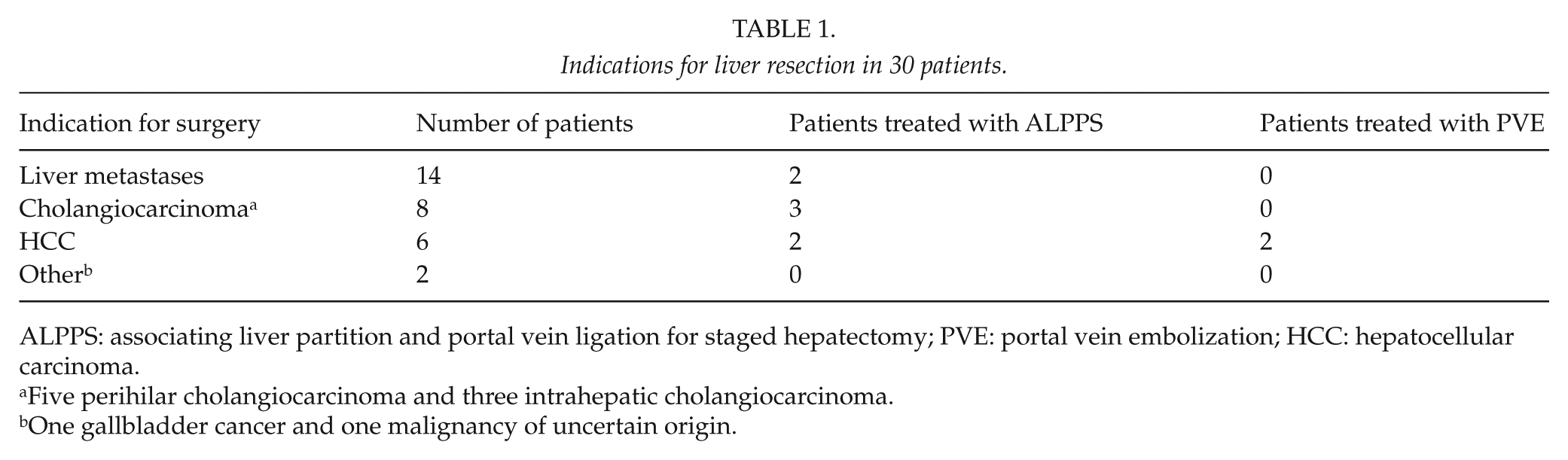
ALPPS: associating liver partition and portal vein ligation for staged hepatectomy; PVE: portal vein embolization; HCC: hepatocellular carcinoma.
Five perihilar cholangiocarcinoma and three intrahepatic cholangiocarcinoma.
One gallbladder cancer and one malignancy of uncertain origin.
ImageJ Calculations or Measurements
Based on availability, either CT or magnetic resonance (MR) studies for the patients were exported from the IDS7 version 14.3.10.3 (Sectra AB, Linköping, Sweden). When both CT and MR were available, CT was used. Before exporting, a line measuring 200 mm was drawn on one of the slides to facilitate later scaling of ImageJ. The radiological studies were exported as .avi files without compression with seven frames per second. The .avi files were then imported to ImageJ using the “file” menu followed by “import” and finally “AVI …”. After importing the file, a line was drawn, using the line tool, on the line previously drawn in the IDS7 system. After this, scaling was done in the “Analyze” menu, followed by “Set scale …” where the known length of the line (from the IDS7) was used as input (Fig. 1A, B).
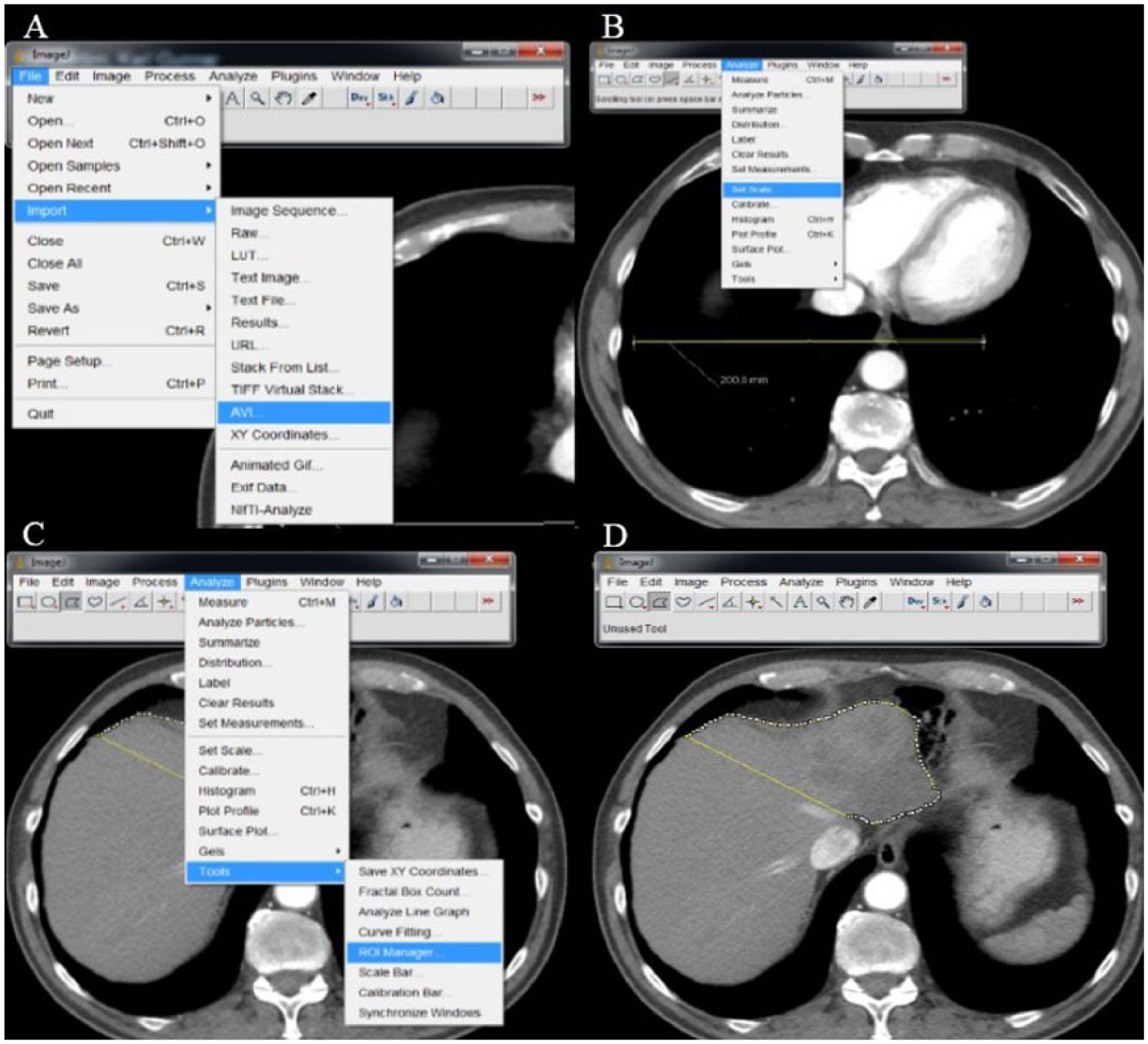
Use of ImageJ to measure liver volume: (A) importing .avi file, (B) setting the scale to match the imported file, (C) opening ROI Manager, and (D) the outlines of the left hemiliver below the junction of the right and middle hepatic vein and the caval vein.
The outlines of the resection were then drawn, using the “Polygon” tool, on each slide and added to the ROI Manager (file menu “Analyze” followed by “Tools” and finally “ROI Manager …”; Fig. 1C, D). When all slices containing liver tissue to be resected had been drawn and added to the ROI Manager, the “Measure” button in the ROI Manager was used to calculate the area of each of the selections. Then, the area of the top and bottom selection was multiplied by half the thickness of the slices, and the others were multiplied by the thickness of a slice (typically 5 mm). Finally, the volumes calculated were added, and in this way, the total volume of the resection had been calculated. This procedure is the same as described earlier apart from multiplying the area at the top and bottom with half of the slice thickness (7). The measurement takes 15–20 min for each patients, and all measurements were done by either a consultant liver surgeon or a fellow, both experienced in evaluating liver imaging for resectability.
Measurements on Resected Liver Tissue
During the liver operation, directly after removal of the resected tissue, it was immersed in a known amount of water in a scaled container. Before immersing in water, the tissue was placed in a plastic bag in order to avoid interfering with later pathological examination and hinder fluid contents of the resected liver mixing with the water. The bags were carefully emptied of air before closure; however, suction-closing was not used. The increase in water level was taken as the volume of resected tissue. The measurement was done by operation room staff specifically instructed in the procedure.
Statistical Analysis
Correlation between computerized measurement of liver volume and real liver volume was calculated as Lin concordance correlation coefficient with an online calculator provided by https://www.niwa.co.nz/node/104318/concordance. All other statistical analyses were performed with IBM SPSS version 22 (International Business Machines Corp., Armonk, NY).
Results
The 30 resections included were 9 right-sided hemi-hepatectomies, 7 extended right-sided hemi-hepatectomies, 6 left hemi-hepatectomies, 5 left lateral sector resections (segments 2 and 3), and 3 extended left hemi-hepatectomies. The median calculated volume was 881 mL (427–1531 mL, 25th–75th percentile). The median measured volume was 890 mL (425–1500 mL). The median difference between calculated and measured volumes was 38 mL (19–56 mL). The median difference expressed as a % of the measured volume was 5% (2.3%–6.6%). The median standardized total liver volume (sTLV) according to the formula published by Vauthey et al. (9) was 1701 mL (1428–1946 mL). The difference between calculated and measured liver volumes expressed as % of sTLV was 2% (1%–3.8%). The concordance correlation between calculated and measured volumes was 0.995 (95% confidence interval (CI) 0.9898–0.9975) as was Pearson correlation coefficient (p < 0.01; Fig. 2).
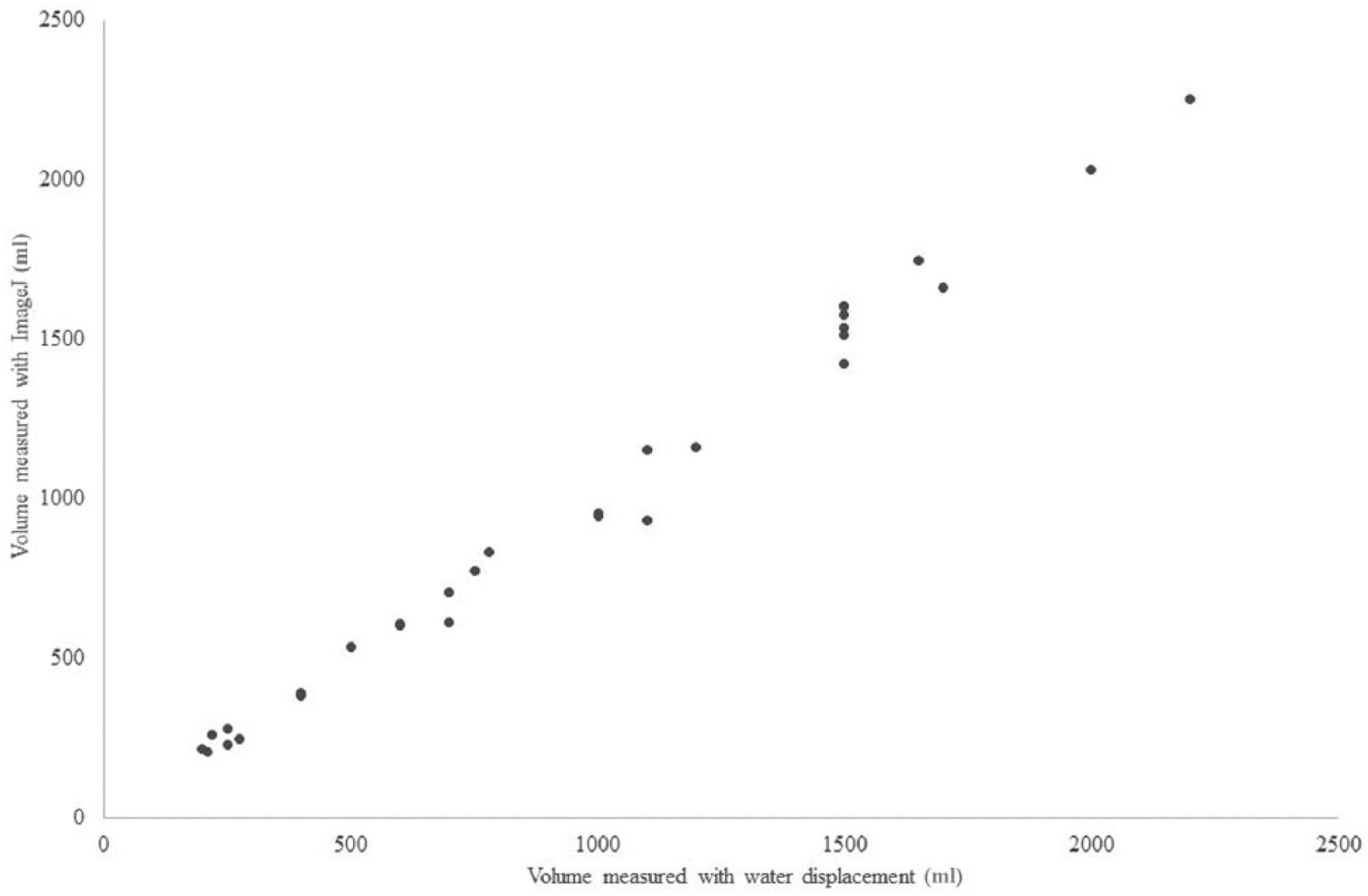
Concordance correlation graph of 30 volumetric analyses of liver resections. Concordance correlation coefficient 0.995 (95% CI 0.9898–0.9975).
For the nine cases of right-sided hemi-hepatectomy, the concordance correlation coefficient was 0.9876 (95% CI 0.9470–0.9971), and for the seven extended right hemi-hepatectomies, it was 0.9859 (95% CI 0.9328–0.9971). The six left-sided hemi-hepatectomies had concordance correlation coefficient 0.995 (95% CI 0.9683–0.9992), while the five left lateral sector resections had 0.995 (95% CI 0.9801–0.9987). No difference was noted in concordance correlation between low volume (n = 10), medium volume (n = 10), and high volume (n = 10; data not shown).
Discussion
This study has shown, for the first time, that calculations on liver volume from radiological studies, done on a personal computer by surgeons with the free software ImageJ correlate well with real volume measurements on the liver tissue resected surgically. These findings are supported by earlier studies with smaller number of patients that have shown good correlation between the volume calculated with ImageJ and weight of specimens as well as volumes calculated with software that demands specialized radiological skills (7, 8).
As good concordance correlation was found between volume calculated and volume measured regardless of the type of liver resection or volume resected. Therefore, the results seem to be applicable to various resection types and sizes. Although liver volume is not the only factor that can and should be assessed before large liver resections to minimize the risk of postoperative liver failure, it is one of the most important ones when marginal resections are planned. With the recent introduction of ALPPS, more and more patients may be offered resections of extensive liver tumors because of the dramatic increase in liver volume observed with the treatment (10). Portal venous embolization has since many years been known to increase liver volume and, therefore, giving some patients with large or multiple liver tumors the opportunity to become tumor free with surgery. These treatment options as well as the standard resection “up front” demand thorough assessment of the liver volume to be able to select the right patients for the various treatments. Even though radiologists equipped with sophisticated software can arguably do more detailed calculations, the experience and knowledge on the nature of liver resections is not to be underestimated. The decision making when it comes to surgery and what kind of resections to offer is always the surgeon’s responsibility. This makes the “hands-on” use of ImageJ (or other similar products) by surgeons performing extensive liver resections important.
Conclusion
ImageJ volumetry is a reliable tool to preoperatively assess the volume of the tissue to be resected. Therefore, it may be safe to assume that it can also be used to assess the more important factor, the volume of liver tissue to be left in place. We encourage liver surgeons to embrace this free software produced by the NIH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the regional ethical board, Linköping University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was not required according to the ethical approval.