
Abstract
Background:
The implementation of the multidisciplinary team conference has been shown to improve treatment outcome for patients with gastric- and gastroesophageal cancer. Likewise, the staging laparoscopy has increased the detection of patients with disseminated disease, that is, patients who do not benefit from a surgical resection. The aim of this study was to compare the multidisciplinary team conference’s decision in respect of M-staging with the findings of the following staging laparoscopy.
Methods:
Patients considered operable and resectable within the multidisciplinary team conference in the period 2010–2012 were retrospectively reviewed. Patient data were retrieved by searching for specific diagnosis and operation codes in the in-house system. The inclusion criteria were as follows: biopsy-verified cancer of the esophagus, gastroesophageal junction or stomach, and no suspicion of peritoneal carcinomatosis or liver metastases on multidisciplinary team conference before staging laparoscopy. Furthermore, an evaluation with staging laparoscopy was required.
Results:
In total, 222 patients met the inclusion criteria. Most cancers were located in the gastroesophageal junction, n = 171 (77.0%), and most common with adenocarcinoma histology, n = 196 (88.3%). The staging laparoscopy was M1-positive for peritoneal carcinomatosis in eight patients (16.7%) with gastric cancer versus nine patients (5.3%) with gastroesophageal junction cancer. Furthermore, liver metastases were evident in zero patients (0.0%) and four patients (2.3%) with gastric- and gastroesophageal junction cancer, respectively. The staging laparoscopy findings regarding peritoneal carcinomatosis were significantly different between gastric- and gastroesophageal junction cancers, p = 0.01. No significant differences were found regarding T-/N-stage or histological tumor characteristics between the positive- and negative-staging laparoscopy group.
Conclusion:
The M-staging of the multidisciplinary team conference without staging laparoscopy lacks accuracy concerning peritoneal carcinomatosis. Staging laparoscopy remains an essential part of the preoperative detection of disseminated disease in patients with gastric- and gastroesophageal cancer.
Introduction
Patients with gastric- and gastroesophageal cancer have a poor prognosis, mainly due to advanced tumor stage and disseminated disease at presentation. Consequently, only 35%–40% of patients are undergoing intended curative therapy (1, 2). The modern diagnostic work-up in the management of gastric- and gastroesophageal cancer includes the multidisciplinary team conference (MDT). The purpose of the MDT is to discuss the patients individually from different medical viewpoints, with the aim of choosing the most optimal treatment and optimize outcome. Several studies have shown that MDT increases the percentage of patients receiving complete staging, and decreases the time from diagnosis to treatment and, hence, is of benefit for the patients (3, 4).
In the preoperative assessment, the introduction of the staging laparoscopy (SL) has also contributed significantly to the identification of peritoneal carcinomatosis (PC) and liver metastases (LM), not verified by computed tomography (CT) (5, 6). Thus, futile laparotomies may be avoided and appropriate palliative treatment initiated for patients with disseminated disease.
At our department, we introduced SL in 2010. Still, not all Danish institutions perform SL but maintain an MDT as the exclusive basis of treatment decision. Therefore, we aimed to determine how precise our MDT was in respect of M-staging in comparison with the findings of the following SL.
Methods
Patients considered operable and resectable with a biopsy-verified cancer of the stomach, gastroesophageal junction (GEJ), or esophagus were identified between 2010 and 2012 by searching for specific diagnosis and operation codes in the in-house system. The retrieved data were assessed by two independent reviewers (Strandby R.B. and Egeland C.), and eventual discrepancies were ruled out by reassessing the medical journals. For inclusion, no suspicion of PC or LM at MDT was required. Likewise, accessible information of the SL performed was mandatory. The study was approved by The Danish Data Protection Agency and the Danish Health and Medical Authorities.
Multidisciplinary Team Conference
All patients were discussed at the MDT. The tumor board consisted of highly specialized consultants from the specialties: surgical gastroenterology, thoracic surgery, radiology, oncology, pathology, and nuclear medicine. Before evaluation at MDT, the patients underwent a diagnostic work-up including physical examination, spirometry, upper endoscopy with biopsy, CT of the chest and abdomen combined with ultrasound of the neck, and/or positron emission tomography-computed tomography (PET-CT) for tumor staging. The CT-scanners used were multidetector-CT scanners (MDCT) with 16–64 detectors.
On the basis of the patients’ estimated TNM-stage (TNM Seventh edition (7)), comorbidity, and resectability, a consensus on treatment strategy was reached between the physicians at the tumor board. If the patients did not have any signs of disseminated disease on CT, PET-CT, or ultrasound of the neck, and had no or an acceptable degree of comorbidity, a SL was scheduled. SL was performed to rule out PC, LM, or other sites of potential dissemination before further treatment was established.
Staging Laparoscopy
After induction of general anesthesia, a 5 mm supraumbilical- or subumbilical-incision was made. Abdominal access was established preferably with Verres Cannula or open technique ad modum Hassan, depending on the individual patient’s surgical anamnesis. After adequate insufflation of CO2 in the peritoneal cavity, a 5 mm trocar was placed below or above the umbilicus. The four quadrants were inspected thoroughly for any malignancy, that is, PC or LM. If indicated, a second trocar was placed to elevate the left liver lobe or mobilize the omentum for optimized visibility of the stomach or GEJ. Intraoperative ultrasound was not performed; thus, only superficial lesions could be assessed. Moreover, PC was defined as any suspicious lesions on the peritoneal surface including the greater omentum. If suspicious plaques and/or acites were evident, biopsies were obtained and/or ascites were aspirated for analysis. For patients with negative findings on SL, neoadjuvant chemotherapy and subsequent resection of tumor were offered.
Statistics
Statistics was made with IBM SPSS® version 20.0.0 (SPSS, Inc, Chicago, IL). The distribution of independent variables was characterized with descriptive statistics. Pearson’s chi-square and Fisher’s exact test was used for nominal variables. A two-sided p-value ⩽ 0.05 was considered significant.
Results
In a 24-month period, 230 patients of all patients discussed on the MDT received a SL. Of those, there was no suspicion of PC or LM in 222 patients before SL was performed. These patients accounted for the study cohort. Eight patients were excluded due to initial suspicion of LM (n = 2) and PC (n = 6) at MDT, which were biopsy-verified by SL. These patients were all offered palliative chemotherapy without primary resection of tumor. Only 22 (9.6%) patients received a PET-CT. Of those, there was suspicion of LM in one patient, and PC in one patient, which was biopsy-verified at the following SL. Thus, 20 patients had a negative PET-CT and SL.
The primary cancer was located in the GEJ in 171 patients (77.0%), the stomach in 48 patients (21.6%), and the esophagus in 3 patients (1.4%). These cancers were most commonly adenocarcinomas (88.3%) with an advanced T- and N-stage (Table 1).
Patient characteristics.
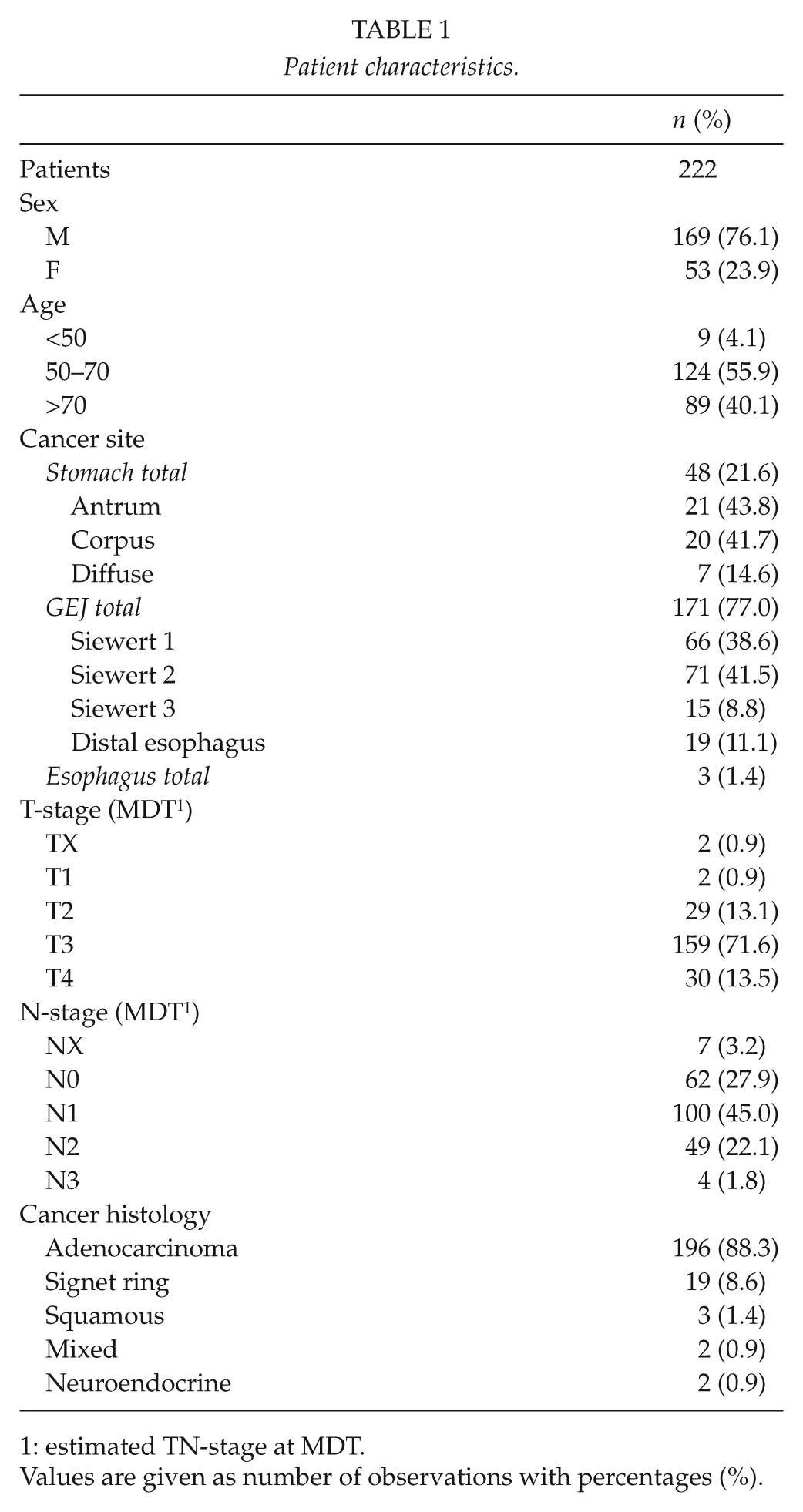
estimated TN-stage at MDT.
Values are given as number of observations with percentages (%).
All 222 patients underwent a SL after the MDT. The overall findings of the examination were negative in 90.5%, and 9.5% were positive for either LM or PC. All metastases were histologically verified. Of patients (n = 48) with gastric cancer, the SL identified 16.7% and 0.0% with PC and LM, respectively. In comparison, the SL identified only 5.3% with PC and 2.3% with LM in GEJ cancers (n = 171) (Table 2). None of the three patients with esophageal cancer had disseminated disease. The differences between the SL findings regarding PC between stomach- and GEJ cancers were significant, p = 0.01. Due to small numbers, nothing could be concluded for esophageal cancers.
Overview of SL findings and univariate analysis for GEJ- and gastric-cancers.
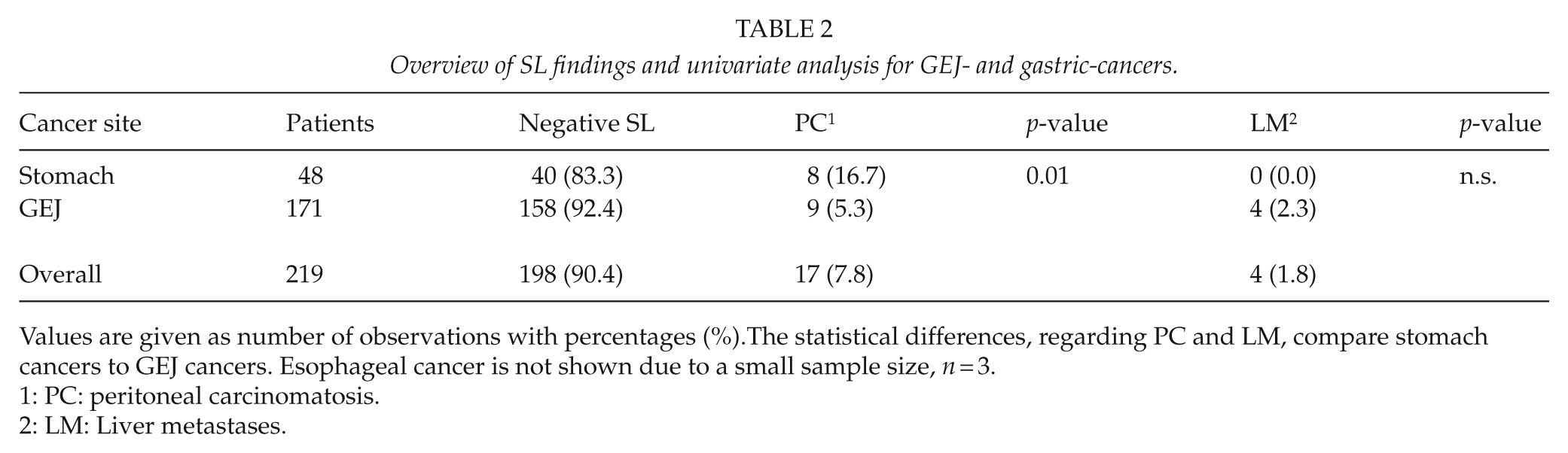
Values are given as number of observations with percentages (%).The statistical differences, regarding PC and LM, compare stomach cancers to GEJ cancers. Esophageal cancer is not shown due to a small sample size, n = 3.
PC: peritoneal carcinomatosis.
LM: Liver metastases.
A subanalysis was made to compare staging and histogical characteristics between the positive SL (+SL) and the negative SL group (−SL) (Table 3). More tumors in the SL+ groups were signet ring cell carcinomas (19.0% vs 7.6%), with more advanced N-stages (81.0% vs 67.2%) and T-stages (90.5% vs 84.8%). However, no significant differences were found between the groups regarding T-stage (p = 0.8), N-stage (p = 0.3), or cancer histology (p = 0.2).
Sub analysis of staging and histological characteristics of positive and negative SL patients with gastric- or GEJ cancers.
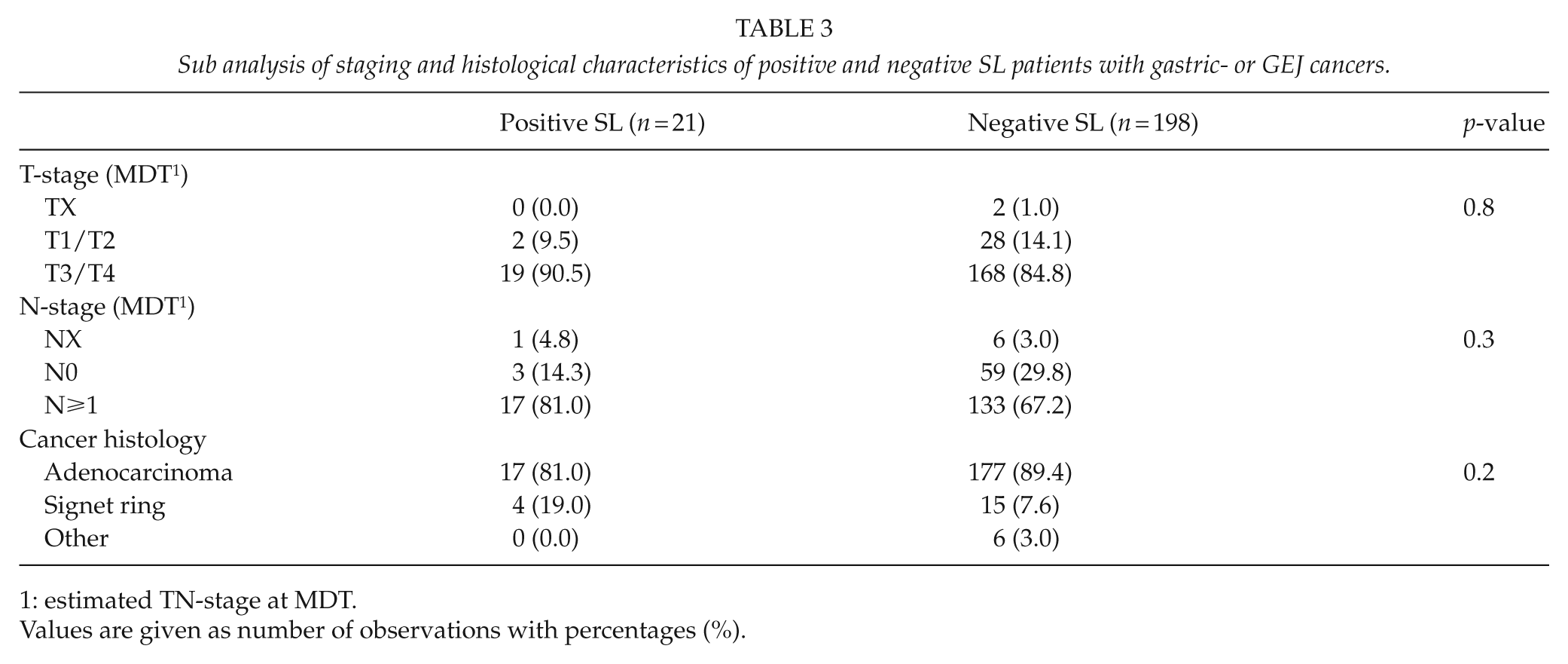
estimated TN-stage at MDT.
Values are given as number of observations with percentages (%).
Discussion
This study found a significant benefit of SL, yielding M1-positive disease in overall 9.5% of patients with gastric- and gastroesophageal cancer, who were initially considered operable and resectable at MDT. Furthermore, a significantly higher proportion of patients with gastric cancer had PC on SL compared to GEJ cancer.
The values of SL in the management of gastric- and gastroesophageal cancer have been reported in several studies, with positive findings in 23%–37.5% for gastric cancer (8–11), and 17%–20% for GEJ cancer (12, 13). Thus, the implementation of SL leads to an altered treatment strategy, or prevents an unnecessary resection of primary tumor of a noteworthy part of the patients examined, due to disseminated disease, and hence poor prognosis. Similarly, PC was found in 16.7% and 5.3% of patients with gastric- and GEJ cancer, in this study. Thus, our results suggest that peritoneal dissemination is less likely present on SL in patients with cancer of the GEJ compared to gastric cancer, and even lower than reported in the literature for both types of cancers. A possible reason for our findings may be that the implementation of the MDT actually optimizes the selection process of resectable patients. Thus, more unresectable or inoperable patients are recognized and correctly palliated, instead of undergoing intended curative therapy. This is in line with findings from a British study, examining the role of MDT with respect to outcome in patients with esophageal cancer (14). The study compared two groups of patients in different time periods, with or without MDT management, respectively. The study found a significant reduction of “open and close” laparotomies and thoracotomies when patients were assessed on preoperative MDT. Furthermore, MDT strategy was significantly associated with better outcome in the multivariate analysis, HR = 0.34, p < 0.001. Similar results have been reported for rectal cancer (15) and breast cancer (16).
Though the MDT seems to benefit the patients, there is still a considerable lack of staging sensitivity, especially when determining M1-disease with PC. This was demonstrated by our findings of 16.7% PC-positive patients at SL for gastric cancer with no initial suspicion of M1-disease. The CT-scan is the cornerstone of the MDT and of substantial value; however, several limitations exist. Despite the fact that a reasonable evaluation of the omentum and larger peritoneal nodules can be achieved, there is still a considerable lack of sensitivity in the evaluation of peritoneal nodules <5 mm (17). The ability to identify PC depends on the slice thickness of the CT-scan, and the introduction of MDCT with thin slices and multiplanar reformation has improved detection of peritoneal nodules (18). This may explain the diverging rates of sensitivity for identifying PC from 14%–76% reported in the literature (18, 19). In contrast, our findings of only 2.3% and 0.0% of LM for GEJ and gastric cancer on SL indicate that the MDT, with decent accuracy, detects these patients before SL is performed.
The impact of MDT on CT-scan accuracy has also been examined (20). A study from 2002 compared the TNM-staging of the preoperative CT-scan between one specialized MDT radiologist and several non-MDT radiologists. The study found a significant difference of 25% versus 5% of M-staging-sensitivity between the MDT radiologists and the non-MDT radiologist. Moreover, the MDT radiologist improved the detection of local invasion more than twofold, and the detection of suspicious lymph nodes over threefold, compared to the non-MDT radiologists. Although, the CT-sensitivity for M-staging was low, even for the specialized radiologist, the study emphasizes the importance of a highly specialized preoperative assessment to achieve a better selection of patients suitable for surgery.
With the purpose of increasing M-staging accuracy, PET-CT has been introduced and examined in comparison with CT and SL. The PET-CT may provide additional information of occult metastatic disease not verified by conventional imaging like distal- or paraaortic lymph nodes or LM (21). A study from 2012 examined 113 patients with advanced gastric- and gastroesophageal cancer. The aim was to evaluate the role of PET-CT in addition to the standard treatment paradigm (21). Of the patients included, 27% had biopsy-verified metastatic disease prior to surgery. PET-CT confirmed only 10% of the dissemination compared to 19% for SL, and only one patient was positive by both modalities. Thus, a minimal overlap was observed. In addition, no patients with PC were identified with PET-CT and one false-positive result was found. Hence, the authors concluded that PET-CT could not be a substitute for SL but add additional staging information, because of the ability to detect M1-disease not visualized on SL. Furthermore, an interesting finding was that if PET-CT was performed prior to SL, one of 10 patients would spare an unnecessary laparoscopy due to clear disseminated disease visualized on PET-CT images. Consequently, the implementation of PET-CT would be of benefit for the patients, reduce the costs of the preoperative assessment, and optimize resources. However, these findings need to be validated in a larger cohort. The additional benefit of PET-CT on decision-making within MDT has also been reported in a recent study evaluating 418 patients (22). The study found that PET-CT prevented 19.7% of patients from undergoing radical treatment due to undetected disseminated disease on CT. The study concluded that PET-CT should be incorporated as a standard modality in the preoperative assessment of gastroesophageal cancer. However, the authors emphasized that PET-positive lesions required bioptic verification for diagnosis of disseminated disease. Thus, the results from these studies underlines an interesting potential for PET-CT, but SL should not be spared in patients with an advanced T- and N-stage, that is, tumors with a high dissemination potential. Our findings of 91% with stage T3/T4 and 81% with a N-stage ⩾1 of patients with a positive SL (Table 3) supports this and international guidelines recommend that SL should be performed in patients with a minimum stage of T1N+ and higher stages of gastric- and GEJ cancers (23).
Our study cohort of 222 patients was evaluated by the same MDT, which we consider a major strength in our study. This may reduce selection bias in this retrospective study. Unfortunately, we did not have a historical group without MDT assessment to compare our findings with. This would have strengthened our results. Only 10% of the patients received a PET-CT-scan. This modality was not a part of the standard diagnostic work-up in the study period, which is why no data are presented for this modality.
In conclusion, our study shows that the MDT conclusion based on diagnostic imaging has a high accuracy for LM, but lacks accuracy for PC. For that reason, SL remains a vital modality in the detection of PC.
Footnotes
Declaration of Conflicting Interests
None of the authors have any conflicting interests to disclose.
Ethics Approval
This study was approved by the The Danish Data Protection Agency (ID: 2007-58-0015) and the Danish Health and Medical Authorities (ID: 3-3013-603/1/).
Funding
This study was partially sponsored by The Danish Cancer Organization (grant number R84-A5558).