
Abstract
Background and Aims:
Restorative proctocolectomy is the most common operation in patients with ulcerative colitis. The aim was to evaluate long-term changes in our operative treatment and early and late complications related to restorative proctocolectomy.
Material and Methods:
The study comprised 352 (149 females) patients over 18 years of age with ulcerative colitis who underwent restorative proctocolectomy in 1985–2009 median follow-up time of 5 years.
Results:
The indication for surgery was active chronic colitis in 168 (47.7%), acute colitis in 159 (45.2%), and cancer or dysplasia in 25 (7.1%) patients. Ileal pouch-anal anastomosis was performed using hand-sewn anastomosis with mucosectomy in 283 patients and stapled anastomosis in 69. A shift from hand-sewn to stapler ileal pouch-anal anastomosis took place in 2005. Covering ileostomy was carried out in 133 (37.8%) patients. There were 82 (23.3%) J-pouch-related complications. The operative mortality was 0.3%. There were significantly fewer leakages and early re-operations when covering ileostomy was used than when it was omitted: 6.0% versus 16.4% (p = 0.004), 4.5% versus 11.9% (p = 0.02), respectively. There were more strictures in hand-sewn than in stapled ileal pouch-anal anastomoses (17.6% vs. 0%, p = 0.001). Pouchitis occurred at least once in 134 (38.1%) patients.
Conclusion:
The ileal pouch-anal anastomosis technique used in restorative proctocolectomy had changed over the past years from hand-sewn to stapled anastomosis. Covering ileostomy seemed to protect against major complications. Pouchitis was the most common late complication.
Introduction
Restorative proctocolectomy (RPC) with ileal pouch-anal anastomosis (IPAA) is the treatment of choice when surgical treatment in ulcerative colitis (UC) is needed (1). The operation is associated with considerable morbidity; leakage and pelvic sepsis are the most serious complications, occurring in 6%–25% of patients (2, 3). Pouchitis is the most common of the late complications; at least one episode is experienced within 10 years after surgery in 25%–48% of patients (4–6); in 3%–17%, pouch failure requiring permanent ileostomy is inevitable (7–9).
The operative technique has gone through changes in recent decades. The use of covering ileostomy is recommended but not mandatory (10, 11). Stapled anastomosis has in many cases replaced hand-sewn anastomosis (12).
The aim of this study was to evaluate the results of RPC in 352 consecutive patients operated for UC in 1985–2009. Special focus was on the effects of the changed IPAA technique on early and late complications.
Material and Methods
All patients with UC who underwent RPC at Tampere University Hospital between March 1985 and December 2009 were identified in the hospital records; the total number of subjects was 352 (149 women, 42.3%), median age of 36 years, range of 18–72. A database was collected from patient files including details on patient history, operation technique, postoperative morbidity, and follow-up.
Indications for surgery were categorized into three groups: acute colitis resistant to conventional medical management, chronic colitis and the development of dysplasia, cancer or estimated high risk of progression to malignancy. Acute colitis was determined when urgent colectomy had to be performed. Chronic colitis included failure of medical treatment, corticosteroid dependent or resistant disease or active disease despite any treatment.
Early complications were defined as occurring within 30 days of the operation. Pelvic sepsis was present when there was a leakage, pelvic abscess, or pelvic infected hematoma. Small bowel obstruction (SBO) was considered a complication when hospital stay exceeded the median 10 days in the whole series.
Late complications consisted of all problems recorded more than 30 days after the operation. The diagnosis of pouchitis was based on clinical signs and symptoms and occasionally on endoscopic and histological findings. Anastomotic stricture was considered a complication if it caused functional difficulties and the dilatation was needed. Pouch failure was defined as the need for a permanent ileostomy with or without pouch excision.
Statistical Analyses
Grouped data are expressed as median and range. Chi-Square or Fisher’s exact test was used to assess differences in categorical variables. Statistical significance was set at p ⩽ 0.05. Binary logistic regression analysis was used to determine the predictors of leakage. Results are shown as odds ratios (ORs) with their 95% confidence intervals (CIs).
Results
Surgery
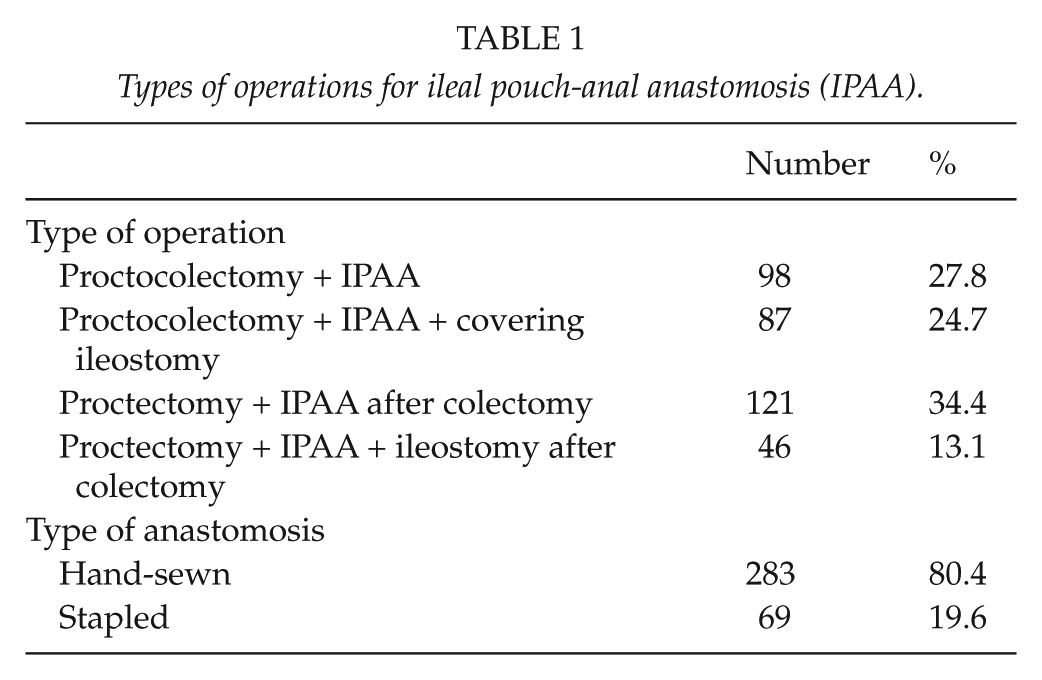
Indications for surgery were acute colitis in 159 (45.2%), chronic colitis in 168 (47.7%), and cancer or risk of cancer in 25 (7.1%) patients. Colectomy was performed on 47.7% of patients prior to the IPAA procedure. During 1985–2005, nearly all IPAAs were hand-sewn with distal mucosectomy, and from 2005 onwards the main technique was a stapled IPAA with a covering ileostomy. Before this, a covering ileostomy was performed only when considered necessary. A J-shaped reservoir was used in all cases. The types of operations and anastomoses performed are shown in Table 1. Four experienced surgeons performed 91% of the operations.
Types of operations for ileal pouch-anal anastomosis (IPAA).
Early Morbidity
Pouch-related complications were the most common, occurring in 82 (23.3%) (Table 2); of these, altogether 61 (17.3% of all) had pelvic sepsis, including 44 leakages. One patient (0.3%) died of postoperative bleeding; he was re-operated on to achieve hemostasis on the first postoperative day, but declined blood transfusions for religious reasons.
Number of pouch-related complications.
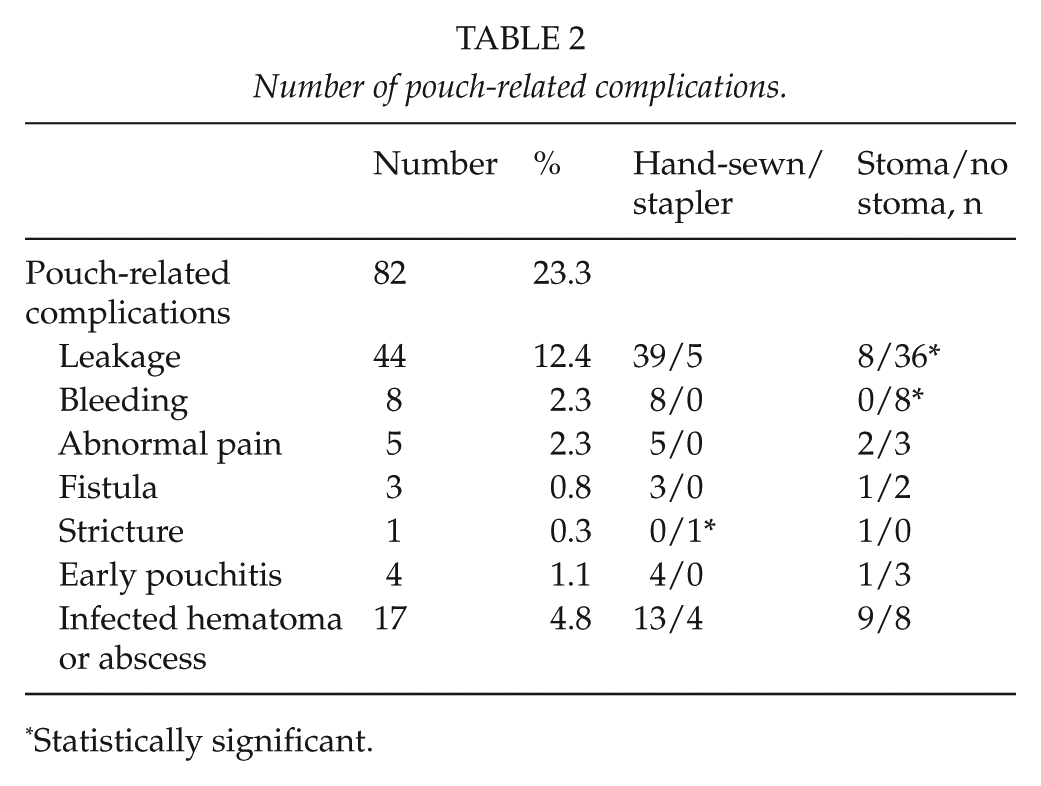
Statistically significant.
A total of 32 (9.1%) of the patients required re-operation due to complications. The indications were leakage in 25, hemorrhage in 2, SBO in 4, and perforation in 1. In all, 23 loop ileostomies were made in these re-operations, of which all but 2 were closed later; 1 permanent end-ileostomy was made due to a leakage.
A total of 81 (23%) patients were re-admitted to hospital within the postoperative period. The reasons were fever in 22, abscess in 20, leakage in 11, dehydration in 9, SBO in 6, and miscellaneous reasons in 13.
There were significantly fewer leakages and early re-operations when covering ileostomy was used than when it was not used, 6.0% versus 16.4% (p = 0.004) and 4.5% versus 11.9% (p = 0.02), respectively (Fig. 1). In the logistic regression analysis, no single factor constituted an independent risk for pelvic sepsis. Omission of covering stoma and high body mass index (BMI) were independent risk factors for leakage, ORs of 3.68 (95% CI: 1.61–8.42) (p = 0.002) and 1.11 (1.01–1.21) (p = 0.03), respectively. When the patients without covering stoma were divided by BMI into four groups (<22, 22–24, >24–27, and >27), the most obese group were found to be at clearly higher risk of leakage, 6.5% versus 25.0% (p = 0.017).
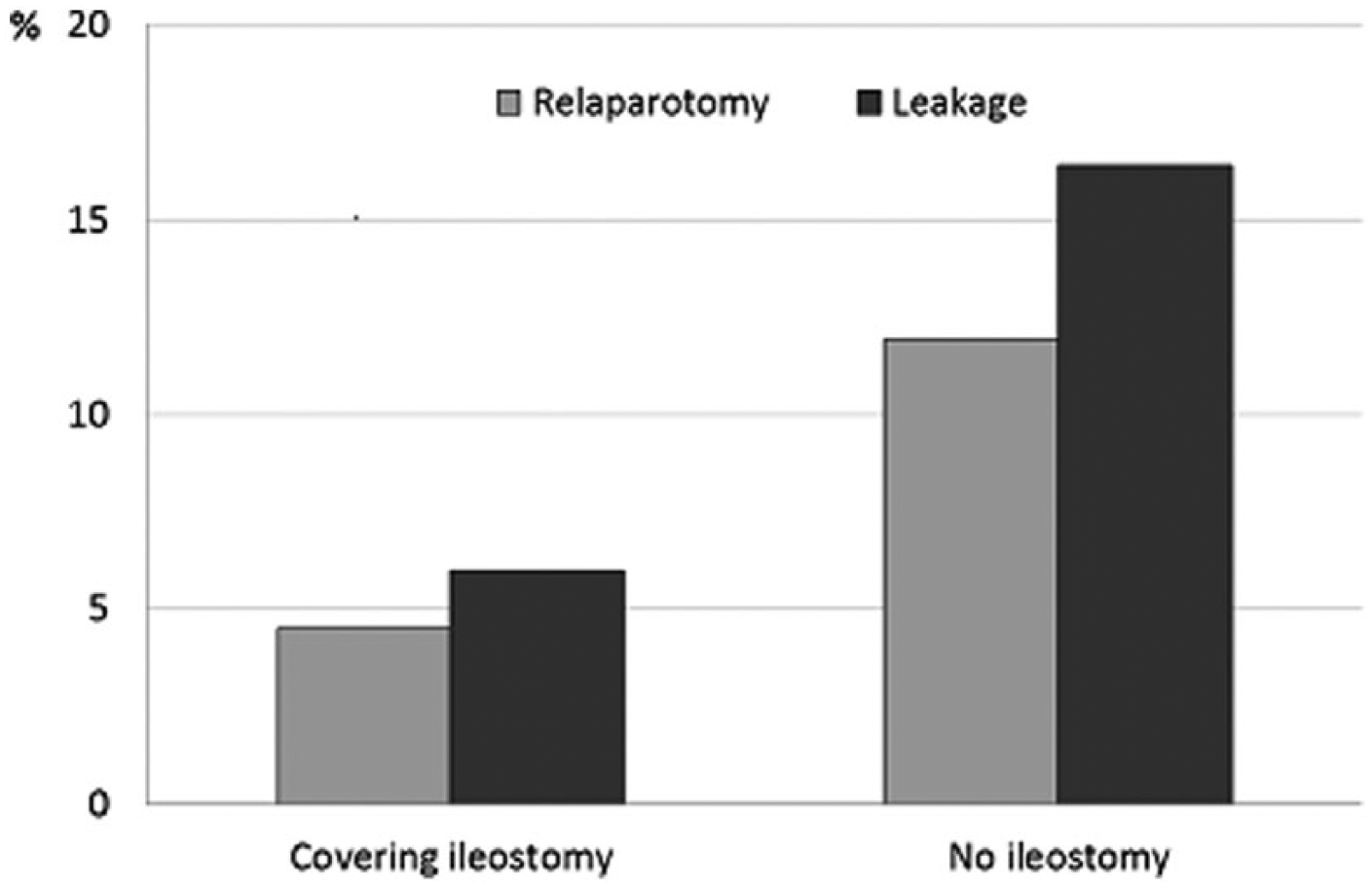
Influence of covering ileostomy on leakages (p = 0.004) and early re-operations (p = 0.02).
Of the early complications, dehydration was the only which occurred significantly more frequently in the patients with covering stoma than in those without stoma, 6.8% versus 0.0% (p < 0.001), respectively. The rate of early SBOs did not differ between these two groups, occurring in 6.0% and 5.9%.
Five of the covering ileostomies made were closed in another hospital. The median time from IPAA to ileostomy closing operation was 113 days (range: 30–912). Of the 125 cases closed in our unit, the median hospital stay was 7 days. The overall morbidity related to closing of covering stomas was 31.6% (n = 42), the most common being SBO in 16.8% patients (n = 25); SBO was considered a complication when it led to longer hospital stay than median or re-admission. A total of 17 (11.4%) patients had an infection complication after ileostomy closure, 4 of whom (3.0%) experienced leakage; all patients with leakage needed re-operation. Three of the covering ileostomies were never closed before pouch excision.
Long-Term Complications
The median follow-up time was 5 years (range: 1 month–24 years). Late complications are presented in Table 3. The most common of these was pouchitis, occurring in 134 (39.3%) patients. Of these 106 (76.3%) experienced more than one episode. A total of 45 (13.2%) patients had at least one episode of SBO; 17 (37.8%) of them underwent a laparotomy and adhesiolysis due to obstruction. The use of covering ileostomy and subsequent closing operation did not result in more late SBOs than omitting the temporary ileostomy, occurring in 14.6% versus 12.4% (p = 0.6), respectively. SBO occurred in 15.9% when IPAA was constructed later after colectomy, and in 10.7% when it was done at the same time (p = 0.16).
Late complications in the series.
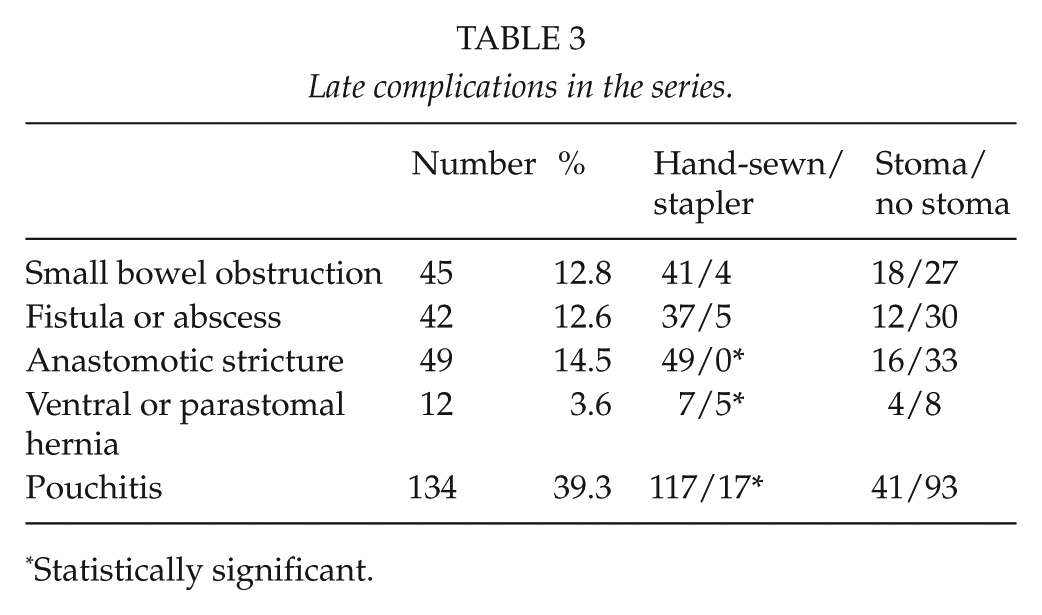
Statistically significant.
Patients with hand-sewn anastomosis had significantly more anastomotic strictures than those with stapled anastomosis (17.6% vs. 0%, p = 0.001).
A total of 41 (12.2%) patients underwent pouch excision, and 1 patient was satisfied with the diverting ileostomy constructed due to peritonitis. One of the patients had the pouch removed due to chronic pouchitis 20 years after the primary operation, and histologic sample revealed mucinotic rectal cancer, of which the patient died 2 years later; in this case, the anastomosis was performed by hand-sewn mucosectomy.
Discussion
The IPAA operation used should offer low postoperative mortality and an acceptable rate of complications. Loop ileostomy is not an ideal form of stoma for the patient to cope with, and it is sometimes associated with considerable morbidity. The only significant difference in early complications between covering stoma and omitting it in our study was dehydration; and the number of patients (n = 9, 6.8%) was low. However, some complications extended the hospital stay. On the other hand, most patients with SBO were treated conservatively after the closing operation, and the most serious complication, leakage, was rare (3%). The morbidity of closing operations in our hospital was at acceptable level when compared to the literature (13).
Some studies recommend ileostomy only in selected cases, since there were no differences in the morbidity rate or pouch-related complications when ileostomy was used or not (10, 14). A meta-analysis of this concluded that the omission of covering ileostomy might be justified in patients defined as low risk, but low risk was not well defined (15). The study by Kiran et al. (16) aimed to identify factors which predict septic complications, and making or omitting stoma had no influence.
Altogether, 18.5% of our patients had experienced pelvic sepsis and leakage occurred in 12.5%. In the literature, the pelvic sepsis figures range from 3% to 25% (2, 3, 5, 7, 17–19) depending on the definition. About one-third (6) of the patients with pelvic sepsis were re-operated on and the others were treated conservatively. Our finding advocates the use of loop ileostomy, as patients with covering ileostomy had significantly fewer leakages and early relaparotomies. This is in line with the recent European Crohn’s and Colitis Organisation (ECCO) recommendation, where the use of loop ileostomy is advocated except in highly selected cases (20). The study by Mennigen et al. (11) supports our finding: they likewise showed that loop ileostomy reduced pouch-related septic complications and the need for early relaparotomies.
SBO is the late complication of IPAA which leads most often to laparotomy. It is thought to be caused especially by pelvic adhesions. In our series, the frequency of early SBO was 5.6% and of late SBO 13.2%. The corresponding figures in the literature are 7.5% and 25% (17). In our series, 20% of early and 35.6% of late SBOs required relaparotomy; the respective percentages in the literature being 3.2%–8.7% and 22.9%–31.4% (17, 21, 22). The incidence of SBO has been reported to increase with time after operation, and has been shown to be more frequent when covering ileostomy is used (22). Our data do not support this.
Stapled technique in anastomosis for IPAA has been shown to result in better nocturnal continence than hand-sewn anastomosis and is also easier to perform (12). According to some studies, stapled technique results in fewer septic complications than hand-sewn technique (23, 24). A systematic review of dysplasia after IPAA in 2040 patients showed a pooled prevalence of dysplasia of 1.13% in the pouch, the anal transitional zone, and the rectal cuff. The only identified risk factor for subsequent dysplasia in the rectal cuff with IPAA was the finding of dysplasia in the surgical specimen (25). It is noteworthy that even hand-sewn mucosectomy is not complete in excising the mucosa of the transition zone (12). Because of the accumulating data in favor of stapler anastomosis as mentioned above, we shifted from making hand-sewn anastomoses to mainly stapler anastomoses around the year 2005.
We still perform hand-sewn anastomosis with mucosectomy, when the patient is operated on for cancer or when there is dysplasia in the rectum. The known risk factors for colorectal cancer in patients with inflammatory bowel disease are family history, extensive colitis with active endoscopic or histologic prolonged inflammation, primary sclerosing cholangitis, and pseudopolyposis (26); in these cases, hand-sewn anastomosis might be recommended, but the issue requires further research.
In this study, one cancer was found after IPAA, and the anastomosis was hand-sewn. Hand-sewn anastomoses resulted in significantly more late strictures than did stapled anastomoses. The same has also been shown in a study comprising 3109 patients (23).
Pouchitis was clearly the most common late complication, 134 (39.3%); 23% had experienced only one episode. These figures are in concordance with other studies reporting pouchitis in 23.5%–48% (3, 5–7, 17).
The main limitations of this study were its retrospective character and the lack of annual follow-up data. The postoperative protocols changed in our hospital during the study period, rendering it challenging to compare the different groups. Also, the different follow-up periods of the two groups of patients with different types of anastomoses made it impossible to compare the long-term outcome between these groups.
In conclusion, serious acute complications in RPC were comparable with previous studies. We favor the routine use of covering ileostomy to avoid the most critical complications considering the functional outcome and long-term success rate, pelvic sepsis, and leakage. The stapled anastomosis technique is favored over the hand-sewn technique, except in selected cases with high risk of dysplasia or cancer. Pouch-related complications are most common in the long-run.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital, Grant numbers 9P060 and 9N002.