
Abstract
Introduction
The impact of diverting ileostomy in adults with ulcerative colitis (UC) undergoing ileal pouch-anal anastomosis (IPAA) is unclear. This study uses a novel approach with population-level data to identify patients with diverting ileostomy at the time of IPAA and determine the impact of diverting ileostomy on postoperative outcomes.
Methods
Using the International Business Machines (IBM) MarketScan® database, adults (18-64 years old) with a diagnosis of UC who underwent IPAA between 2000 and 2019 were examined. Patients were assigned to the diverting ileostomy (DI) cohort or no-DI cohort based on the presence of an ostomy closure code in the 1-year following their IPAA. Rates of ileostomy formation and readmissions were quantified and outcomes between cohorts compared.
Results
There were 540 patients in the no-DI and 2494 in the DI cohort. There were regional differences in the rate of ostomy creation, but the overall rate of ostomy creation remained stable across years. Patients with no-DI vs DI had a longer index length of stay (LOS) (7 vs 6 days, P = .001). Adverse postoperative outcomes did not differ between cohorts. Diversion did not independently affect the likelihood of a 30-day readmission, and since 2000, readmission rates have declined for all IPAA patients.
Discussion
This is the first study to capture population-level data on the effect of diversion at the time of IPAA for adult UC patients. This study demonstrates that the rate of fecal diversion at the time of IPAA has remained stable over time, but readmission rates have declined.
Introduction
Despite advances in medical treatment, there is a 9.6% risk of colectomy in the 10 years following ulcerative colitis (UC) diagnosis. 1 Total proctocolectomy with ileal pouch-anal anastomosis (IPAA) removes the inflammatory disease burden while restoring functional status through creation of an internal fecal reservoir. Due to patient factors and clinical preoperative status, this procedure is often performed in a staged fashion. After the colon and rectum are removed, the internal reservoir—most commonly a J-pouch—is created. Creating a functional pouch is a complex anastomosis with multiple suture or staple lines with a direct connection to the anus. Anastomotic leaks can cause catastrophic consequences and long-term pouch dysfunction. The risk of leak increases if performed in patients with poor tissue quality and healing conditions. Thus, many surgeons opt to create a diverting ileostomy (DI) proximal to the IPAA. Theoretically, this allows the pouch to heal for several weeks prior to ostomy reversal, thus minimizing the risk of a clinically significant anastomotic leak.2,3
A DI can be performed as part of a staged approach to total proctocolectomy (TPC) with IPAA. This can be a traditional 2-stage procedure (TPC and IPAA with DI, then ostomy closure), a 3-stage procedure (total abdominal colectomy [TAC], completion proctectomy with IPAA and DI, and ostomy closure), or a modified 2-stage procedure (TAC, then completion proctectomy without DI). However, the ileostomy and the subsequent takedown carry significant morbidity.4,5 Patients with ileostomies experience high readmission rates for dehydration and stoma-related issues. 6 Several studies have found an increased risk of small bowel obstruction and development of anastomotic stricture with ileostomy. 7 Most significantly, reversing an ileostomy necessitates a subsequent surgery and hospitalization, which may represent unnecessary surgery.
Because of the morbidity and additional procedures associated with ostomies, some centers have shifted to the modified two-stage approach, without diverting ileostomy.8-11 However, data on IPAA outcomes is challenging outside of single institutions because creating an IPAA is coded as “loop ileostomy…if done.” This makes determination of diversion status challenging in population-based studies. Using a national administrative claims database, this study captures one of the largest populations of UC patients undergoing IPAA and uses a novel method to assign patients to cohorts based on the presence of a diverting ileostomy. National diversion rates are summarized over the last 20 years, examine 30-day readmission rates, and quantify the independent impact of diverting ileostomy on the odds of readmission and postoperative infection. The authors hypothesized that there would not be outcome differences between cohorts with and without a diverting ileostomy.
Materials and Methods
Population Identification
A retrospective cohort study was performed using administrative claims data from the International Business Machines (IBM) MarketScan® database (IBM Watson Health, Cambridge, Massachusetts). This database comprises claims data from employer-sponsored, privately insured patients across the United States. MarketScan® contains data from over 43.6M patients—approximately 1/3 of the employer-insured population—to create a nationally representative sample. The database captures longitudinal health care data, including outpatient, inpatient, and pharmacy information.
Patients between 18 and 64 years old that carried an ICD-9 or ICD-10 code for ulcerative colitis (556.XX or K51.X) and a CPT code for IPAA (44158, 45113, 15119, 44211, 45119, 44211, and 45397) were included. Patients were excluded if they did not have 30 days of continuous data in MarketScan® prior to and at least 1 year of follow-up after the IPAA procedure date. Patients were also excluded if they had any of the following colorectal diagnoses: familial adenomatous polyposis, Hirschsprung’s disease, and Crohn’s disease. Lastly, patients were excluded if they underwent additional non-IPAA surgeries during the study period.
Cohort Assignment
CPT codes describing IPAA creation encompass “diverting ostomy…. if done.” To stratify patients whom had a DI at the time of their IPAA, the cohort was queried for patients with a CPT code for enterostomy closure within 1-year after the IPAA procedure. Patients with an ostomy closure code were assigned to the DI cohort; patients who did not have an ostomy closure code were assigned to the no-DI cohort.
Patient demographics and preoperative risk factors, including comorbidities, were collected. The presence of obesity, malnutrition, and preoperative sepsis were queried using ICD codes to identify common risk factors for anastomotic leaks to control for them during analysis. Postoperative complications occurring in the first 30 days were included. ICD codes were used to identify patients with infectious complications, including sepsis, urinary tract infection, pneumonia, and surgical site infections. Additionally, ICD codes for abdominal drainage procedures representing organ space surgical site infections requiring drainage were included. Lastly, 30-day readmissions were captured.
The study protocol was exempt from the Institutional Review Board as it involved deidentified patient data.
Statistical Analysis
Descriptive and bivariate analyses were performed to compare the no-DI and DI cohorts. Wilcoxon rank sum tests were used for continuous variables. Fisher’s exact and chi-square tests were used for categorical variables based on category counts. The Cochran-Armitage test was used for temporal trends in readmission rates. Logistic regression models were created for 30-day readmissions and postoperative surgical site infections, using the presence of a diverting ostomy as the exposure variable. Crude and adjusted odds ratios are reported with 95% confidence intervals. Analyses were performed with significance determined by P-value < .05.
Results
There were 7866 patients between 18 and 64 years old who underwent IPAA between 2000 and 2019 in the MarketScan® database. Of these, 6177 had continuous data prior to and after their IPAA procedure. When patients with diagnoses other than UC and who had other procedures were excluded, the final population size was 3034. Of these, 2494 (82.2%) had a subsequent procedure code for ostomy takedown and were assigned to the DI cohort. The remaining 540 (17.8%) were assigned to the no-DI cohort.
Patient Demographics
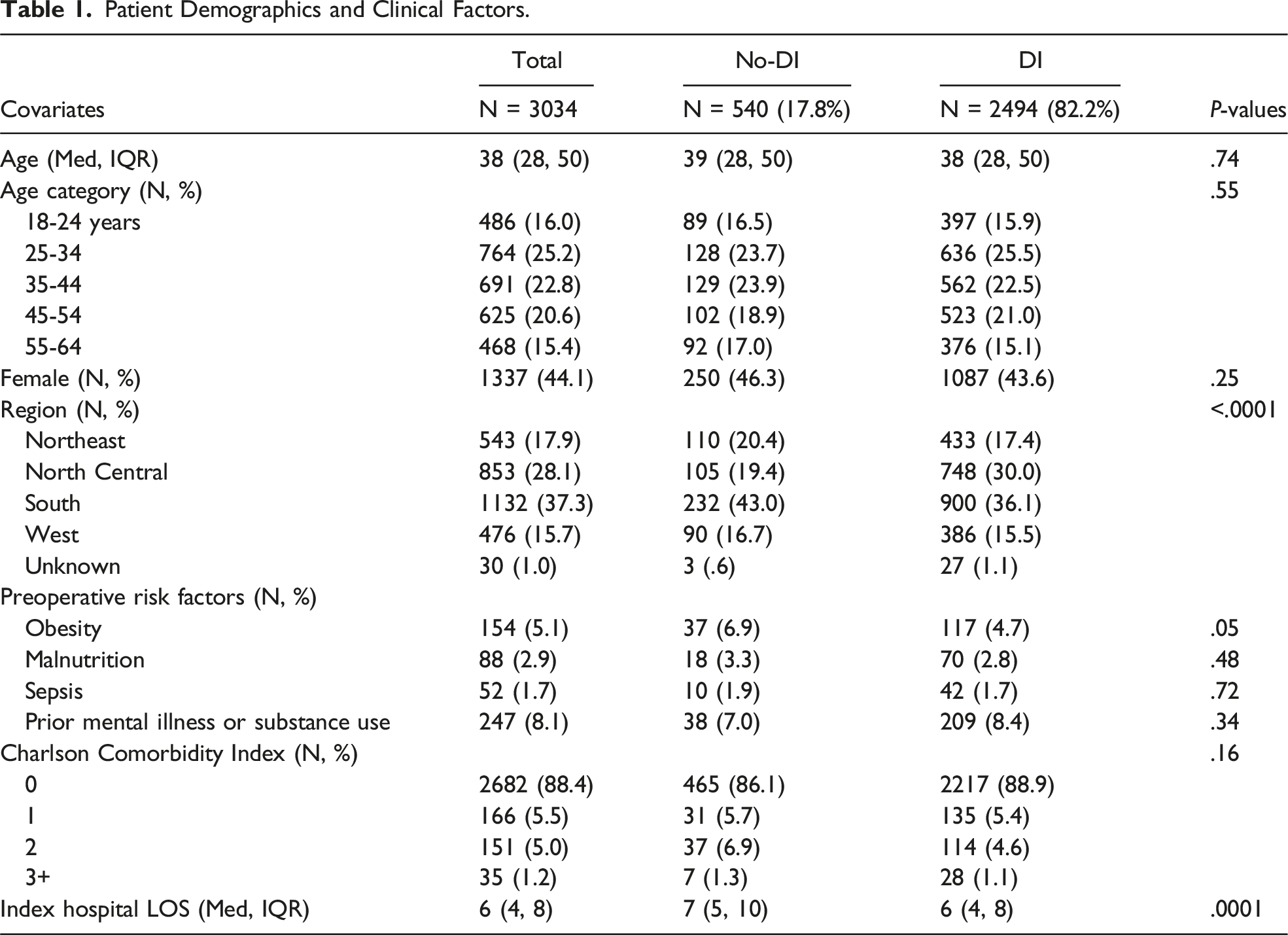
Patient Demographics and Clinical Factors.
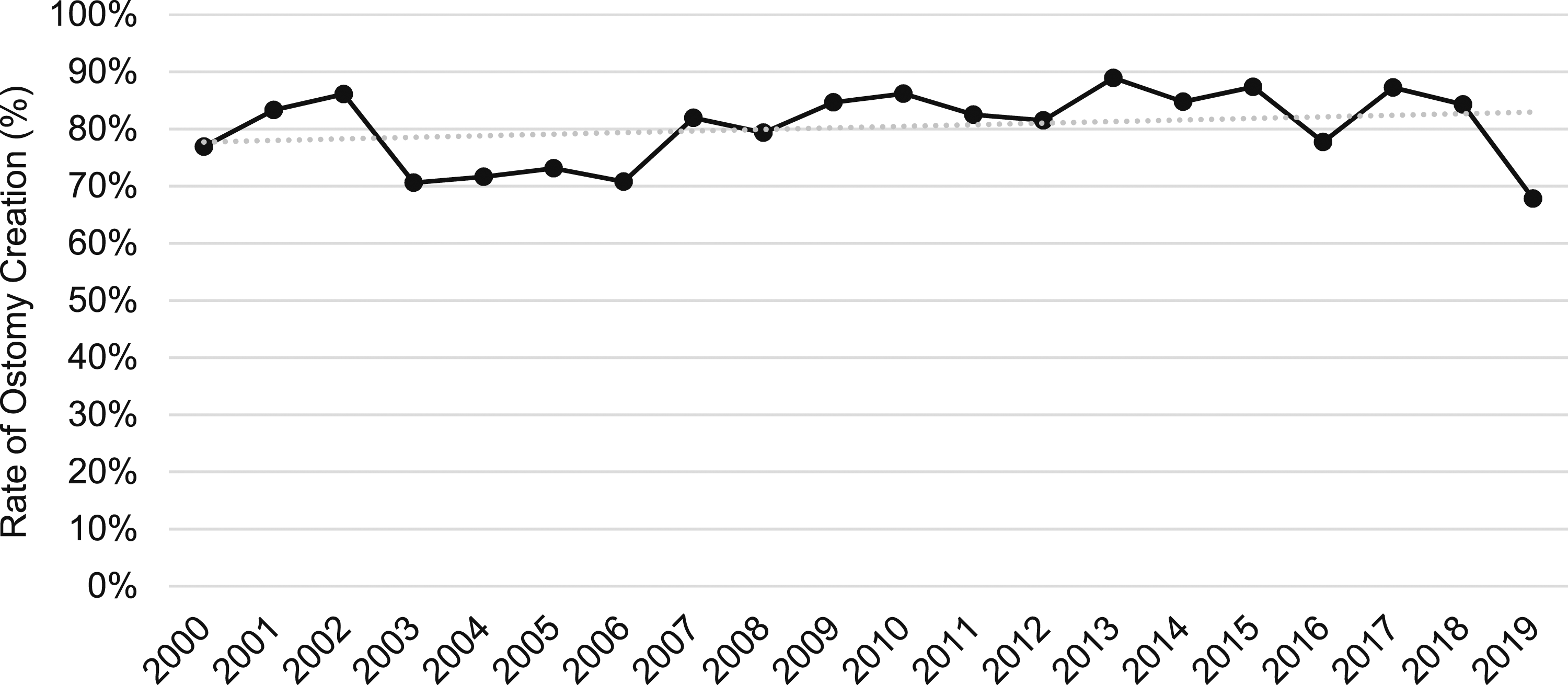
Ostomy creation rate at the time of IPAA across study years.
Preoperative obesity was seen in 5.1% of the patients who underwent IPAA. The prevalence of obesity did not differ between cohorts. A Charlson Comorbidity Index of 0 was found in 88.4% of all IPAA patients. Hospital length of stay was shorter in the DI cohort (6 vs 7 days, P = .0001).
Postoperative Adverse Outcomes
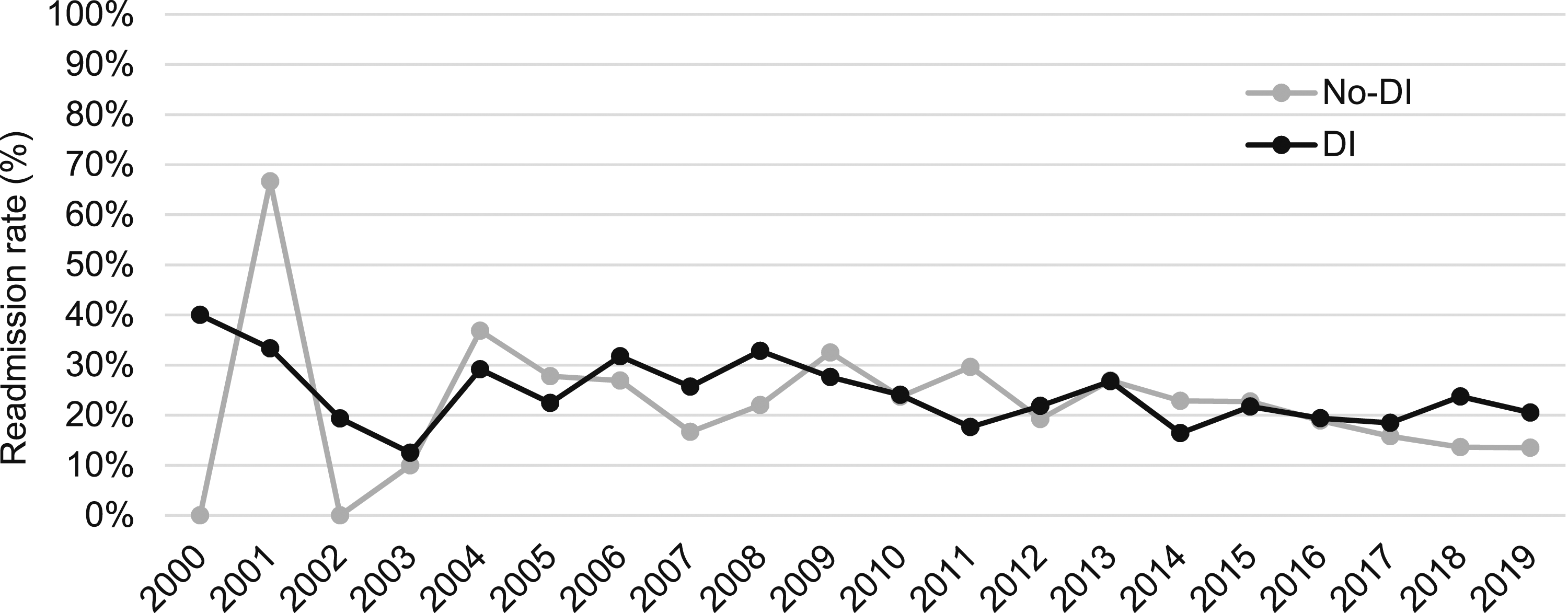
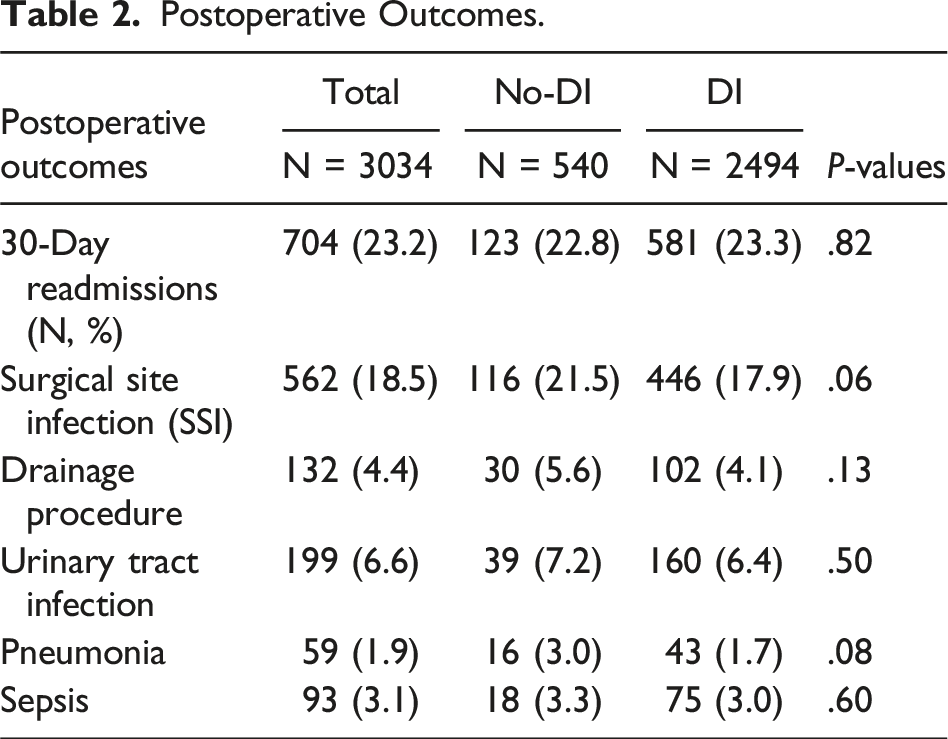
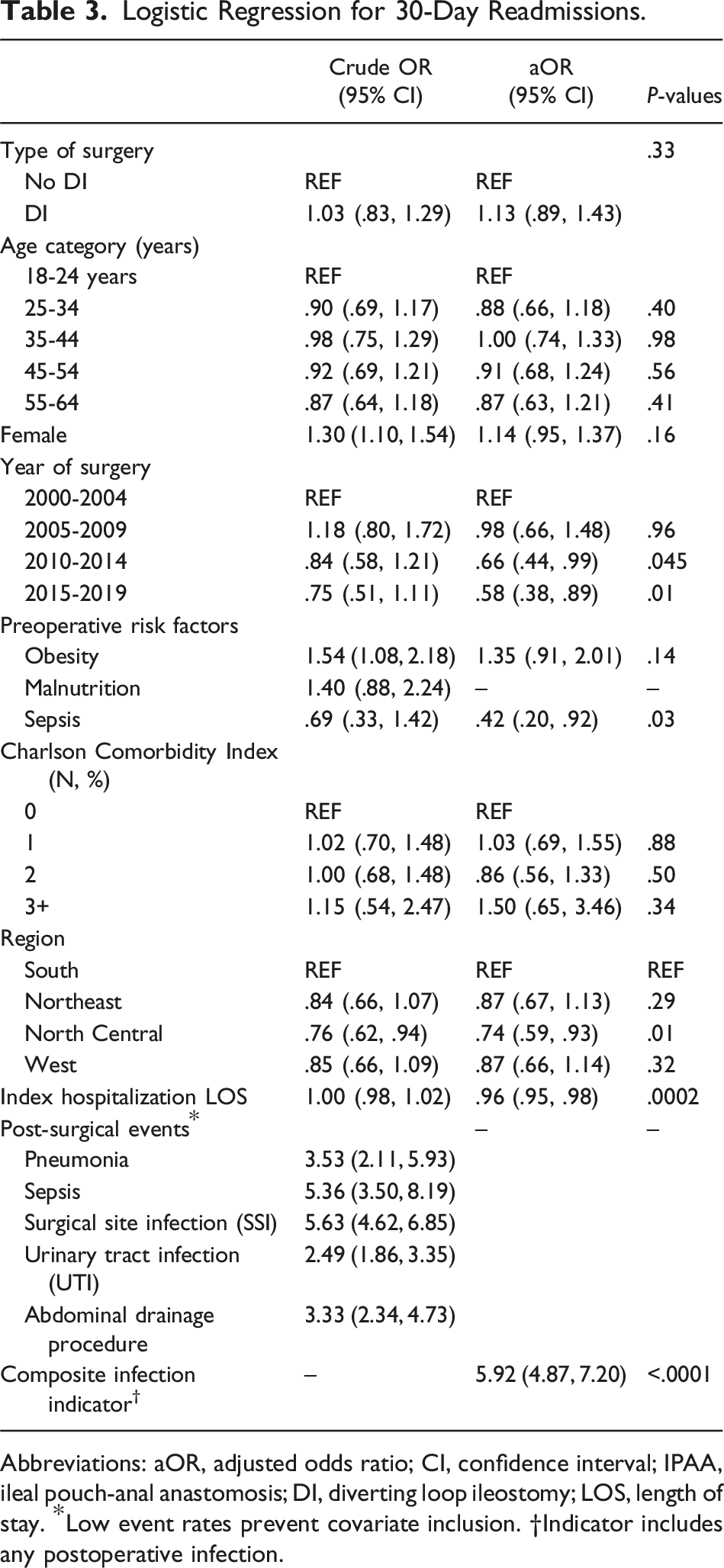
The most common postoperative adverse outcomes were 30-day readmission (23.2%) and surgical site infections (18.5%). The prevalence of adverse events did not differ between cohorts (Table 2). For all patients undergoing IPAA, the combined readmission rate over time decreased throughout the study years at a rate of .48% per year (P = .0009) (Figure 2). When stratified into cohorts, the readmission rates of both the no-DI and DI cohorts did not significantly decrease across study years (P = .06) (Figure 3) (Tables 2and 3). 30-Day readmission rates for all IPAA patients across study years. 30-Day readmission rates for IPAA patients stratified by the presence of diverting ileostomy across study years. Postoperative Outcomes. Logistic Regression for 30-Day Readmissions. Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; IPAA, ileal pouch-anal anastomosis; DI, diverting loop ileostomy; LOS, length of stay. *Low event rates prevent covariate inclusion. †Indicator includes any postoperative infection.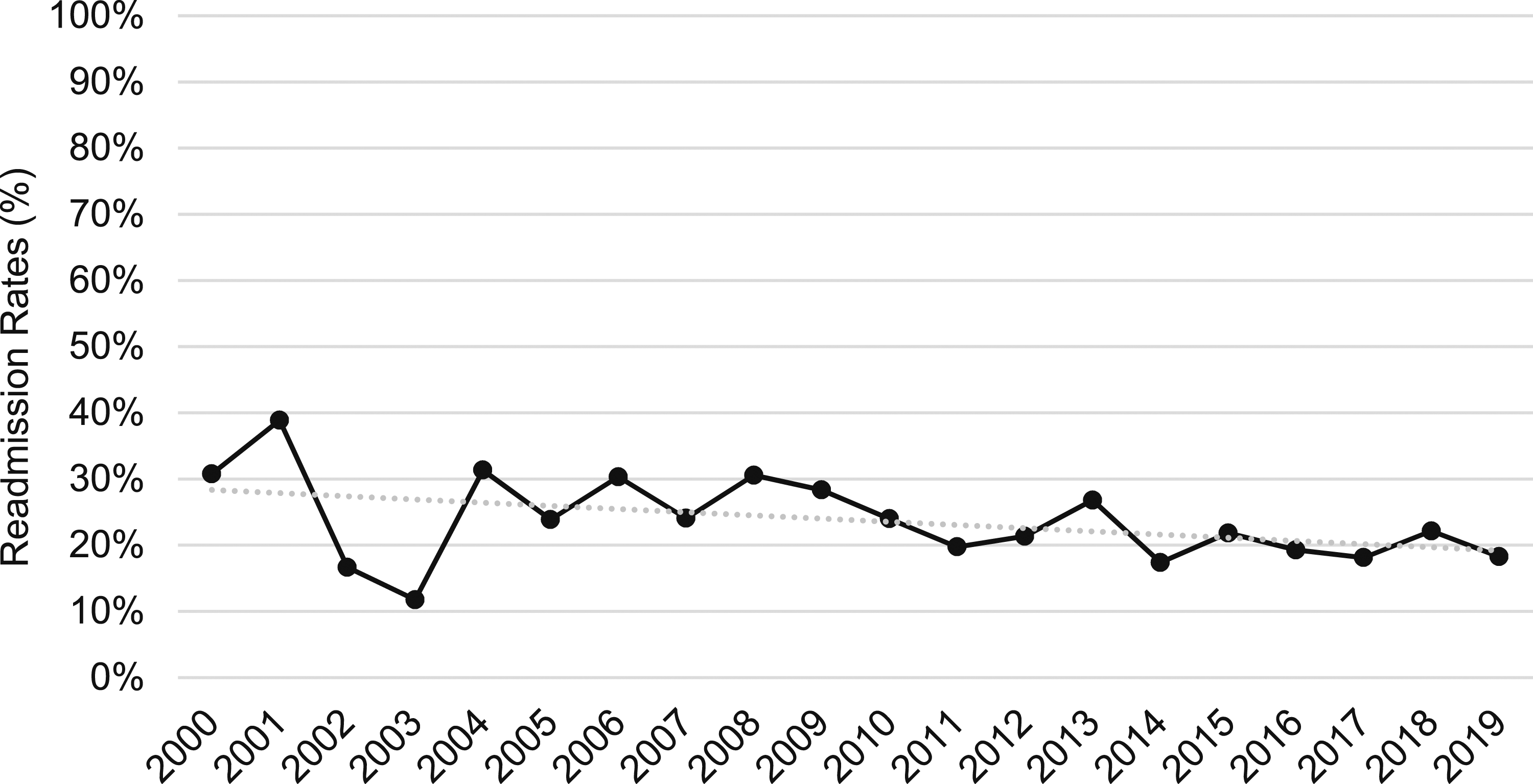
Logistic Regression for Postoperative Surgical Site Infections.
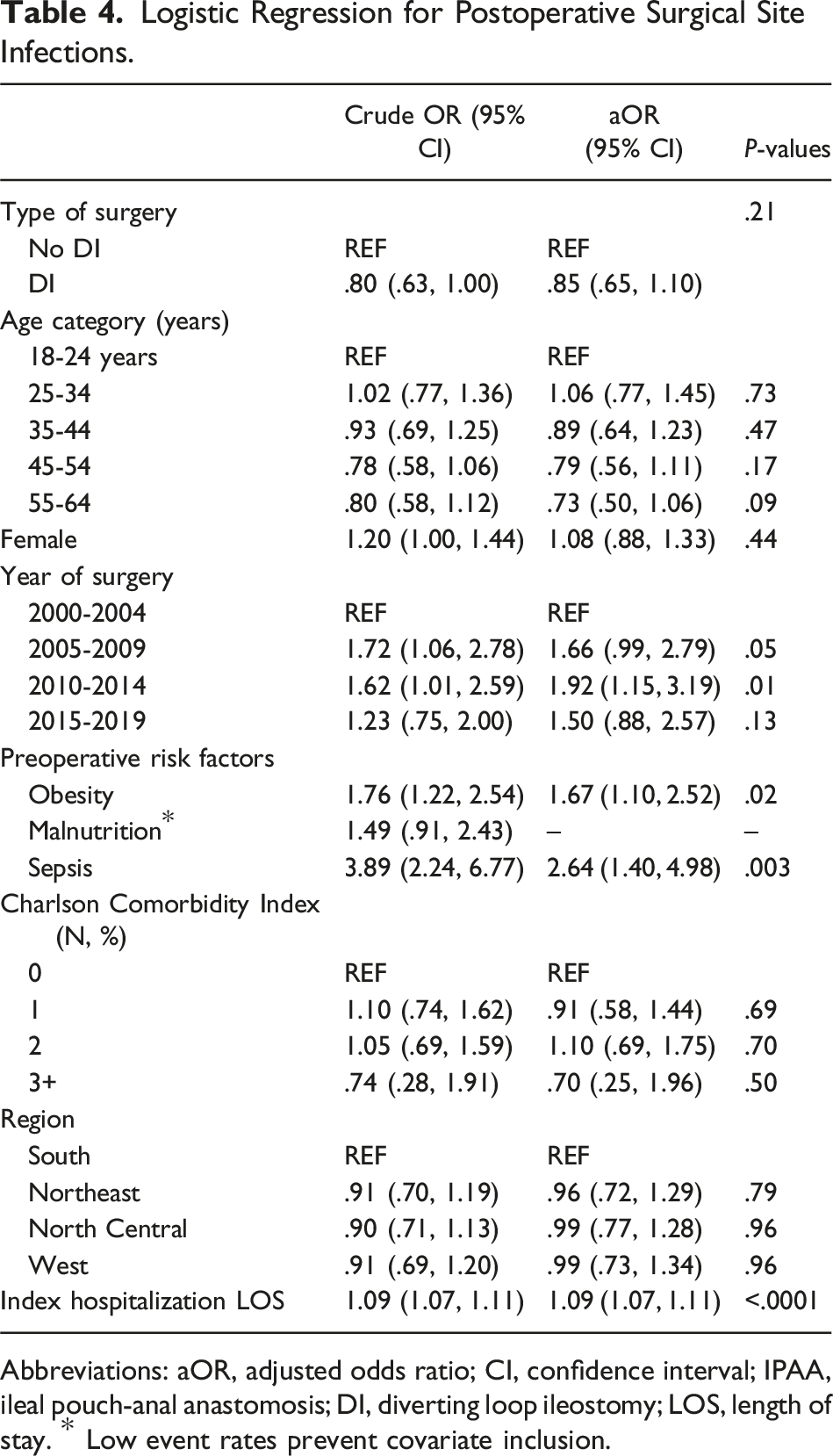
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; IPAA, ileal pouch-anal anastomosis; DI, diverting loop ileostomy; LOS, length of stay. * Low event rates prevent covariate inclusion.
Discussion
This study uses a national commercial insurance claims database to examine a population of adult patients with UC undergoing IPAA over a 20-year period. The population captured is one of the largest populations of IPAA patients described in the literature. Although patients that were diverted at the time of IPAA had a shorter index length of stay, postoperative outcomes did not significantly differ between groups. Additionally, the presence of a diverting ileostomy at the time of IPAA did not independently change the likelihood of readmission nor postoperative surgical site infection. There were regional differences in stoma creation rates, but the percentage of patients undergoing diversion during IPAA has remained stable over the last 20 years. In both cohorts and in the total population, readmission rates for patients undergoing IPAA have significantly declined over time.
The modified two-stage IPAA involves the creation of the pouch at the second stage without the formation of a diverting ileostomy. A meta-analysis including 10 studies and 1727 patients who underwent IPAA for UC showed no difference in leak rates between adults diverted at the time of IPAA and those who were not. 12 Widmar et al looked at long-term pouch outcomes in patients who underwent IPAA with and without diversion. 13 They found that symptomatic leaks were identified earlier in non-diverted patients and often could be addressed during index admission. However, long-term pouch functioning remained the same between diverted and non-diverted patients.
Diverting ileostomy after IPAA is intended to prevent pelvic sepsis after a pouch leak by limiting contamination from the leak. As such, a leak which would only require an intra-abdominal drain placement in a diverted patient may require a return to the operating room in a non-diverted patient. To capture all pouch leaks regardless of clinical severity, this study included 1) reoperations within 30 days, 2) intra-abdominal drainage procedures, and 3) ICD coding for organ space surgical site infections. Unfortunately, the granular data needed to determine which of these constituted a pouch-associated leak is unavailable in an administrative data set; however, any bias within this data set would bias the data toward overcounting rather than undercounting these critical complications. These findings support the clinical judgement of surgeons performing IPAA with or without DI and provide baseline data from which future prospective studies to determine which patients are most likely to benefit from DI and which may safely avoid diversion can be designed.
In the data from this study, IPAA without diversion was not associated with increased postoperative SSI. Previous studies have also demonstrated that clinical anastomotic leaks in non-diverted patients did not lead to increased reoperations, pouch failures, or fistula.14,15 One meta-analysis of 4973 cases demonstrated that reoperation was higher in patients without DI but that anastomotic strictures and pouch failures were higher in patients with DI. 10 In the pediatric UC population, Chen et al found that non-diverted patients had increased complication rates when complications were considered in aggregate (64.7 vs 15%, P < .01). 16 However, there was no difference in individual complications, including anastomotic leak, bleeding requiring transfusion, or small bowel obstruction. Between the study cohorts, there were no differences in rates of readmissions or reoperations, which held when stratifying for steroids or biologics. Despite these findings, in any retrospective study comparing non-diverted and diverted patients, there is inherent surgeon selection when determining whether a patient would benefit from diversion. These selection factors range from preoperative medication and nutrition considerations to intraoperative evaluation of tissue quality, all of which require a level of data that are difficult to capture yet likely impact postoperative outcomes.2,3
In this study’s population, 82.2% of patients were diverted at the time of IPAA. Data from the National Surgical Quality Improvement Program (NSQIP) registry has demonstrated that the proportion of emergency surgery for ulcerative colitis has been decreasing significantly in the last several years, from 21% in 2006 to 8% in 2018. 17 These findings likely demonstrate advancements in medical therapy for severe cases and breakthrough flares of UC, and may partially explain the significant decrease in readmission rates for both diverted and non-diverted patients over the study years. Another explanation for the steady decrease in readmission rates may be the increased utilization of Enhanced Recovery After Surgery® (ERAS®) bundles.18-20
Despite the changes in medical therapy and standardization to perioperative care over the 20 years examined, the diversion rate at the time of IPAA was unchanged. This points to a strong institutional and cultural preference for diversion practices, as many centers use consistent criteria for diversion. 3 The reported rate of stoma creation is highly variable in the literature and institution-dependent, with diversion rates in retrospective populations as low as 32.1% and as high as 86.1%.13,14
There is heterogeneity in institutional practices for diversion and the populations selected for study, but common findings have emerged when comparing patients with and without diverting ileostomy. 21 Patients that are not diverted have longer index hospitalizations. Ileostomy creation always necessitates a second surgery and admission for ostomy closure. Reversal carries its own risk of morbidity, with one study reporting a complication rate of 14.6% with ileostomy closure.4,22,23 Given the extensive range of diversion practices and consistent rate of diversion over the past 20 years, it is likely that too many ulcerative colitis patients are still being diverted, without clear evidence that this is benefiting patients in the long run.
There are limitations to this analysis. MarketScan® comprises private payors; therefore, this sample does not include self-pay, Medicaid or Medicare patients, and other non-employer sponsored coverage that may have different outcomes. This payor mix introduces selection bias, which may not make the results generalizable to other populations. Additionally, MarketScan® does not have data for every patient with a given procedure code but instead provides a large, representative sample. 24 This could result in further selection bias.
Additionally, preoperative medications were not included as part of the analysis. Colorectal and ulcerative colitis studies have reported a dose-related risk of pouch complications with steroid use. 25 Using this database, the dosage and duration of steroid treatment prior to IPAA could not be stratified. The impact of biologics on preferred surgical approach—whether to divert patients during IPAA—has not been conclusive.26,27 One meta-analysis found that patients exposed to biologics that underwent a modified 2-stage IPAA without diversion had better outcomes than traditionally diverted patients. 12 The authors suggest this could be because of increased healing time after colectomy before IPAA creation. In a multicenter, prospective study including patients with UC and Crohn’s disease, Cohen et al found that preoperative exposure to tumor necrosis factor inhibitors was not associated with an increased risk for postoperative complications. 28
The method of cohort assignment in this study was defined based on ostomy takedown within 1 year. Therefore, there may be a small group of patients that remain diverted after 1 year but were assigned to the non-diverted cohort. This portion of patients is likely small but would bias findings towards the null. Lastly, some short-term complications seen in this study may have long-term effects on pouch function and inflammatory conditions, neither of which are evaluated here.
Conclusions
Forgoing diversion at the time of IPAA saves the patient from a second hospitalization, surgery, and morbidity of an ostomy. In this study, patients without diversion have a longer index hospital stay but did not have significant differences in postoperative outcomes. Across this 20-year sample, the rate of ileostomy creation at the time of IPAA was unchanged, with significant regional differences in diversion practices. However, readmission rates in both populations have declined steadily since 2000. In adult UC patients undergoing IPAA, there remains a need for individualization when deciding to perform diversion.
Footnotes
Author Contributions
U.C.A.: Conceptualization, methodology, validation, formal analysis, data curation, writing—original draft, writing—review and editing, and visualization. C.B.A.: Methodology, software, validation, formal analysis, data curation, and visualization. E.L.B.: Conceptualization, writing—original draft, writing—review and editing, and supervision. J.M.S.: Conceptualization, methodology, validation, writing—review and editing, and supervision. A.G.C.: Data curation, writing—original draft, writing—review and editing, and supervision. M.R.P.: Conceptualization, methodology, validation, data curation, writing—original draft, writing—review and editing, visualization, and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.