
Abstract
Objectives:
Temporary abdominal closure methods allow for management of open abdomens where immediate primary closure is not possible and/or where repeat abdominal entries are necessary. We assessed pressure mapping and fluid extraction efficiency of three open abdomen dressing systems: ABThera™ Active Abdominal Therapy System, V.A.C.® Abdominal Dressing System, and Barker’s vacuum packing technique.
Methods:
An in vitro test model was designed to simulate physical conditions present in an open abdomen. The model consisted of a rigid rest platform with elevated central region and a flexible outer layer with centrally located incision. Constant −125 mmHg negative pressure was applied according to the type of system, under simulated dynamic conditions, using albumin-based solution with a viscosity of 14 cP. Data were collected by pressure sensors located circumferentially into three concentric zones: Zone 1 (closest to negative pressure source), Zone 2 (immediately outside of manifolding material edge), and Zone 3 (area most distal from negative pressure source). Each value was the result of approximately 100 pressure readings/zone/experiment with a total of three experiments for each system.
Results:
Pressure distribution of ABThera Therapy was significantly (p < 0.05) superior to Barker’s vacuum packing technique in all three evaluated zones. Similarly, V.A.C. Abdominal Dressing System pressure distribution was significantly (p < 0.05) improved compared to Barker’s vacuum packing technique in all zones. There were no pressure distribution differences in Zone 1 between ABThera Therapy and V.A.C. Abdominal Dressing System; however, in Zones 2 and 3, ABThera Therapy was significantly (p < 0.05) superior to V.A.C. Abdominal Dressing System.
Conclusions:
These data suggest that all approaches to negative pressure therapy for open abdomen treatment are not equal. Additional research should be conducted to elucidate clinical implications of data demonstrated here.
Introduction
Delayed primary closure and management of the open abdomen (OA) continue to pose significant challenges for surgeons. Definitive closure of the abdominal fascia and wall immediately following a laparotomy may be technically impossible or medically contraindicated due to increased intra-abdominal pressure (IAP). Management of the OA patient continues to present clinicians with challenges that make the care of the already critically ill patient one of the most complex in modern medicine. The large abdominal opening resulting from an emergent laparotomy leads to challenges in fluid balance as well as complications associated with environmentally exposed bowel. Some complications associated with OA patients include infection, edema, fistulas, and pulmonary, liver, renal, and other organ dysfunctions. 1
Prolonged abdominal viscera exposure can result in high rates of complications including, but not limited to, fluid loss, dehydration, hypovolemic shock, bowel adhesions, perforation, fistula formation, infection, sepsis, multiple organ dysfunction syndrome (MODS), and death.2,3 With elevated IAP, the compliance of the chest wall and total respiratory system is decreased. The lung compression effects of increased IAP may lead to a loss of lung volume with atelectasis. 4 They may require prolonged periods of ventilator support, which can be associated with other morbidities. In addition, the post-injury hyper-inflammatory response poses further challenges for patients and their treating clinicians. 5
In the event that a surgeon is unable to close an abdomen at the end of a procedure, he or she may use one of several temporary abdominal closure (TAC) techniques that remain in place for a number of hours, days, or weeks, until the abdomen can be safely closed.6–12 The etiology that necessitates OA management may include surgical exploration for abdominal trauma, abdominal sepsis, and relief of abdominal compartment syndrome (ACS). 3 An ideal OA management TAC approach would facilitate ease of re-exploration, control of abdominal contents, and reduction of the risk of intra-abdominal hypertension (IAH) and resultant ACS, while preserving fascial domain for future closure of the abdominal wall. 1 The optimal TAC technique would also allow physicians to achieve primary fascial closure (PFC) earlier, thereby reducing the time that the abdominal wall remains open, the number of operating room (OR) trips for repeated attempts at closure, and potential complications and morbidities associated with such procedures. It would also reduce prolonged intensive care unit (ICU) and hospital stays and therefore potentially reduce total costs of associated care. 3
The objective of this study was to assess the negative pressure distribution of three OA dressing systems.
Methods
In this study, we investigated the pressure mapping and fluid extraction efficiency of three TAC techniques in a simulated abdominal bench test. The TACs evaluated were (1) Barker’s vacuum packing technique (BVPT), consisting of one sterile manually perforated non-adherent polyurethane drape, two sterile surgical towels, two Jackson Pratt (JP) drains, one Ioban adhesive drape, and one external vacuum source; (2) V.A.C.® Abdominal Dressing System (VADS; KCI, San Antonio, TX) consisting of one sterile pre-perforated non-adhesive polyurethane drape, one polyurethane open cell abdominal foam, four adhesive drapes, one vacuum tubing with track pad, and one negative pressure wound therapy (NPWT) pump; and (3) ABThera™ Active Abdominal Therapy System (ABThera Therapy; KCI, an Acelity company, San Antonio, TX) consisting of one visceral protective layer (VPL), two polyurethane open cell abdominal foam, four adhesive drapes, one vacuum tubing set with T.R.A.C.™ Pad, and one ABThera negative pressure therapy (NPT) pump.
All three TAC techniques were evaluated for pressure mapping and fluid extraction efficiency using a bench model created to simulate OA conditions in a controlled environment. This test set-up (Figure 1) consisted of a 48″ × 48″ rigid polycarbonate plate with a silicone dome in the center simulating the distended abdominal area. Thirty pressure transducers were placed through the polycarbonate plate in three concentric circles around the silicone dome and one centrally located, in order to record pressures in real time during the simulated therapy time. An analog data acquisition system was used to record real-time pressure measurements from all pressure transducers simultaneously. A peristaltic pump was used to pump a simulated abdominal wound fluid into the model at a rate of 1000 mL/h. Upon initiation of the test, all systems were pre-filled with 1 L of simulated wound fluid simulating accumulation of wound fluid in the abdominal cavity prior to therapy initiation. The simulated wound fluid was an albumin-based solution made to a viscosity of 14 cP. A calibrated scale was used to quantify the fluid being extracted from the model into the collection canister.
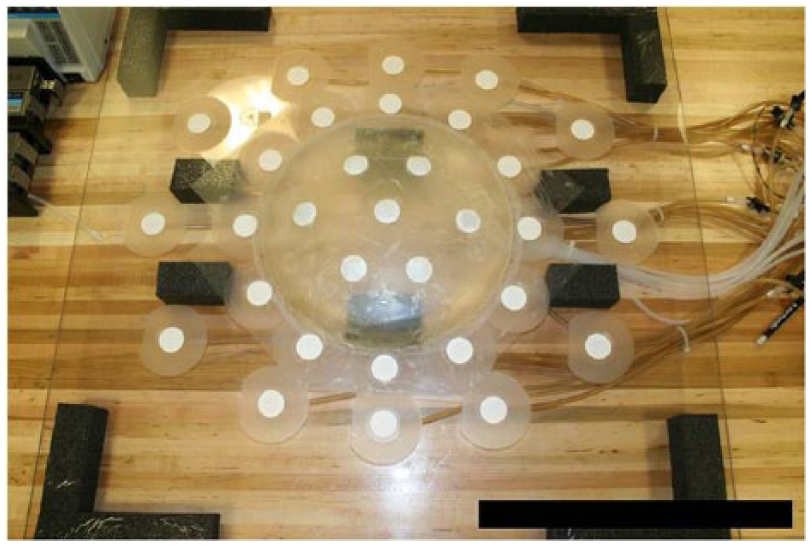
Model consisted of a rigid rest platform having an elevated central region and a flexible outer layer with a centrally located incision. The dressing was placed between the rigid and flexible layers and was sealed around the perimeter.
Each TAC technology was placed onto the abdominal simulated model just as it would be placed into an OA (Figure 2). Once the pre-loading of abdominal fluid was completed, the pressure sensors and acquisition system were started, and a baseline pressure measurement was collected. Upon verification of the baseline, the NPT and peristaltic infusion of simulated wound fluid were started simultaneously and real-time data collection began. The test was performed at room temperature for 30 min and repeated in triplicates. Both the pressure and simulated wound fluid data were collected and recorded.
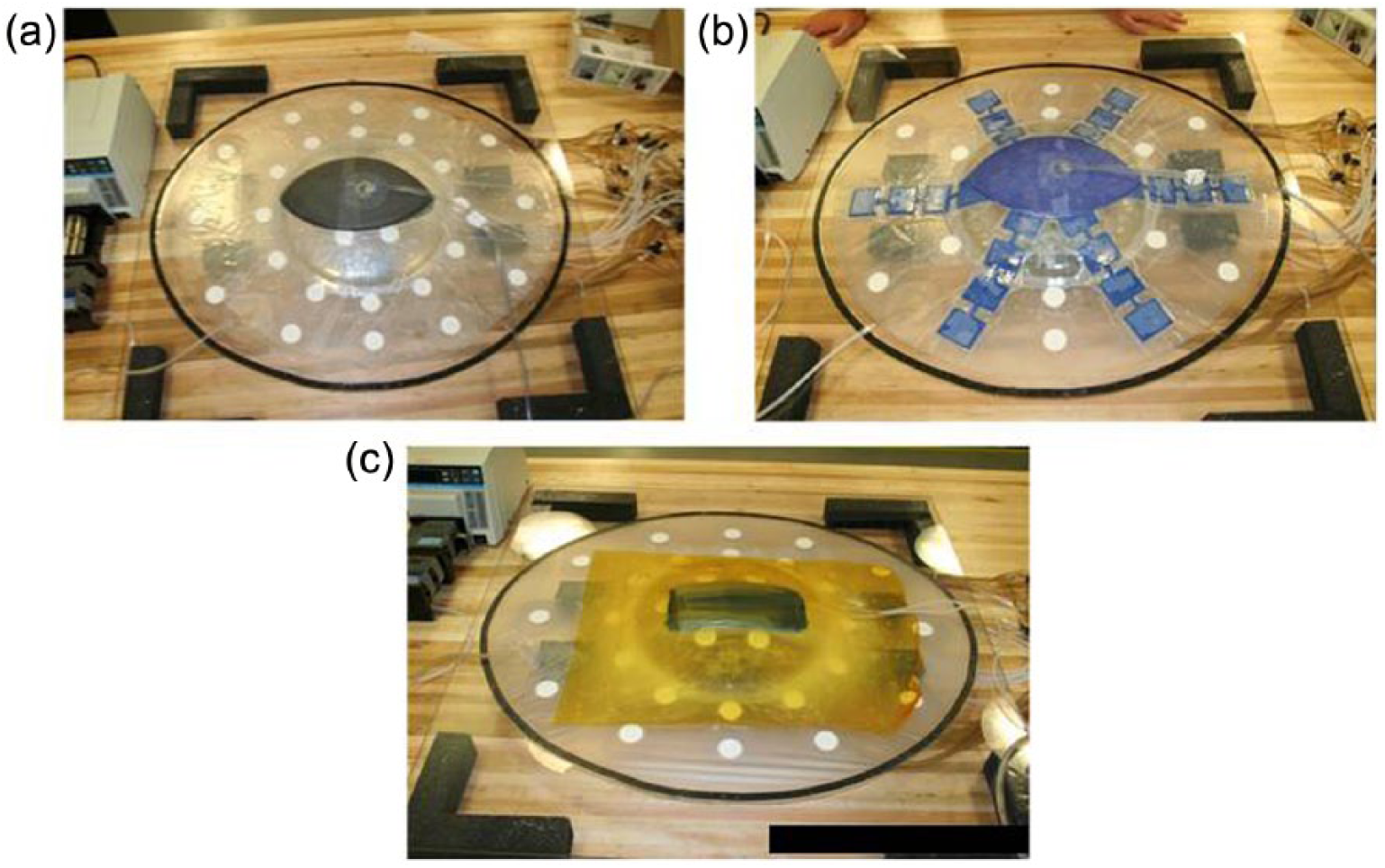
Depiction of all three TAC techniques on the bench testing model: (a) VADS, (b) ABThera™ Therapy, and (c) BVPT.
The pressure data were analyzed by averaging 10 readings from each pressure transducer for each area sensor and the averages of the triplicates calculated. Data collection topology is represented in Figure 3.

Depiction of all three TAC techniques’ data collection topology: (a) VADS, (b) ABThera™ Therapy, and (c) BVPT.
As represented in Figure 3, the data collection pressure sensor arrays were defined within the test model in concentric zones and were defined as:
Zone 1(a): sensor 31—representative of the TAC center point, directly below the interface pad used to connect the dressing system to the therapy unit (negative pressure source).
Zone 1(b): sensors 25–30—representative of the inner circle of the TAC (directly under the manifolding material).
Zone 2(a): sensors 14, 16, 18, 20, 22, and 24—representative of the middle circle of the TAC (immediately outside (adjacent) the manifolding material but still directly under open cell foam extensions on ABThera VPL).
Zone 2(b): sensors 13, 15, 17, 19, 21, and 23—representative of the middle circle of the TAC (immediately outside (adjacent) the manifolding material and in between the open cell foam extensions on ABThera VPL).
Zone 3(a): sensors 2, 4, 6, 8, and 12—representative of the outer circle of the TAC (furthest outside the manifolding material but still directly under open cell foam extensions on ABThera VPL).
Zone 3(b): sensors 1, 3, 5, 7, and 11—representative of the outer circle of the TAC (furthest outside the manifolding material and in between the open cell foam extensions on ABThera VPL).
The analysis was based on trying to answer four principal research questions: (1) Is there a significant difference in mean pressure among the three different dressing configurations when considering the area directly underneath (covered) the pressure manifolding material (open cell foam or sterile towels)? (2) Is there a significant difference in mean pressure among the three different dressing configurations when considering the area not directly underneath (covered) the pressure manifolding material (open cell foam or sterile towels)? (3) Is there a significant difference in mean pressure among dressings described by the three concentric zones? (4) Is there a significant difference in the number of equally spaced apart sensors directly underneath (covered) the pressure manifolding material (open cell foam or sterile towels)? Data were subjected to statistical analysis based on the zones and grouping of sensors and their relative position to the negative pressure source. The statistical analysis model used for answering the four principal research questions was as follows:
Research Question 1. Data analysis consisted of a one-factor analysis of variance (ANOVA), using the pressure readings recorded across the sensors covered by manifolding material for each respective TAC configuration. Pressure readings across triplicates served as a dependent variable.
Research Question 2. Data analysis consisted of a one-factor ANOVA, using the pressure readings recorded across the sensors not covered by manifolding material for each respective TAC configuration. Pressure readings across triplicates served as a dependent variable.
Research Question 3. Data analysis consisted of a one-factor ANOVA, using the pressure readings recorded across the sensors associated with each concentric circle (zones). Pressure readings across triplicates served as a dependent variable.
Research Question 4. Data analysis consisted of a 2 × 3 Fisher’s exact test, comparing proportions for each dressing configuration.
All comparisons were evaluated utilizing a significance level or alpha of 0.05. The Tukey–Kramer method was used to adjust for multiple comparisons. In addition to pressure data analysis, we evaluated the fluid extraction efficiency of all three TACs. We were able to quantitatively compare the volume and flow rates for all three TACs as indicators of TAC efficiency.
Results
Overall results of the data demonstrated that pressure distribution of ABThera OA Dressing (ABThera Therapy) and VADS were both significantly (p < 0.05) higher than BVPT in all three evaluated zones (Table 1). There were no differences in Zone 1 between ABThera and VADS, but ABThera was significantly (p < 0.05) higher than VADS in Zones 2 and 3 (Table 1).
Summary table for pressure mapping by zone of interest.

SEM: scanning electron microscopy; VADS: V.A.C.® Abdominal Dressing System; BVPT: Barker’s vacuum packing technique.
The data also demonstrated a higher efficiency in fluid removal both in total volume and flow rate. The final extracted volume was calculated at the 30-min time point of data collection. The final volume was as follows: ABThera Therapy, 0.802 ± 0.02 L; VADS, 0.628 ± 0.01 L; and BVPT, 0.582 ± 0.09 L. The graphical representation of the volume comparison is presented in Figure 4.
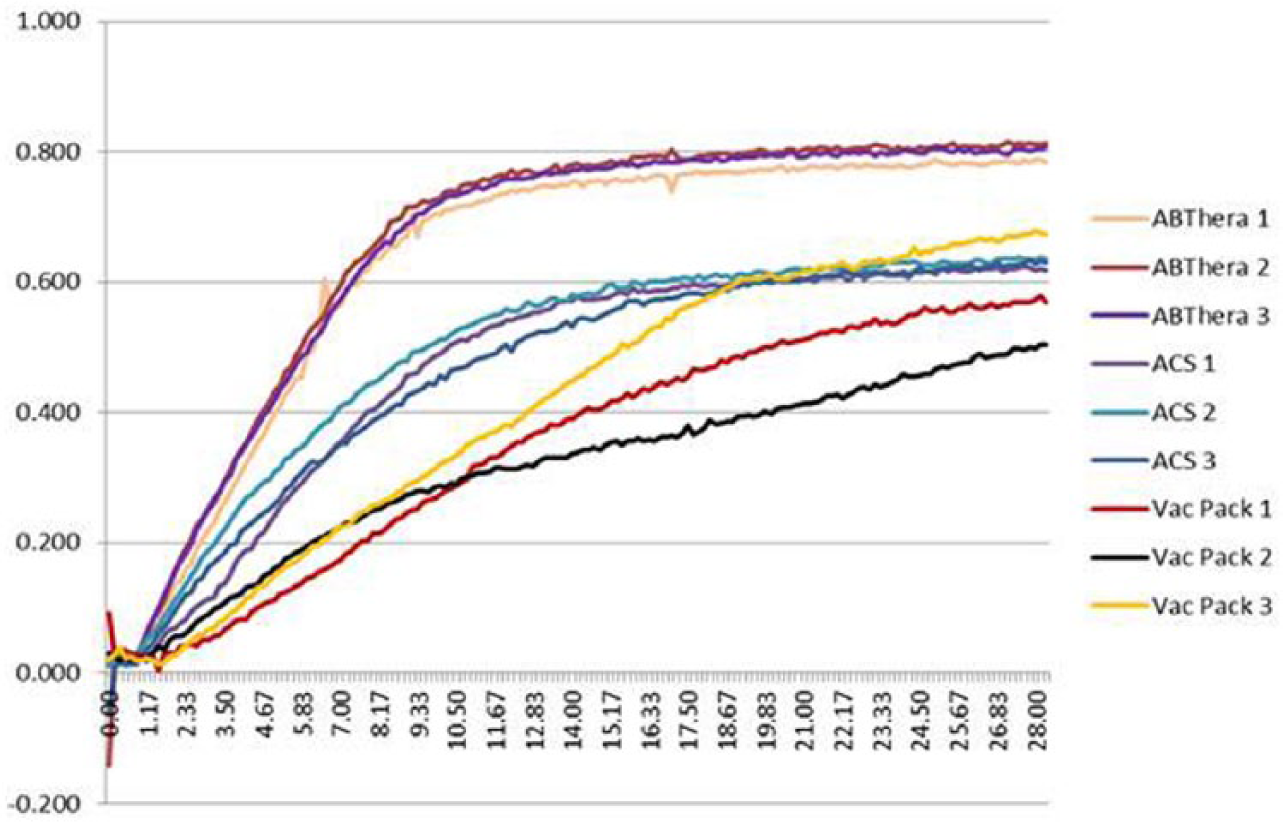
Graphical representation of volume extraction for TACs in triplicates.
Final volume analysis showed ABThera Therapy was significantly (p ⩽ 0.05) higher than VADS and BVPT. The reproducibility of volume extraction can also be seen in Figure 4, where both ABThera Therapy and VADS demonstrated no statistical difference between each triplicate run while BVPT showed a significant (p ⩽ 0.05) difference between triplicate runs. The volume extraction rates were also analyzed. The rate of ABThera Therapy was 93 mL/min and was significantly (p ⩽ 0.05) higher than both VADS at 61 mL/min and BVPT at 34 mL/min (Figure 5). VADS was also significantly (p ⩽ 0.05) higher than BVPT.

Graphical representation of volume extraction rates for all TACs.
Discussion
The management of patients with an OA is an evolving concept that has been improving over time. The inventions of new techniques to manage the OA as well as the techniques used to manage the physiological sequela after trauma are constantly under evaluation. This bench study attempted to evaluate the techniques and products currently used in trauma/surgery for managing OAs. In this evaluation, we closely examined two established techniques for open abdomen management (OAM) and one new emergent approach to OAM. In this study, we evaluated the performance of these TACs side by side, in a clinically relevant bench model. The results indicate that ABThera Therapy proved to be the most efficient approach to OAM in relation to the four main parameters investigated in this study: pressure delivery, fluid volume removal, fluid flow rate, and reproducibility of treatment.
As we look into the goals of what OAM should provide, we are interested in protection of the visceral content, management of incisional domain, and intra-peritoneal fluid removal. It has been demonstrated through the years that something as simple as a sterile intravenous (IV) bag can provide visceral content protection. Similarly, incisional domain has been addressed by surgeons with simple techniques, such as sutures, bindings, and clamps. On the other hand, removal of intra-peritoneal fluid remains as one of the most challenging aspects of OAM. Recent data [bench (Barlos et al. 13 ) and animal (Kubiak et al., 14 Bochicchio et al., 15 and Cheatham et al. 16 )] linking the effects of intra-peritoneal fluids and their effects on hyper-inflammatory response within the visceral content have made this aspect of OAM one of the most critical endpoints of treatment.13–16 With this in mind, we have concentrated the efforts of this study to demonstrate the differences among these three techniques currently used in the OAM as to their properties associated with fluid removal.13–15,17
The key to intra-peritoneal fluid removal has been NPT applied to the abdominal cavity in order to vacuum out the fluid. All of the approaches studied here utilize NPT as the principle of OAM.2,3,14,15,18–23 With this in mind, the efficiency of NPT delivery is paramount in the successful delivery of therapy when managing the OA. In this study, we evaluated the performance of these TACs side by side, in a clinically relevant bench model. The results indicate that ABThera Therapy proved to be the most efficient approach to OAM. This was demonstrated by four main parameters investigated in this study: pressure delivery, fluid volume removal, fluid flow rate, and reproducibility of treatment.
The first parameter is pressure delivery and is considered the most important since all other parameters of the TACs are dependent on this. In the evaluation of pressure delivery, the challenge has always been on how to deliver the target pressure to areas of dependency far away from the NPT source. It is well known that as the distance increases from the NPT source the pressure drops. Also, the inversely proportional relationship of pressure and fluid removal makes this facet of OAM a challenging one. In this study, we challenged the three TACs to the extreme using a high-viscosity, but clinically relevant, fluid. This fluid was a simulated wound fluid with a composition similar to that of naturally occurring intra-peritoneal fluid. It was clear by the data that as soon as the distance from the TAC’s pressure source increased the pressure dropped. Also, the pressure was reduced by the type of material used as the manifolding material. In the BVPT, we saw a marked reduction of pressure at the manifolding material area (Zone 1). We postulated that this was directly related to the use of cotton fiber–based towels as the manifolding material. In contrast, we observed a much lower dampening of pressure when open cell foam was used as the manifolding material. Obviously, due to the relationship of pressure and fluid movement, as the pressure increases, more fluid can be reomved quickly. Also, as the amount of fluid increases or the viscosity of the fluid increases, the higher the pressure required to remove such fluid.
As illustrated in Figure 6, the open space provided by these two materials is the key to the pressure manifolding. The gauze-based material is 90% open space at atmospheric pressure, but once NPT is applied, the material collapses the fibers and the open space is reduced to approximately 6%. It takes −200 mmHg of pressure to fully occlude the material (unpublished data). This reduces the open space available for the fluid to move through. Also, the small fibers of cotton that come in contact with the open spaces increases the resistance of the fluid as it moves, reducing the velocity of the fluid through the open space. On the other hand, open cell foam is 98% open space at atmospheric pressure, but at −200 mmHg, it is 75% open space (unpublished data). This allows for open movement of fluid through the fully collapse material. The open cell foam does not contain any fibers that would increase the resistance of the fluid, allowing for optimal fluid velocity through the material. The comparison of these two materials can be seen in Figure 6.
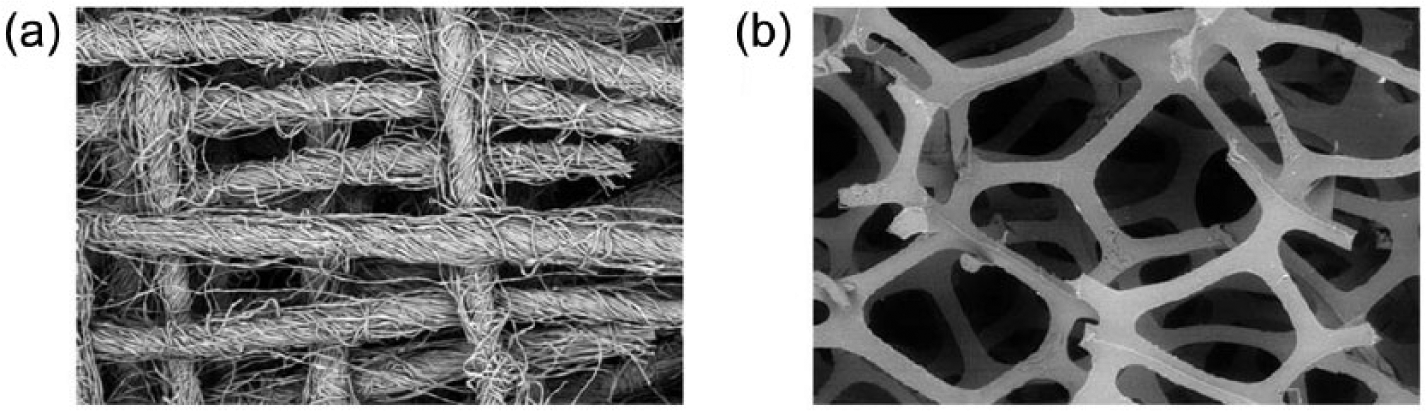
Electron micrographs of (a) cotton-based towels and (b) open cell foam demonstrating void space for fluid movement.
Another aspect of pressure manifolding that was evident in this study was the fact of the design of the evaluated techniques. When looking at the pressure distribution across the three TACs, it is obvious that the goal of the ABThera VPL design was to provide better pressure manifolding to areas distal from the NPT source (Zones 2 and 3). The data clearly showed the drop in pressure once measurements were made outside the manifolding material for all TACs. The original design of the VADS was to generate a ready-to-use system that would provide OAM similar to that of the BVPT, which was the standard of care (SoC) at the time. As the data show, there was no major difference in the performance of the VADS over the BVPT other than achieving a higher flow rate by changing the manifolding material and the reproducibility of treatment delivery. The new design of the ABThera VPL builds on the notion of extending the manifolding material into the distal areas of the abdomen, where fluid tends to accumulate in the more dependent areas. By extending the manifolding material via the arms of the VPL, higher pressures can be delivered to areas that were previously inaccessible by the VADS or BVPT. This was evident by recorded pressures in most distal areas of the ABThera dressings (Zone 3) compared to the same zone in the other TACs. Similarly, the pressures in Zone 1 compared to Zones 2 and 3 within each TAC were evaluated. It is clear that the new ABThera design has improved the NPT delivery, increasing the efficiency of OAM.
The next two parameters, fluid volume and flow rate, can be discussed in the same context since they are two aspects of fluid extraction. The increased efficiency on pressure delivery to the abdomen translates into improvements in fluid volume extraction and fluid flow rate. With higher pressures applied to the abdomen, more fluid can be removed faster. The data clearly show the increased volume removed by ABThera Therapy compared to VADS and BVPT. One interesting point to discuss is that the dressing was evaluated with 1 L of 14 cP fluid. In the 30-min volume determination, it was recorded that both BVPT and VADS removed 0.582 ± 0.09 L and 0.628 ± 0.01 L, respectively, while ABThera Therapy removed 0.802 ± 0.02 L. One observation that the data do not show is that when we examined the model after the completion of the experiment, both the VADS and the BVPT had fluid remaining in the model (about 0.3 L), while with ABThera Therapy, there was no residual fluid in the model. Upon further evaluation, we weighed the manifolding material for all three TACs in order to determine the amount of fluid contained within the dressings. Both the VADS and the BVPT contained approximately 0.1 L of fluid within the manifolding material, while the ABThera Therapy contained 0.2 L of fluid. Since ABThera Therapy removed 0.8 L out of the model and contained 0.2 L within the dressing, this explained the fact that there was no residual fluid in the model at the conclusion of the experiment. Both the VADS and the BVPT left fluid behind in the model.
The final parameter evaluated in this study was the reproducibility of treatment. When each one of these TACs was used in this model, a variance in the data collected was noted. This variance was very small in both ABThera Therapy and VADS. The variance in the BVPT was of notable difference and was of concern since every time we want to provide such therapy to a patient, we want a level of consistency in the therapy outcome. The differences in the BVPT are due to the fact that this technique was based on products readily available in the OR and were not controlled. For example, the folding of the towels as manifolding material is never the same. Thus, the alignment of fibers creating void space is never consistent. The manner in which the non-adhesive layer is fenestrated with a scalpel, creating fenestrations of various sizes and geometries, the way in which the drains are positioned, and the amount of relative wall suction used all contribute to variance. No two patients using BVPT get the same therapy. On the other hand, both the VADS and the ABThera Therapy are products manufactured under a set of quality standards based on a good manufacturing process. This ensures that every dressing is controlled to a set of specifications designed to provide a therapy within a set of performance parameters.
In summary, the data presented here demonstrate that not all approaches to negative pressure therapy for treatment of the OA are equal. The ABThera Therapy data support significant improvement in the development of a TAC device to manage the OA. All parameters evaluated in this study (pressure delivery, pressure distribution, fluid removal, and performance consistency) demonstrated that the ABThera Therapy system was the superior TAC. In addition to the recommendations of the World Society of Abdominal Compartment Syndrome 24 and the more recent studies on the OA,16,25,26 more research should be conducted to clearly elucidate the clinical implications of the data demonstrated here.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Delgado is an employee of Acelity (San Antonio, TX).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.