
Abstract
Background and aims:
The aim of this study is to examine the clinical and functional outcome of laparoscopic posterior rectopexy in a consecutive series of adult patients with full-thickness rectal prolapse.
Material and methods:
Preoperative data on demography, life-style practices, medication, comorbidity, and previous surgery for rectal prolapse were ascertained from patient charts. Information on operative procedure, and pre- and postoperative complications were recorded. Short- and long-term follow-up were done after a median of 60 days and 2 years after surgery.
Results:
Between 1 February 2009 to 1 June 2012, 81 laparoscopic posterior rectopexies were done. Male-to-female ratio was 4:77, median age 73 [57–80.5] years and median ASA Grade 2. Conversion to open surgery was done in 6.2%, the median operating time was 82 min [66 - 102] and median length of hospital stay was 2 days [2–5.7]. Minor and major complications were seen in 5.3% and 14.8%, respectively. The 30-day mortality rate was 1.2%. Constipation or incontinence improved or disappeared in 65.2% and 74.4%, respectively. The cumulated recurrence rate was 11.1% after a median observation time of 2 years.
Conclusion:
Laparoscopic posterior rectopexy is a safe and well-tolerated procedure in older patients and can be done with acceptable complications and recurrence rates and short hospital stays. Laparoscopic posterior rectopexy seems to improve bowel function in many patients.
Introduction
Rectal prolapse is a circumferential protrusion of all layers of the rectum through the anal sphincter. It can be classified into complete full-thickness rectal prolapse (FRP) or incomplete thickness prolapse, also referred to as intussusception or internal prolapse. FRP mostly affects older women. The only effective treatment is surgical, but since patients are often elderly, they frequently suffer from comorbidity that could contraindicate major abdominal surgery.
An overwhelming number of transabdominal and perineal surgical techniques have been described for the treatment of FRP and the choice of treatment varies substantially between countries (1, 2). Transabdominal procedures are performed through laparotomy or laparoscopy and often include rectal mesh fixation. These procedures were thought to provide more effective repairs with lower recurrence rates than perineal approaches, but recent data suggest that recurrence rates are much higher than previously thought (3). Perineal approaches can be done in regional or local anesthesia and have been reserved for frail patients and patients with intussusception and small FRP to lower the risks inherent to laparotomy and general anesthesia. Recurrence after perineal procedures varies between 0 and 44% (3–5). Improvement in incontinence and constipation may be higher in patients undergoing abdominal procedures (3, 4, 6).
Laparoscopic posterior rectopexy (LPR) for the treatment of FRP was introduced in the early 1990s. More recently, anterior laparoscopic rectopexy has gained increasing interest (7), but no randomized studies have examined, if this approach results in better outcome than LPR. Large-scale randomized trials have been eagerly awaited, but recently the large-scale prosper trial was terminated prematurely due to slow accrual of patients (3).
The purpose of this study was to examine if LPR is a safe and feasible method for the treatment of FRP in a consecutive series of patients and to assess the short- and long-term recurrence rates and changes in functional outcome after LPR.
Material and Methods
Study Design
The study design included a retrospective chart review and prospective follow-up of a series of consecutive patients who underwent LPR from 1 February 2009 to 1 June 2012 in a tertiary center in Denmark.
Patient Selection, Pre- and Peroperative Assessment
All patients referred with a possible FRP were examined by a specialist in colorectal surgery. FRP was diagnosed with the patient placed in a straining chair as a circumferential protrusion of all rectal wall layers. LPR was the preferred procedure for patients with a FRP > 5 cm. High age, previous perineal or abdominal procedures for FRP, or a history of abdominal surgery was not an exclusion criterion. Patients with severe comorbidity and complicated former abdominal surgeries were offered perineal procedures.
Data on age, gender, and preoperative functional symptoms or discomfort: constipation (yes, no), incontinence (yes, no), size of the prolapse (cm), smoking (yes, no), alcohol intake (normal, abuse), NSAID or prednisolone treatment (yes, no), former prolapse surgery (yes, no, type), abdominal surgery (no, upper, lower), and comorbidity (pulmonary, cardiovascular disease, diabetes, cancer, or other chronic diseases) were obtained from medical charts. Data on peroperative complications and conversion to open surgery were extracted from patient files. Information on American Society of Anesthesiologists (ASA) score, body mass index (BMI), operating time, and need for transfusion was retrieved from an electronic surgical registration system (Orbit). Operating time was defined as time from skin incision to skin closure. Peroperative complications included bowel lesions or bleeding defined as vascular lesions requiring suturing, long time electro-cautery, use of vaso-sealing materials, or need of peroperative transfusion. Reasons for conversion to open surgery were recorded.
Operative Technique
LPR was done as a multiport laparoscopic posterior mesh rectopexy. Mesorectum was mobilized posteriorly from the sacral promontory to the pelvic floor. Lateral stalks were not divided. Bowel resection and circumferential division of the peritoneum was not done in this series. A T-shaped polypropylene mesh (Surgipro®, US Surgical, Norwalk, Connecticut) was placed with the vertical “leg” laying flush with the anterior surface of the sacrum, and secured to the promontory and sacrum with four to eight titanium tacks (ProTack®, Covidien, Norwalk, Connecticut). The mesh “wings” were sutured to the lateral sides of the rectum/mesorectum with two Gore-Tex sutures on each side. The visceral peritoneum was left open. The fascia in the 12 mm port sites was routinely closed with Vicryl™ 0, whenever possible. After the occurrence of the first port site hernias, extra efforts were made to ensure sufficient closing of the fascia in these port sites.
POSTOPERATIVE Complications and Length of Stay
Minor or major complications within 30 days after surgery were recorded. Major complications were those requiring admission more than 3 days, re-operation, blood transfusion, or resulting in death. Minor complications were incidents requiring antimicrobial or other medical therapy. Length of stay (LOS) was calculated from the day of surgery to the day of discharge.
Short-Term Follow-Up
Approximately 2 months after surgery, all patients were invited for an out-patient examination and asked about functional outcomes, that is, obstipation and incontinence (yes/no). Possible recurrences were confirmed by examination of the patient in a straining chair.
Long-Term Follow-Up
Patients operated before 1 June 2012 were contacted by telephone and asked about signs of recurrence, functional outcomes, that is, obstipation and incontinence (yes/no), and whether they were satisfied with the outcome. Telephone interviews were carried out between October 2012 and March 2013. A specialist in colorectal surgery invited patients, who reported a possible recurrence, for a re-examination. Furthermore, all patients were asked whether they had been admitted to hospital after surgery, and whether they felt that they could recommend the procedure to other patients.
Since this study is based on medical chart reviews and telephone interviews, approval from the ethical committee was not needed.
Cumulated Incidence of Rectal Prolaspe Recurrence
The cumulated incidence of rectal prolapse recurrence was calculated by adding the incidence of recurrence at short-term and at long-term follow-up.
Statistical Analysis
Calculations were done with the SPSS statistical software version 19. Continuous variables are given as medians and interquartile (IQ) ranges. Complication and recurrence rates are given as proportions with 95% confidence intervals. Comparisons of median values are done with the Mann–Whitney test and comparisons of proportions with cross-tabulations and chi-square test. P-values < 0.05 were considered significant.
Results
Study Population
Between February 2009 and 1 June 2012, 85 patients were scheduled for LPR. Three patients operated for intussusception were excluded. In one patient, the procedure was aborted because of peritoneal carcinosis, leaving 81 patients eligible for analyses (Fig. 1).
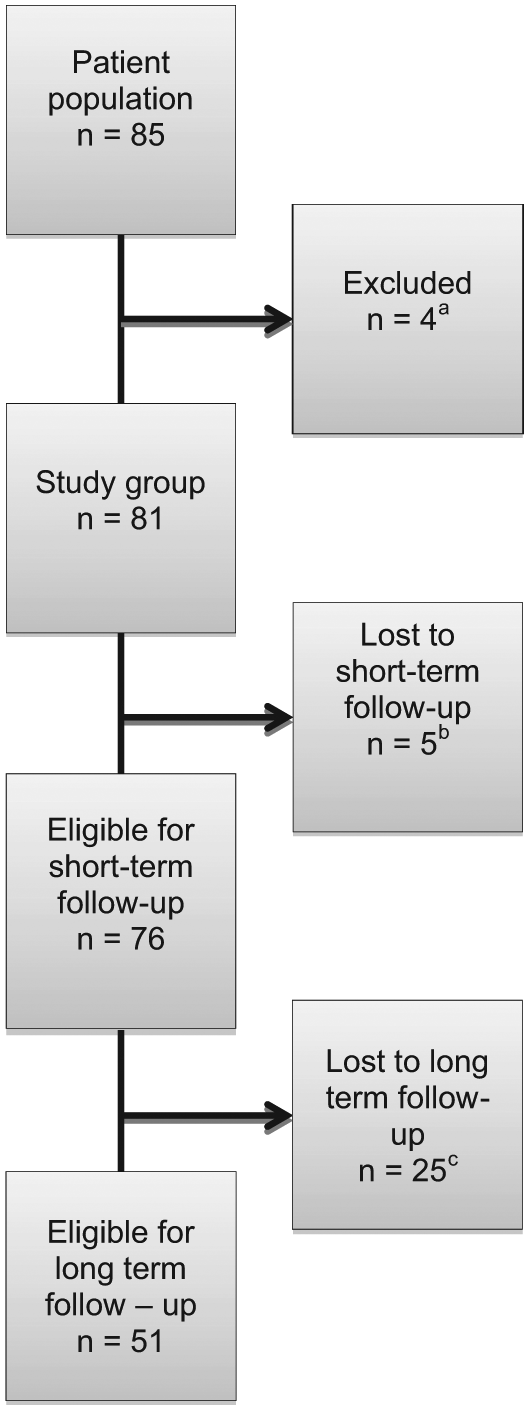
Study population.
Patient demographics and pre- and peroperative data from patients undergoing LPR are shown in Table 1. Most patients were women. Median age was 73 (57–80.5) years and median BMI was 22 (19.9–24.4). Comorbidity was present in almost two-thirds of the patients. Patients that underwent LPR had a mean ASA score of 1.8.
Demographic, pre- and peroperative clinical characteristics in 81 adult Danes who underwent laparoscopic posterior rectopexy a .
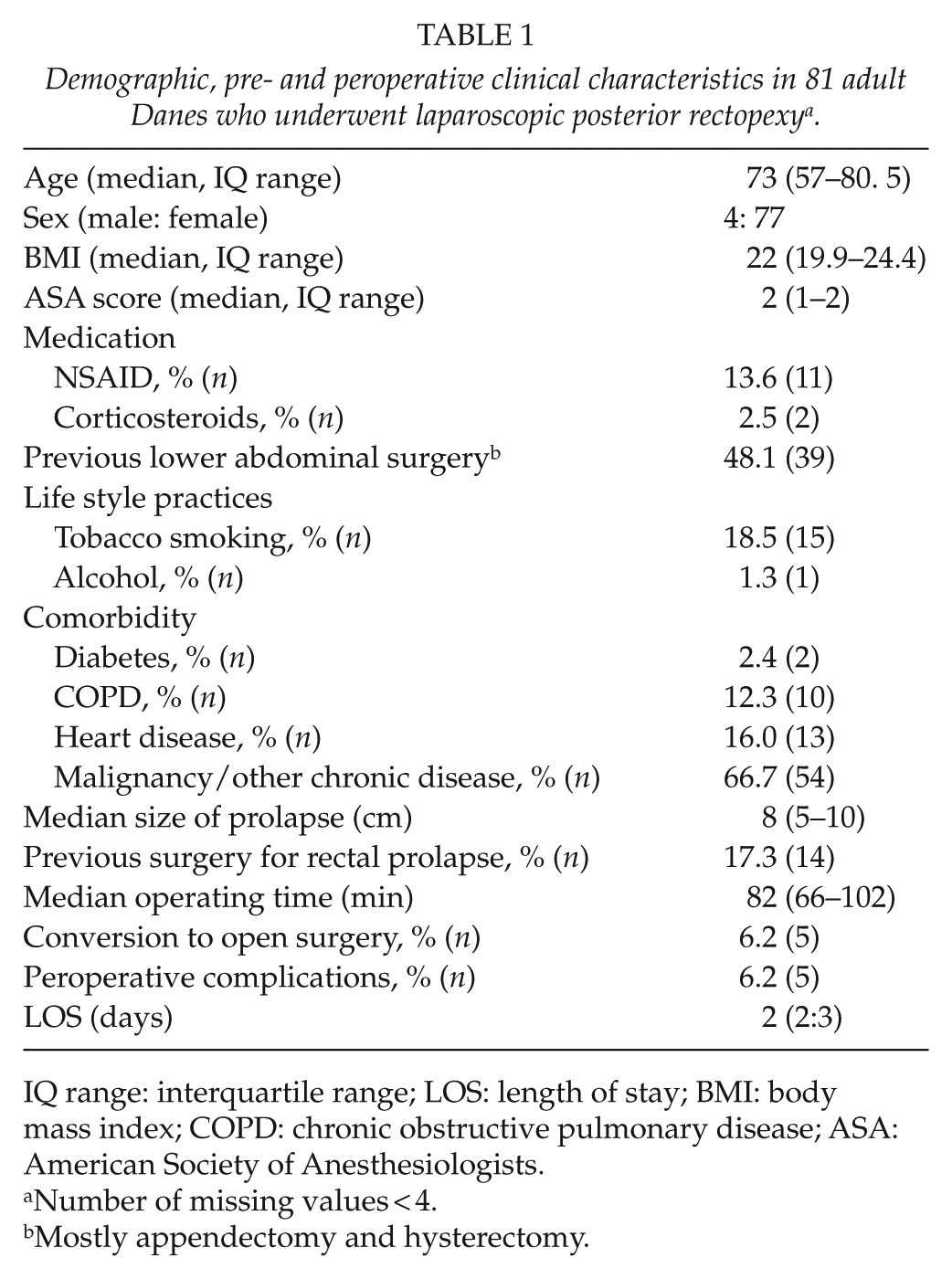
IQ range: interquartile range; LOS: length of stay; BMI: body mass index; COPD: chronic obstructive pulmonary disease; ASA: American Society of Anesthesiologists.
Number of missing values < 4.
Mostly appendectomy and hysterectomy.
Median prolapse size was 8 cm (5–10), and the maximum size was 15 cm. Almost 80% had preoperative functional symptoms, primarily incontinence (55.6%) or constipation (30.9%).
A total of 14 (17.3%) patients reported previous surgery for rectal prolapse. Six patients had had a perineal procedure (Altemeier’s or Delorme’s operation). Open and laparoscopic rectopexy had been done in three patients, two patients had had a Longo procedure, and three patients had undergone more than one previous procedure. Hysterectomy or appendectomy was reported in 48.1% of the patients.
Additionally, 23 patients with a history of former complicated abdominal surgery and/or severe comorbidity were scheduled for an Altemeier procedure in the same study period. Of those, six patients had surgery because of a failed LPR. Three more patients were scheduled for a Delorme procedure, and one patient had a Delorme procedure after a recurrence after LPR. The mean ASA score of patients scheduled for a perineal procedure was 2.7.
Peroperative Data
Median duration of surgery was 82 min (66–102). Bleeding occurred in five patients (6.2%). Conversion to open surgery was necessary in five cases (6.2%; bleeding = 1, adhesions = 1, poor overview = 2, and unknown reasons = 1). Median LOS was 2 days (2–5.7).
Postoperative Complications
In total, 19.7% (n = 16) had postoperative complications (Table 2). Major complications were seen in 12 patients (14.8%). Port site hernias causing small bowel obstruction were seen in four patients, and one more patient had a small bowel obstruction due to adhesions. Four cases of postoperative bleeding and one wound infection occurred. One patient, who had cardiac arrest, was resuscitated without injury. One patient was re-operated after 7 days due to sepsis and necrosis of the sigmoid colon. The patient was suffering from atherosclerosis. The most likely explanation was probably thrombosis of the inferior mesenteric artery due to handling of the mesorectum. A Hartmann’s procedure was performed but the patient died from septic complications. The 30-day mortality rate was 1.2% (Table 2).
Postoperative complications.
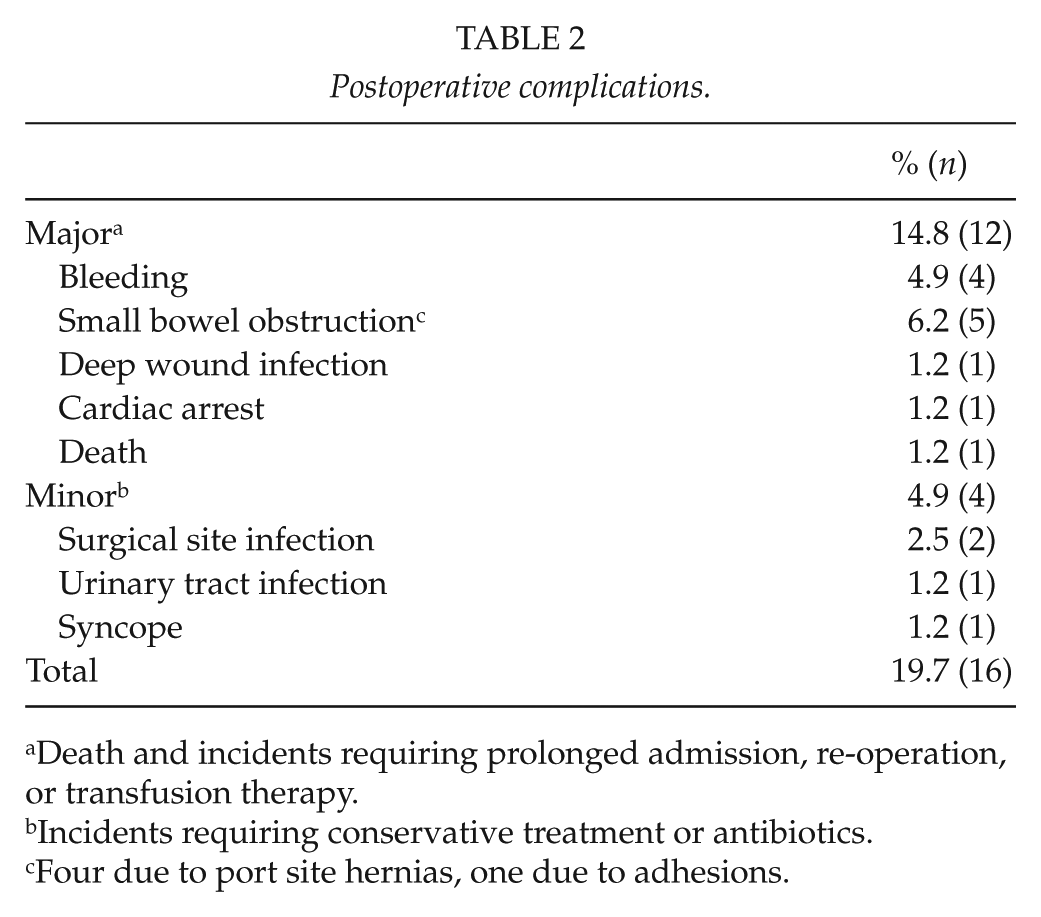
Death and incidents requiring prolonged admission, re-operation, or transfusion therapy.
Incidents requiring conservative treatment or antibiotics.
Four due to port site hernias, one due to adhesions.
Minor complications occurred in four patients (4.9%; Table 2).
Short-Term Follow-Up (60 Days)
A total of 76 patients returned for short-term follow-up. Median short-term follow-up took place 64 (57–69) days from surgery.
Short-term recurrence was 7.8% (n = 6). No recurrences were seen in patients with a previous history of rectal prolapse surgery.
Postoperative incontinence and constipation was reported in 15.7% and 24.5% of the patients, respectively. Of 43 patients who reported preoperative incontinence, 11 (26%) were still incontinent after surgery. In 23 patients with preoperative constipation, 15 patients reported that constipation had resolved. De novo constipation was described in nine patients (12.9%).
Long-Term Folllow-Up
Long-term follow-up of 51 eligible patients was done after a median of 731.5 IQR (421–1095) days (~2 years) after surgery (Fig. 1) ranging from 178 to 1095 days. Recurrences were reported in seven (13.5%) of the patients who could be reached. Four of these patients already had recurrence at short-term follow-up. Two patients had undergone re-operative prolapse surgery.
Incontinence or constipation was reported in 13.7% and 27.5%, respectively. In seven patients reporting incontinence at long-term follow-up, three patients were incontinent both prior to surgery and at short-term follow-up, while four patients had been temporary continent at short-term follow-up, however, with relapse of incontinence at long-term follow-up. Among those with constipation at long-term follow-up, 51% had no previous complaints of constipation before surgery or at short-term follow-up. Most patients were satisfied with the functional outcome (72.5%) and would recommend the procedure to other patients.
Cumulated Incidence of Rectal Prolapse Recurrence
Out of 81 patients, 9 had a recurrence diagnosed either at short-term or at long-term follow-up. The cumulated incidence of recurrence after a median observation time of 2 years was 11.1%. Cumulated incidence of recurrence were 19.2%, 12.5%, 5.6%, and 4.8% for patients operated in 2009, 2010, 2011, and 2012, respectively. No differences were seen in median age, prolapse size, or duration of procedure between patients with and without recurrence (p > 0.45). Comorbidity, ASA score, medication use, and alcohol abuse did not affect recurrence rates. Current smokers had significantly higher recurrence rates than non-smokers (26.7% vs 8.1%, chi-square test, p = 0.04). Patients with recurrence were offered a perineal re-operation.
Discussion
In this observational follow-up study of 81 consecutive patients with FRP, the 60-day recurrence rate was 7.8%, and cumulated incidence of recurrence was 11.1% after a median follow-up of 2 years. Smoking was associated with an increased risk of recurrence. Median operating time was 82 min and median LOS was 2 days. Major postoperative complications occurred in 14.8%, including port site hernias requiring re-operative surgery in 4.9%. The 30-day overall mortality was 1.2%. Bowel function, that is, incontinence and constipation, improved markedly, but 13% reported supervening constipation after surgery.
Many surgical techniques have been described for the treatment of rectal prolapse, and recurrence rates, complication rates, and changes in bowel function after surgery have varied accordingly (3–5, 8, 9). Even though anterior rectopexy has gained wide interest because of assumed lower risk of nerve damage and postoperative constipation (10), a recent Cochrane review was inconclusive in terms of selecting the most optimal choice of laparoscopic procedure (5). The posterior laparoscopic approach was chosen in this study because of considerable local experience in the open Welsh procedure. LPR seems to be well tolerated in old relatively unselected patients with varying degrees of comorbidity. Approximately 70% of the patients were categorized as ASA Groups 2–3, almost half of the patients reported previous lower abdominal surgery, and 17.3% underwent LPR after a failed previous procedure. Despite this, 30-day mortality was low (1.2%) and the recurrence rate after a median observation time of 2 years was acceptable (11.1%). These findings are in line with a study by Lindsey who reported very convincing data on this procedure, and suggested that perineal procedures should be reserved for the very frail patient (11).
A high number of hernias located at the right iliac fossa 12 mm port site were seen. Port site hernias after laparoscopic procedures are rare (12). Patients with FRP are more likely to suffer from hypermobility syndrome, Ehlers Danloss, and collagen or elastin tissue defects (13–15). This may suggest that a defect in the connective tissues could weaken both the abdominal wall and the suspension of the rectum to the pelvic walls thereby increasing the risk of port site hernias and FRP.
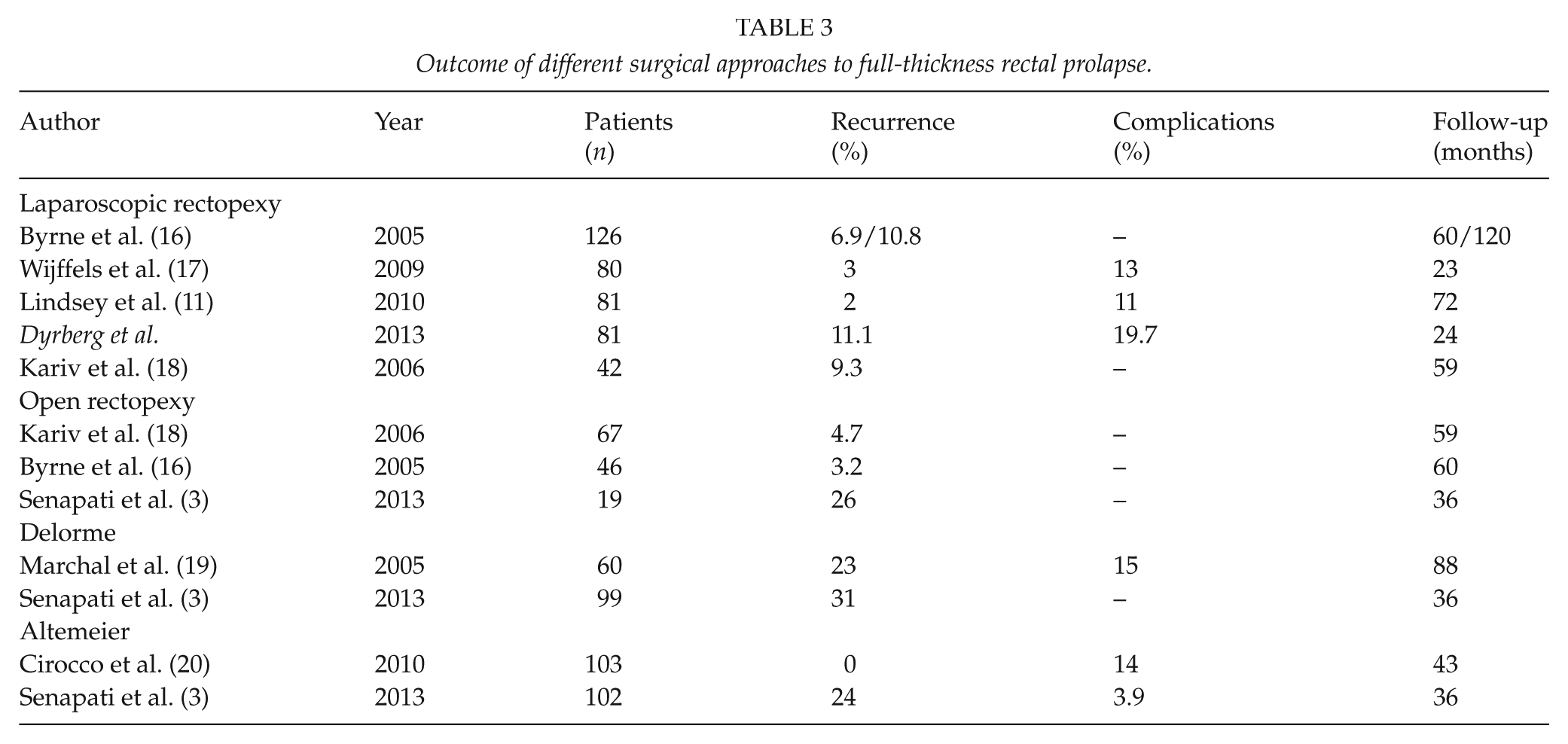
Recurrence after surgery for FRP has been reported as high as 11% after LPR, 26% after open abdominal rectopexy, and 24%–31% after a perineal procedure (Table 3) (3–5, 9, 16, 17, 19, 20). These findings are in accordance with the results of this study.
Outcome of different surgical approaches to full-thickness rectal prolapse.
It is well documented that smoking interferes with wound healing and increases the risk of postoperative complications such as anastomotic dehiscence after colorectal surgery (21). Tobacco smoking was associated with recurrence in this study. It is likely that the number of smokers was actually higher as patients tend to underestimate their use of tobacco. A liberal inclusion of frail patients with comorbidity, re-do surgery for previous FRP procedures and a relatively old study population may also have increased our recurrence rates.
LPR seemed to induce constipation in 12% of the patients. Lateral stalks were not routinely divided in this study. This may have minimized postoperative constipation (4). It has been suggested that de novo constipation is less frequent after anterior rectopexy, but there is no evidence to support this notion. Interestingly, LPR improved preoperative constipation in 65.2% (15/23) of patients in this study. This is in agreement with other studies, which have found improvement in 0%–84% of patients (4, 18).
Fecal incontinence is improved after surgery in 27%–90% of patients (4). In this study, 74.4% (32/43) stated complete elimination or improvement of incontinence 60 days after surgery; the corresponding proportion was 86.3% (44/51) 2 years after LPR. The mechanism of this restitution includes improvement in rectal compliance and anorectal sensation, restoration of internal anal sphincter function, and postoperative constipation (1, 22).
Median operating time was 82 min, and overall conversion rate was 6.2%. A recent study found an overall conversion rate of 7.2% after excluding patients with a BMI > 40 (18). Other studies have reported operating time from 110 to 174.3 min (1). The shorter operating time in this study may be due to the fact that the rectum was only mobilized posteriorly and laterally, no bowel resection was done, and peritoneum in the small pelvis was not closed after mesh fixation. No postoperative complications were caused by mesh adhesions within the observation period. Non-absorbable mesh and mesh sutures were used in this study. It is unknown whether biological meshes may provide better outcomes than non-absorbable meshes (23).
Minor and major postoperative complications occurred in 19.7%. This is slightly higher than previously reported for both perineal and transabdominal procedures (Table 3). We applied a broad definition of complications and included all cases in which postoperative convalescence was abnormal. Previous uncomplicated abdominal surgeries did not rule out LPR. Indication for LPR was liberal and all patients referred with FRP were primarily considered for an abdominal procedure. One patient died (1.2%). Other studies have found higher mortality, and some have found lower (3, 11). Considering the fact that many patients were old, we believe that complication and mortality rates found in this study are acceptable.
There are some limitations to this study. This is an observational study based on chart review with a subsequent prospective follow-up of 62.9% of the patients, which may increase the risk of selection bias. The fact that a validated registration of the functional outcome and quality of life before and after surgery was not used represents another limitation. One of the strengths of this study were that all patients were treated free of charge at a public hospital in Denmark. This minimizes the risk of selection bias. Two colorectal surgeons with considerable experience in laparoscopic colorectal surgery made the diagnosis and procedures. This strategy ensures accurate diagnosis, but makes it difficult to generalize findings to units with less experience in laparoscopic surgery. All patients could be tracked by their unique traceable 10-digit social security number provided by the Danish Civil Registry System (24) after surgery, which enabled thorough follow-up of responding patients alive.
Finally, this study has relatively long median observation period compared to similar previous studies. This is a major strength, as the risk of recurrence increases with time (16, 25).
In conclusion, LPR is an effective treatment for FRP. Length of stay is short even in old and frail patients with significant comorbidity. The procedure is safe, feasible, and fast and can be done with acceptable recurrence rates and significant improvement in functional outcomes. Randomized trials comparing anterior and posterior laparoscopic mesh rectopexy are needed.
Footnotes
Declaration of Conflicting Interests
The authors have no conflict of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or non-for-profit sectors.