
Abstract
Introduction:
Controversy exists between laparoscopic Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding in super-obese patients.
Methods:
This is a retrospective review of prospectively collected data. A total of 102 consecutive super-obese (body mass index >50) patients underwent laparoscopic Roux-en-Y gastric bypass (Group 1), and 79 consecutive ones underwent laparoscopic adjustable gastric banding (Group 2). Early complications and weight loss outcomes were evaluated.
Results:
No significant difference was found in operative mean (±standard deviation) time (93.5 ± 33 vs 87.7 ± 39 min, p = 0.29), hospital stay (2.68 ± 2.27 vs 2.75 ± 1.84 days, p = 0.80), or overall early postoperative morbidity (17.65% and 10.12%, p = 0.20). Intra-operative complications occurred in six patients (5.9%) in Group 1 and none in Group 2 (0.0%, p = 0.04). Mean excess weight loss percent at 6 and 12 months in Group 1 was 44.75% ± 11.84% and 54.71% ± 18.18% versus 26.20% ± 12.42% and 31.55% ± 19.79% in Group 2 (p < 0.001).
Conclusion:
There seems to be no significant differences in early complications between laparoscopic Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding operations in the short term. Weight loss and excess weight loss percent at 6 and 12 months are significantly better after laparoscopic Roux-en-Y gastric bypass.
Keywords
Introduction
Bariatric surgery has proven effective in reducing weight, decreasing comorbidities and mortality, and improving quality of life of morbidly obese patients (1–3). Morbid obesity is defined as a body mass index (BMI) >40 or >35 kg/m2 with comorbidities, while patients with BMI >50 kg/m2 are classified as super-obese (4).
Many operations have been proposed, but only a few are currently in use. Despite the marked increase in prevalence of sleeve gastrectomy worldwide (27.8%) in 2011, laparoscopic Roux-en-Y gastric bypass (LRYGB; 46.6%) and laparoscopic adjustable gastric banding (LAGB; 17.8%) are still very common procedures (5, 6). While LRYGB seems to be advantageous in terms of weight loss (WL), LAGB could be more suited for high-risk patients because of its lesser invasiveness and complication rate in the short term (6). Controversy still exists regarding the indications and outcomes of these two operations. For super-obese patients, the picture is even less clear, and successful treatment of super-obese patients has been reported following both LRYGB and LAGB.
There is progressive health impairment with increasing BMI (7). Therefore, super-obese patients have a higher incidence of medical comorbidity such as hypertension, diabetes mellitus, pulmonary dysfunction, sleep apnea, and degenerative arthritis, predisposing these patients to a greater risk following bariatric surgery (8).
Further complicating this issue is the lack of evidence-based outcome data comparing LRYGB and LAGB in this high-risk patient population. The literature regarding both LAGB and LRYGB in super-morbidly obese patients is sparse. Many studies combine data of all patients who meet criteria for bariatric surgery, despite differences in comorbidity, technical considerations, and outcome associated with more advanced stages of obesity. The aim of this study is to compare the early outcomes and peri-operative complications of LRYGB and LAGB operations in super-obese patients.
Methods
This is a retrospective review of prospectively collected data. Between 2006 and 2009, 733 consecutive patients underwent laparoscopic bariatric surgery at our institution (a district hospital), operated by the same surgical team (297 LAGB and 436 LRYGB). Of these patients, 181 (24.69%) had a BMI >50 kg/m2 and were classified as super-obese.
Inclusion criteria for this study were as follows: BMI >50 kg/m2, a minimum follow-up of 12 months, and no previous bariatric procedures (revisional surgery excluded). Patients were divided into two groups on the basis of the procedure. Patient characteristics are outlined in Table 1. Correspondingly, 91.1% and 74.7% suffered from at least one of the most typical co-morbid conditions associated with heavy overweight.
Demographics of patients at time of study.
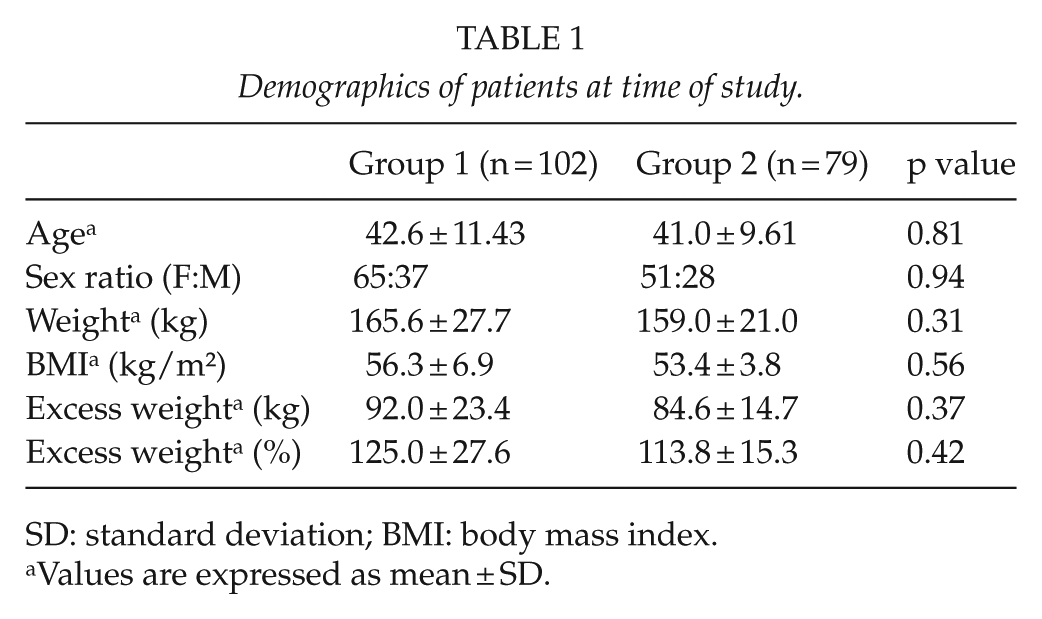
SD: standard deviation; BMI: body mass index.
Values are expressed as mean ± SD.
Operative time, intra-operative complications, hospital stay, and major and minor complications were compared. Complications were defined and graded according to Clavien–Dindo classification (9).
Patients were followed every 3 months for the first year, through our institutional bariatric surgery outpatient clinic. Data were entered prospectively into the hospital’s database for bariatric patients and retrospectively reviewed. WL, BMI, and excess weight loss percent (EWL%) outcomes were evaluated at 6 and 12 months postoperatively. The study protocol was approved by the Institutional Review Board.
Operative Technique and Peri-Operative Management
The surgical technique used for LAGB has been previously described (10). Basically, we used the “pars flaccida” technique and a broad, low-pressure band, the Swedish adjustable gastric band (Obtech, Baar, Switzerland, later and now associated with Ethicon Endo-Surgery, Cincinnati, Ohio, United States). LRYGB was performed using a 5-trocar, double-loop technique and treated by fast-track pathways as recently described in detail (11). Fast-track compliance was 100%. In total, 11 super-obese patients were operated by the means of circular stapler in the creation of the gastrojejunal anastomosis as also described earlier because it was our standard technique during the first 30 LRYGB cases (12).
Statistical Analysis
The results of parametric and nonparametric data were expressed as mean ± standard deviation (SD), and SPSS statistical software (SPSS 16.0.1, Chicago, IL, USA) was used for all statistical analyses. Confidence intervals were set at 95%. A two-sided p value of ≤0.05 was considered as statistically significant. Comparisons between both groups were determined using Fisher’s exact test for discrete variables because of the nonparametric nature of the data and Student’s t-test for continuous variables. A post hoc statistical power of 0.184 was calculated for the two-tailed hypothesis for the continuous outcome measures, while a post hoc statistical power of 0.292 for discrete variables with an observed effect size (Cohen’s d) of 0.159.
Results
The two groups were comparable (Table 1). There were no significant differences in operative time (93.51 ± 33.32 vs 87.72 ± 39.24 min), conversion rates (0% in both groups), or hospital stay (2.68 ± 2.27 vs 2.75 ± 1.84). A total of six patients (5.9%) in Group 1 had intra-operative complications due to anastomotic or gastric pouch leak during intra-operative leak testing with methylene blue (three patients), bowel perforations due to stapler—iatrogenic injury—(two patients), and one case of anvil detachment from gastric tube in the upper esophagus because a circular stapling gastrojejunal anastomosis was performed that needed intra-operative gastroscopy. However, all intra-operative complications were managed without further sequel. No intra-operative complications occurred in Group 2 (0.0%), with a significant difference (p = 0.04).
There were no significant differences in overall early postoperative complication rates between the groups, although the LRYGB group had a higher early morbidity rate (17.65% vs 10.12%, p = 0.20) compared to the LAGB group. Overall number of complications was not significantly higher in Group 1 (21 vs 12, p = 0.44). Clavien–Dindo grade III complications were significantly higher in LRYGB group (p = 0.01, Table 2). Mostly, complications included wound infections, hemorrhage, anastomosis leakage, or stricture (Table 2).
Postoperative complications <30 days. a
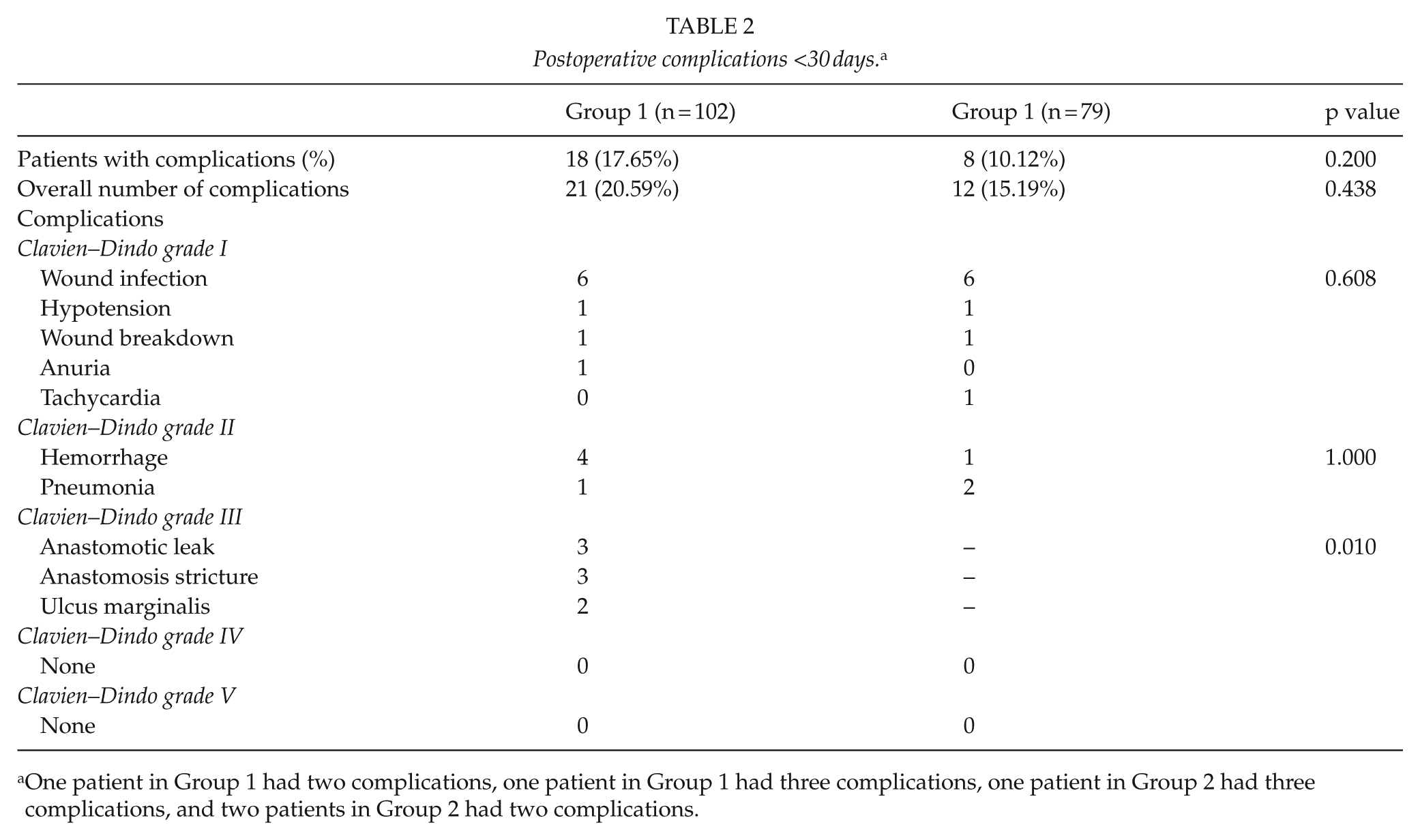
One patient in Group 1 had two complications, one patient in Group 1 had three complications, one patient in Group 2 had three complications, and two patients in Group 2 had two complications.
The mean WL, BMI, and mean EWL% at 6 and 12 months are summarized in Table 3. WL after LRYGB compared to that following LAGB was significantly greater at both 6- and 12-month follow-up. Similarly, BMI at 6 and 12 months was significantly lower after LRYGB. The EWL% mean values were significantly higher at 6 and 12 months in favor of the LRYGB group (Table 3). Follow-up adherence at 12 months was 92.5%.
Comparison of weight loss outcomes in Group 1 and Group 2 patients.
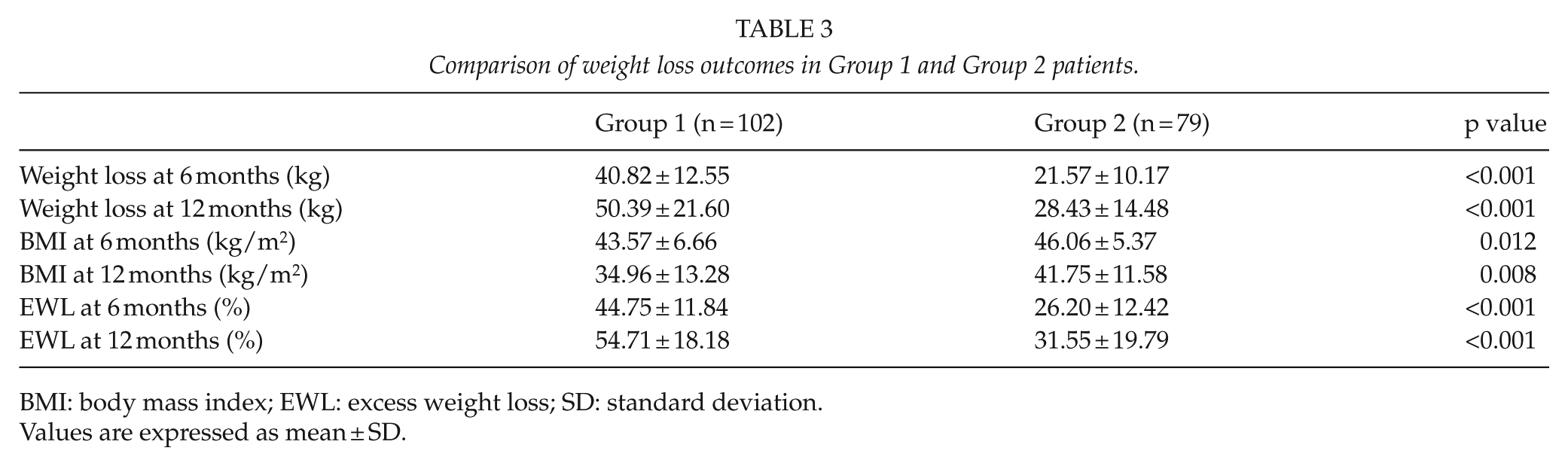
BMI: body mass index; EWL: excess weight loss; SD: standard deviation.
Values are expressed as mean ± SD.
Discussion
Our retrospective study compared early outcomes following LRYGB and LAGB operations in super-obese patients. There are several reasons to distinguish between morbid obesity (BMI >40 kg/m2) and super-obesity BMI >50 kg/m2). First, super-obese patients more frequently have associated life-threatening co-morbid conditions, and therefore, they have an elevated surgical risk (13). Second, super-obese patients often fail to achieve satisfactory WL after purely restrictive operations (14, 15). Third, the heaviest patients need to lose more weight to achieve a valid reduction in their mortality risk (16, 17). In addition, the number of patients who fall into the super-obese and super-super-obese (BMI >60 kg/m2) categories is growing (18, 19).
Thus, from a surgical point of view, super-obese patients remain a difficult population to manage, usually with outcomes slightly worse than the outcomes following surgery for morbid obesity (19). Furthermore, there is no real consensus concerning the best surgical procedure for super-obesity (16). This fragile population has benefited from different bariatric procedures: studies on sleeve gastrectomy, duodenal switch, gastric banding, and Roux-en-Y gastric bypass have all reported relatively safe outcomes (20, 21).
Although evidence suggests that LAGB is not the most effective bariatric procedure concerning WL (6), it is still popular, with a worldwide prevalence of 17.8% in 2011 (5). This may be related to the lower costs and early morbidity compared with LRYGB (22). Indeed, a very recent large study showed that the procedure with the lowest 30-day mortality rate is still LAGB (0.02%) (23).
All bariatric/metabolic operations have their advantages and disadvantages. The LAGB operation is considered the least invasive method of all laparoscopically performed operations aiming at weight reduction and resolution of comorbidities. In addition, it is a totally reversible operation and easier to reverse compared to LRYGB. It may be associated with a shorter learning curve and a lower early postoperative complication rate compared to LRYGB (6, 23). On the other hand, LRYGB has shown to be safe even in the learning curve period and more effective than LAGB in maintaining WL in the long term (24, 25).
For the purposes of this study, we focused on relatively short-term postoperative complications and results in order to compare the postoperative safety of these two procedures in super-obese patients. Our retrospective analysis showed that in the peri-operative and early postoperative phases (<30 days), the overall complication rate was nearly similar in both groups (Table 2). However, Clavien–Dindo grade III complications (9) were significantly higher in LRYGB group, showing the potential risk associated with gastrointestinal tissue manipulation (p = 0.01, Table 2). Furthermore, LRYGB group presented a significantly higher intra-operative complication rate (p = 0.04). Previous studies showed early postoperative complication rates ranging from 0.8% to 12% in LAGB series and from 5.5% to 30% in LRYGB series (6, 25). Indeed, the hospitalization time after both methods is low and still considered significantly lower in the LAGB group (25). However, in our series of super-obese patients, we did not find any differences regarding the hospital stay (p = 0.80).
It is well known that late postoperative complications and failures are more common following LAGB operations compared to LRYGB operations (26) and may be even more so in super-obese patients (27). WL and failures tend to increase in the long term, and one weakness of this study is our short follow-up time of only 12 months. However, lower long-term complication rates and better outcomes in terms of WL after LRYGB are sometimes accompanied by serious life-threatening adverse events (26). In contrast, revisional bariatric procedures have much higher complication rate than primary operations (14).
LAGB exposes patients to failure rates reported to be as high as 40%–50% and to revision rates of 20%–30% (14). On the other hand, a recent study on LAGB from Australia (28) demonstrated a durable EWL of 47% at 15 years and a very high safety of LAGB, with 1 death in a total of 6177 patients. They reported a need for additional surgery due to late adverse events, with nearly half of the patients requiring one or more revisional procedure during the follow-up period (28). In the literature, long-term studies (>10 years) showed an EWL maintenance in the range of 33%–60% (28). However, it has been indicated that the overall rate of revision might not be too different between LRYGB and LAGB, as the median rate for revisional procedures after LRYGB was 22%, with a range of 8%–38% (28). In a recent 6-year-follow-up randomized study, including 66 patients, with a BMI range from 40.5 to 43.1, Werling et al. (29) showed that gastric bypass was superior to vertical banded gastroplasty regarding WL, body composition, dietary composition, and postprandial satiety hormone responses. In contrast, more recently, a matched-pairs analysis for preoperative airways, BMI, cardiovascular, and diabetes scores showed that both procedures had similar improvements in all scores, except for BMI where LRYGB had a greater reduction than LAGB (30).
There are only two previous studies comparing LAGB and LRYGB in super-obese patients. Mognol et al. (31) studied 290 patients with BMI >50 finding significant differences in the early postoperative period and hospital stay with more sustained WL at about 2 years in the LRYGB group. Bowne et al. (32) showed that at 16-month follow-up, LAGB super-obese patients had significantly more late complications, re-operations, less WL, less reduction in comorbidities, and more dissatisfaction compared with LRYGB. We did not find significant difference in overall early morbidity between the groups, except for the slightly higher incidence of intra-operative and anastomosis-related complications in the LRYGB group (Table 2).
Beyond the short follow-up time, this study has several limitations including the retrospective and non-randomized nature as well as the different preoperative patients’ demographics, although not statistically significant. Moreover, the study is not adequately powered in order to draw definitive conclusions. It is also difficult to evaluate the possible impact of the learning curve on the results, as 11 of the super-obese patients undergoing LRYGB were operated during our learning curve period for this procedure (24). Another potential bias may come from the proportion of patient lost to follow-up, which is known to create a particular challenge in assessing bariatric surgical outcomes, as it is likely that the bariatric surgery patients who are not doing well are the most hesitant to return for follow-up (33).
In conclusion, super-obese patients have higher postoperative complications and higher failure rate after bariatric surgery compared to morbid obese patients; therefore, different assessing criteria might be used for the management of this challenging population. Our study supports the primary use of LRYGB as a safe procedure in super-obese patients. LAGB can be one of the accepted surgical tools for WL for high-risk patients willing to be involved in a regular and long-term postoperative WL management educational program. The results of this study should be interpreted with caution as it is a not randomized study, and there is likely to be some form of selection bias which might have a confounding effect.
Footnotes
Declaration of Conflicting Interests
No commercial associations or disclosures may pose or create any conflict of interest with the information presented in this article.