
Abstract
Background and Aims:
Elderly patient might experience an increased risk of complications after laparoscopic Roux-en-Y gastric bypass. We aimed to perform a meta-analysis of comparative studies on this issue in patients aged 60 years or older.
Material and Methods:
A systematic literature search was performed. Medline, Cochrane Library, Embase, Scopus, and Google Scholar were searched until July 2016 for studies on outcomes of laparoscopic Roux-en-Y gastric bypass in elderly versus younger patients. Primary outcomes were mortality and overall complications. Secondary outcomes were length of hospital stay, excess weight loss percentage, effect on diabetes, hypertension, hyperlipidemia and obstructive sleep apnea. Heterogeneity across the studies was evaluated by the I2 test, and a random effects model was used. Results were expressed as mean difference and risk ratio (RR).
Results:
Seven studies involving 3128 patients were retrieved and included in this study. A significantly increased risk of mortality and overall complications was observed among patients older than 60 years compared with younger ones (RR, 6.12; 95% confidence interval 1.08–34.83; p = 0.04; RR, 1.51; 95% confidence interval 1.07–2.11; p = 0.02). Particularly, elderly patients experienced 1% increased risk of mortality and 3% increased risk of overall complications. Length of stay, diabetes, and obstructive sleep apnea remission rates were similar among the groups. Excess weight loss percentage was significantly greater among younger patients (mean difference, −3.44; 95% confidence interval −5.20, −1.68; p < 0.001), as were hypertension (RR, 0.57; 95% confidence interval 0.42–0.76; p < 0.001) and hyperlipidemia (RR, 0.61; 95% confidence interval 0.45–0.83; p = 0.002) remission rates.
Conclusion:
Laparoscopic Roux-en-Y gastric bypass in patients older than 60 years may be a risky bariatric surgery operation due to higher complications and mortality and may not be as effective as in patients younger than 60 years. Thus, older patients should be carefully counseled before this procedure for individual risk–benefit assessment.
Introduction
Life expectancy has been continuously increasing regardless of gender and ethnic background in the United States (1). Similarly, in Finland, life expectancy of a 60-year-old woman in 2008 was 24.3 years, whereas for a man of the same age, it was 22.8 years (2).
Obesity remarkably decreases life expectancy and quality of life (3), while bariatric/metabolic surgery is the most effective treatment for morbid obesity (4). Surgery has demonstrated a superior efficacy in the induction and maintenance of weight loss compared with current medical therapies (4). Furthermore, compared to conservative treatments, bariatric surgery has showed not only a greater weight loss but also more effective improvements in comorbidities typically associated with obesity, independent of the type of procedure performed (4).
Several studies have already compared weight loss achievements after different types of bariatric/metabolic surgeries (5), or different techniques of the same procedure (6), whereas others have analyzed different preoperative predictors, with controversial results (7–11).
To date, the effect of age on weight loss outcomes has been analyzed in only a few studies, most of them with insufficient numbers undergoing the same bariatric operation and results at long-term follow-up are often missing. According to some studies, elderly patients may lose less weight, gain less benefits, and they may be at a greater risk for mortality after bariatric/metabolic surgery compared to younger patients (12, 13). However, a previous meta-analysis showed comparable results for patients older than 55 years (14). In recent systematic reviews, pooled analyses resulted in low mortality and complication rates, with successful weight loss outcomes in patients older than 60 and 65 years (15, 16). However, controversy still exists regarding the indications and outcomes of laparoscopic Roux-en-Y gastric bypass (LRYGB) for the elderly obese, because of lack of comparative analyses with other procedures and with different ages (17).
We aimed to perform a systematic review and meta-analysis to summarize the current evidence regarding patients over 60 years old having LRYGB, hypothesizing that outcomes and complication rates might be comparable to those of a younger population.
Methods
Appropriate methodology according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed (18). This meta-analysis is registered in PROSPERO, an international prospective register of systematic reviews, with the reference code CRD42016041815.
We performed a literature search through Pubmed, Embase, Scopus, Cochrane Library, Google Scholar, and Research Gate aiming for any study containing data on LRYGB in patients over 60 years old (19). The search terms applied through Boolean searches in the above-mentioned databases were morbid obesity, bariatric surgery, metabolic surgery, gastric bypass, Roux-en-Y gastric bypass (RYGB), elderly, over 60 years, advanced age, and old.
Studies to be included in this review had to match predetermined criteria according to the PICOS (patients, intervention, comparator, outcomes, and study design) approach. Criteria for inclusion and exclusion are specified in Table 1.
PICOS criteria for inclusion and exclusion of studies.
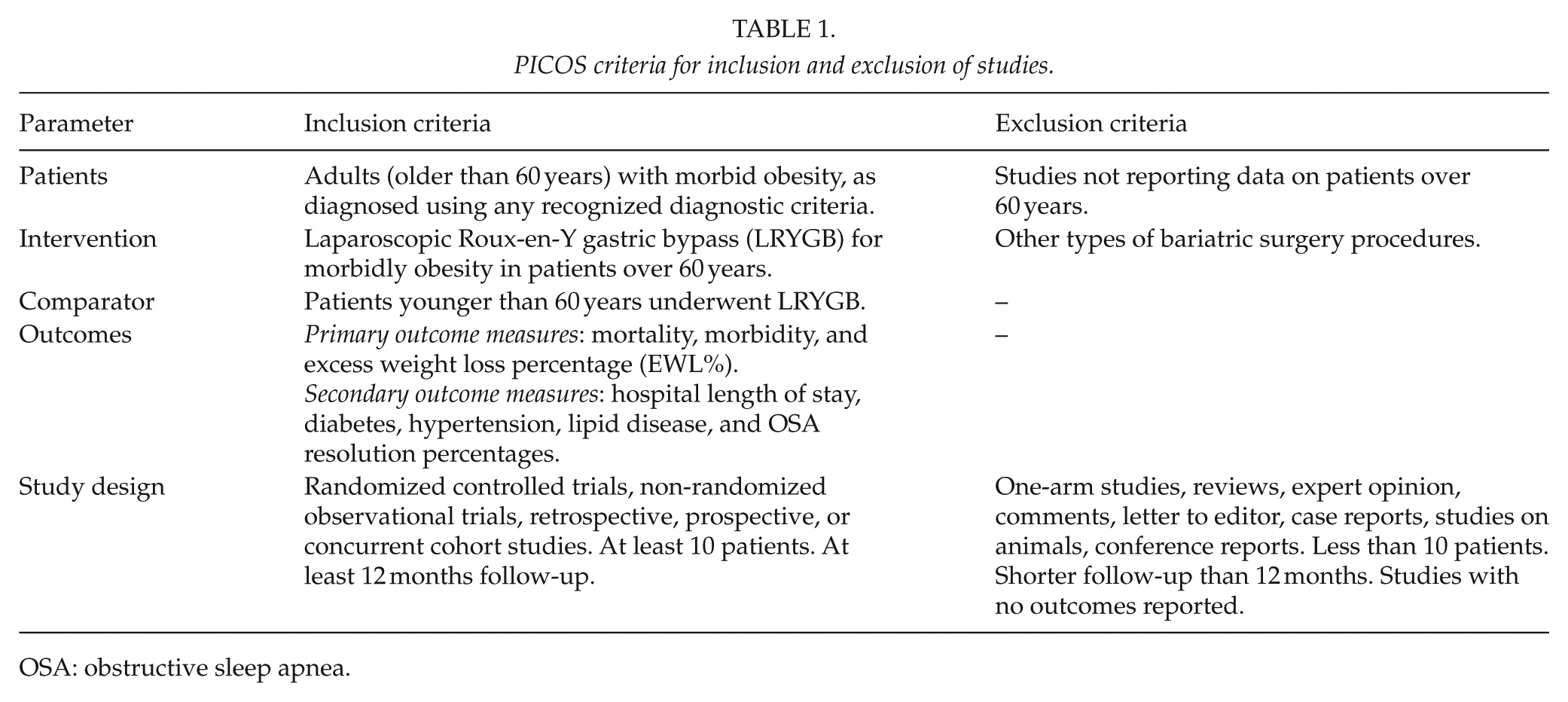
OSA: obstructive sleep apnea.
The search was performed in July 2016, in order to find those studies showing outcomes on LRYGB, also combined with RYGB, for patients aged 60 years or older in comparative fashion, with a minimum follow-up of 12 months. Furthermore, the reference lists of all relevant articles were scrutinized, attempting to identify further relevant studies. There was no restriction on language, or study design, but only comparative studies were considered. Thus, studies on other methods than LRYGB, studies including different bariatric procedures, and studies not comparative, or with a follow-up shorter than 12 months were excluded.
We chose a cut-off of 60 years of age as this age represents the United Nations standard numerical criterion for older population (19), although previous studies in bariatric surgery literature have often used the age of 55 to define older age (13, 14, 16, 20), and the definition for an elderly individual according to the World Health Organization is 65 years (19). References potentially dealing with this topic were individually searched and identified by two authors. The same authors independently extracted and entered the data into predesigned tables. No attempt was made to obtain missing data from the authors. However, the few missing data were dealt according to previously validated estimation formulas (21).
Outcomes studied in the meta-analysis were mortality and morbidity at 30 days from the procedure/intervention. Excess weight loss percentage (EWL%) outcomes at 1-year follow-up. Secondary outcome measures included hospital length of stay, hypertension, lipid disease, diabetes, and obstructive sleep apnea (OSA) resolution percentages compared with younger groups at follow-up.
The quality of the included studies was independently assessed by the two investigators (S.G. and M.V.) using the Newcastle–Ottawa Scale to evaluate the individual non-randomized studies (22).
We used Review Manager 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2015) to perform statistical analysis. Differences in dichotomous outcome variables were expressed as risk ratio (RR) with 95% confidence interval (CI), while differences in continuous variables were expressed as mean difference (MD) with 95% CI.
Heterogeneity was assessed with I2 statistic, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance (23). Because heterogeneity is anticipated among observational studies, we made our evaluation using a random effect model (DerSimonian–Laird) (24). To perform the meta-analysis, the Mantel–Haenszel statistical method was used for dichotomous outcome variables and inverse variance for continuous outcome variables. A p < 0.05 was considered statistically significant.
Results
The literature search yielded 1729 articles, 7 of which (17, 25–30) were pertinent to our study, and sources of reported outcomes of bariatric surgery in patients 60 years or older in a comparative study with a younger group (Table 2). The literature search flowchart is shown in Fig. 1. The analysis encompassed a total of 3128 patients. In total, 10 patients died during the 30-day postoperative period (6 in elderly group vs 4 in the younger), and a significantly increased risk of mortality among elderly patients was observed in six studies (RR 6.12; 95% CI 1.08–34.83; p = 0.04, Fig. 2), with an overall mortality risk difference of 1.00%. Similarly, overall complication rate was significantly higher in patients older than 60 years (RR 1.51; 95% CI 1.07–2.11; p = 0.02, Fig. 3), with an overall complication risk difference of 3.00%.
Characteristics of the elderly group into the included studies.
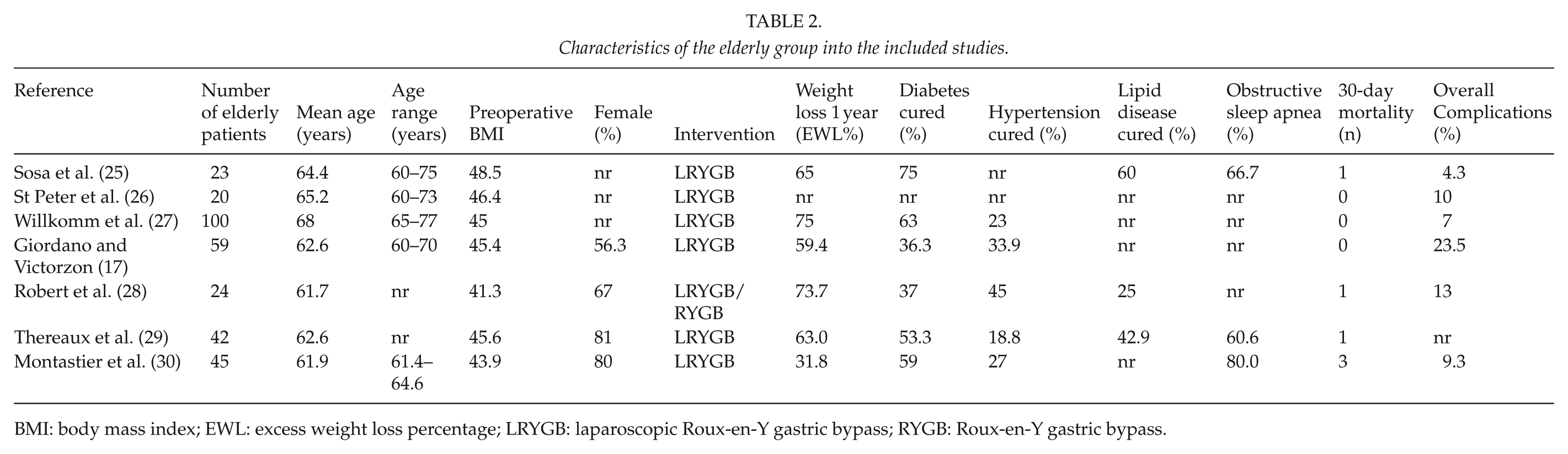
BMI: body mass index; EWL: excess weight loss percentage; LRYGB: laparoscopic Roux-en-Y gastric bypass; RYGB: Roux-en-Y gastric bypass.
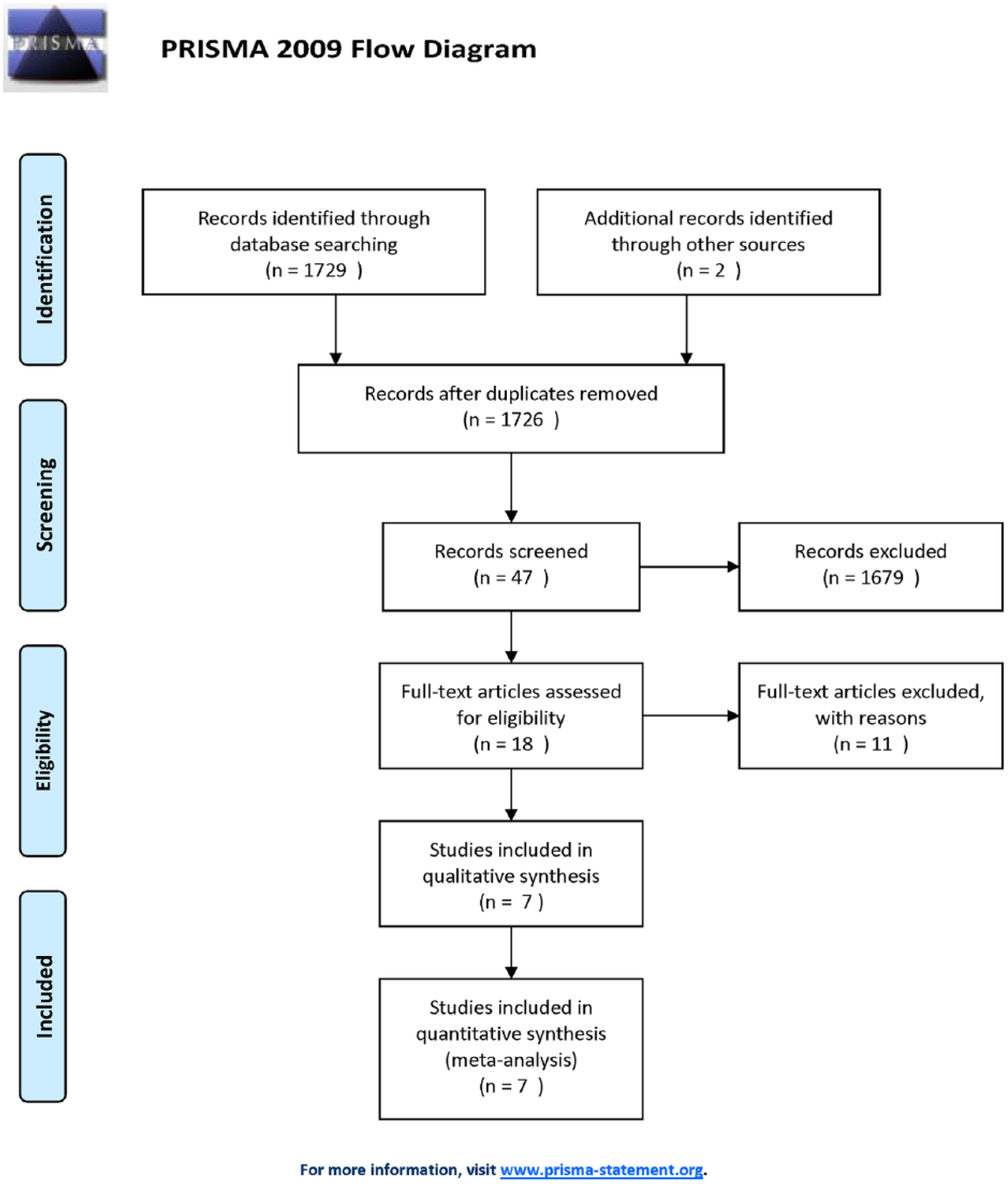
Flowchart summarizing literature search results.
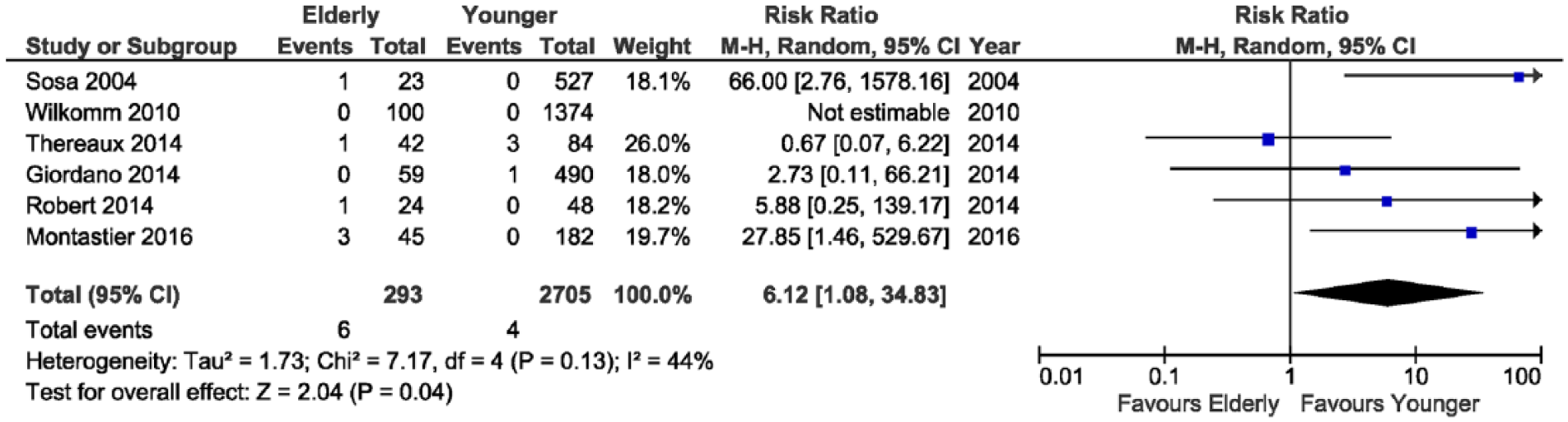
Forest plot showing a significantly lower mortality in patients younger than 60 years.
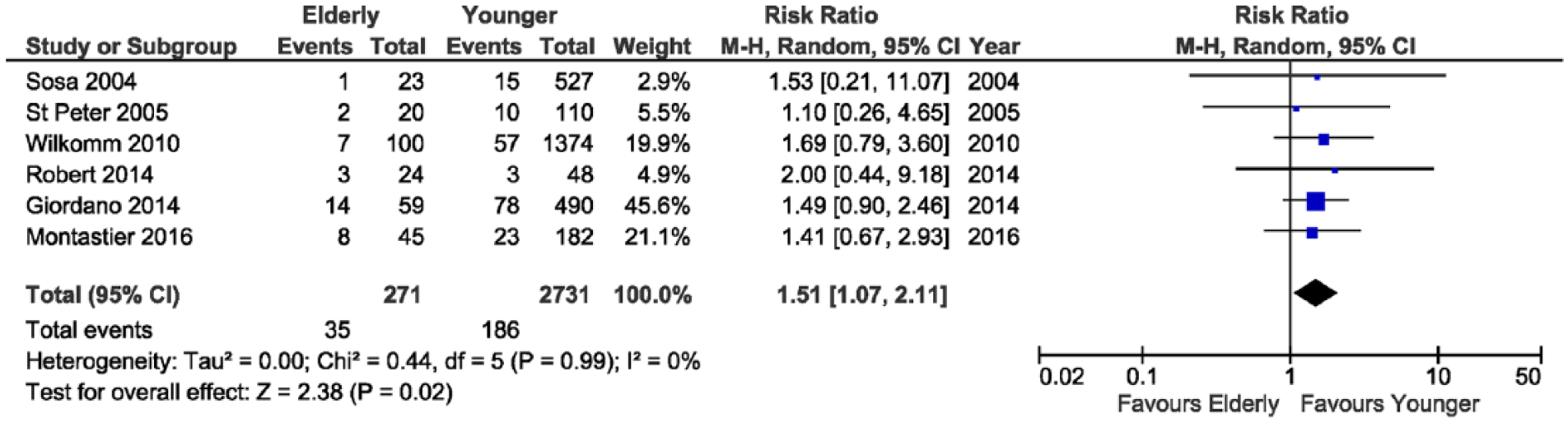
Forest plot showing a significantly lower complication rate in patients younger than 60 years.
EWL% was significantly higher among younger patients (MD −3.44; 95% CI −5.20, −1.68; p < 0.001, Fig. 4), but there was no significant difference in hospital length of stay (MD 0.29; 95% CI 0.10–0.67; p = 0.15).
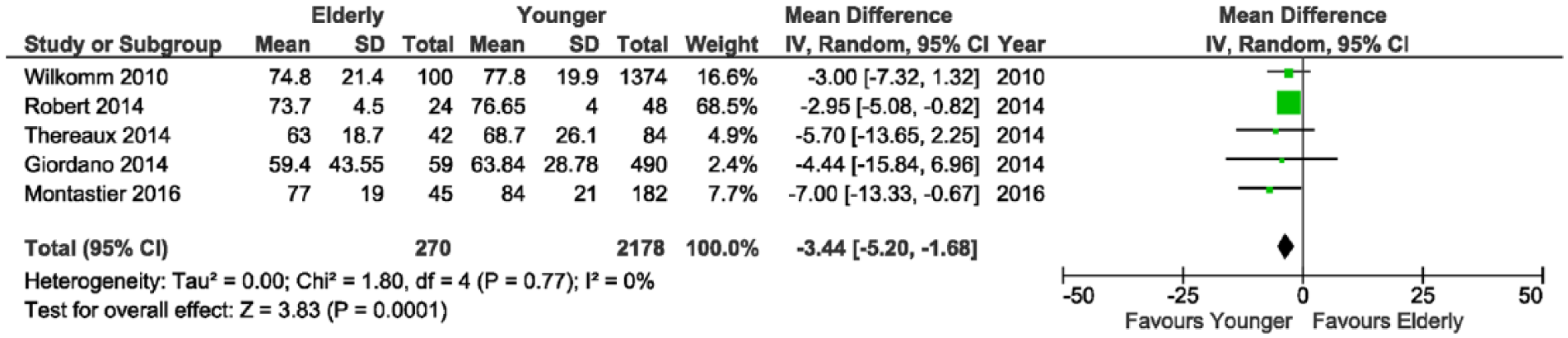
Forest plot showing significant difference in excess weight loss percentage at 1-year follow-up favoring patients younger than 60 years.
Hypertension and hyperlipidemia remissions occurred significantly more often in younger patients (RR 0.57; 95% CI 0.42–0.76; p < 0.001; RR 0.61; 95% CI 0.45–0.83; p = 0.002, respectively, Figs 5 and 6).
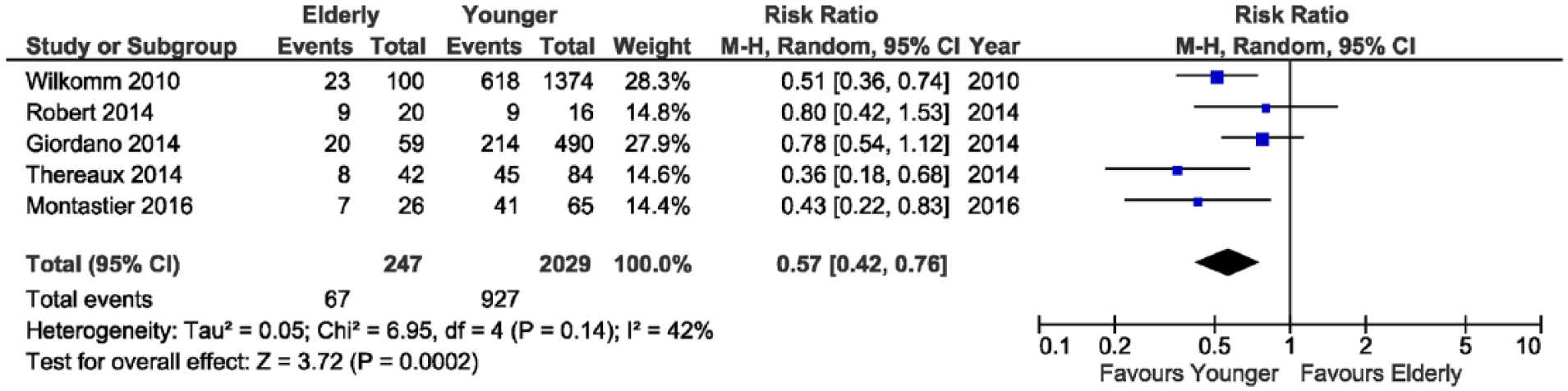
Forest plot showing significant difference in hypertension remission rates at 1-year follow-up or later.

Forest plot showing significant difference in lipid disease remission rates at 1-year follow-up or later.
No significant differences were detected among diabetes remission rates (RR 0.90; 95% CI 0.79–1.03; p = 0.13) and OSA remissions (RR 0.80; 95% CI 0.57–1.13; p < 0.20). Finally, the exclusion of most studies from the analysis did not materially change the summary estimates, with sensitivity analysis using the “leave one out” methodology, and absence of significant asymmetry in the funnel plot was observed.
Discussion
This meta-analysis of comparative studies provides an insight into the value of LRYGB in patients 60 years or older in comparison to younger. The pooled results demonstrated an overall low mortality, but more significant in the elderly group (Fig. 2). Also, overall complications occurred more often for patients older than 60 years (Fig. 3). Weight loss outcomes and chronic disease remissions favored younger patients (Figs 4 to 6).
This pooled analysis is the first one pointing out the higher overall risk and less satisfactory results of LRYGB in patients older than 60 years in a comparative fashion. Particularly, elderly patients experienced 1% increased risk of mortality and 3% increased risk of overall complications compared with younger patients after LRYGB.
The prevalence of obesity among populations 60 years or older is likely to increase together with life expectancy, regardless of gender and ethnic background (31). Consequently, the number of elderly patients requesting bariatric surgery is likely to increase (2, 3).
Some previous large cohort studies have associated body mass index (BMI) and age with important risk factors for 30-day mortality after LRYGB (31–33), showing also a linearity between increasing BMI and age with the risk of mortality (32). However, as expected, bariatric surgery is performed more often, particularly in the last decade (34) with improvement in outcomes, as well as in perioperative morbidity and mortality (34).
Dorman et al. (35) in a multi-center study found that advanced age prolongs the length of hospital stay, without major complications, although a trend toward higher mortality was observed. Similarly, Spaniolas et al. (36) comparing LRYGB and sleeve gastrectomy (SG) for elderly patients failed to demonstrate significantly different 30-day outcomes between these two procedures, showing acceptably low morbidity and mortality rates. More recently, Moon et al. (37) in a similar study found that SG had the lowest readmission and reoperation rate and that LRYGB had the highest mortality rate. In our comparative pooled analysis on only LRYGB, we did not find differences in hospital stay between the two groups (Fig. 4), but higher mortality, complications, and worse outcomes for patients older than 60 years.
It is well known that elderly patients lose less weight because of diminished metabolic activity, sarcopenia, and less mobility than younger patients. Furthermore, elderly people are fragile, they often suffer from chronic comorbidities, all determinants, which might influence baseline physical conditions of the included studies and justify these pooled outcomes.
The requirements for body energy dispense usually decrease with age (38) due to a reduced lipolytic capacity (39), particularly in sympathetic response (40), issues that can explicate the enhanced amount of fat tissue deposits in elderly people. In addition, this reduced lipolytic capacity is particularly present in postmenopausal obese women undergoing a caloric restriction diet (41).
Conversely, it has been showed that women of age 55–65 years versus 20–45 years loose less weight after bariatric surgery, not only because of a decreased capacity to use energy through the mobilization of fat from lipid deposits but also because postmenopause might induce a larger caloric intake (42). This fact is consistent with the population in the studies included in this meta-analysis represented mostly by female gender (Table 2). Nevertheless, younger patients have a reduced caloric intake especially after LRYGB (43).
Another concern is given by the fact that baseline body expenditure decrease after the age of 40, with a concomitant decline of physical activity (44, 45). A very sedentary lifestyle is common particularly during advanced age (46), while an active lifestyle is important in the maintenance of lower weight in the long-term after bariatric surgery (47).
Aging has an impact on the capacity of wound healing (48). As a consequence, the skin becomes athrophic, vulnerable to the environment, with homeostatic incapability due to a progressive loss of function (49). Microscopically, growth factors decrease, and cell proliferation and migration are reduced, with less extracellular matrix during the wound healing process (49). All these mentioned issues together can explain the higher prevalence of comorbidity and postoperative complications in elderly patients.
In a previous study and pooled analysis (15, 17), we were able to demonstrate in a non-comparative analysis that a good weight loss can be achieved by bariatric surgery in the elderly with acceptable risks, independent of the type of bariatric procedure, and LRYGB in patients >55 years did not show significantly worse morbidity than in younger patients. For this reason, we performed a pooled analysis on this topic, in order to verify these findings for LRYGB in patients older than 60 years, including only comparative studies. We demonstrated a successful excess weight loss, improvement of the most common obesity-related comorbidities, and acceptable mortality and complication rates, despite the fact that many of these outcomes were worse than in younger patients, consistent with other previous studies on this topic (12–14). Particularly, Lynch and Belgaumkar (14) also compared older (>55 years) with younger subjects, specifically the gastric bypass procedure in a separate analysis, but there were few included studies with small cohorts.
We believe that elderly patients can benefit from LRYGB, taking into account higher perioperative risks typical of elderly population. This fact has also been discussed in the recent statement of the Italian Society for Bariatric and Metabolic Surgery extending the indications toward 70 years of age (50).
Age alone should not be an absolute contraindication for bariatric surgery. Indications for bariatric surgery should be carefully evaluated in the light of routine preoperative tests and discussed with the patient acknowledging that there might be perioperative higher risks, worse outcomes than they might expect, and tailoring the best type of bariatric procedure.
This study has several limitations and potential bias influencing these findings. Our analysis focused on the LRYGB, because it is considered the most common and effective bariatric surgery procedure, also in long-term follow-up, providing very durable outcomes (51). Seven studies were used for this pooled analysis, all retrospective with clear heterogeneity in methods and settings, although the same procedure was used (Table 2). The number of patients considered was relatively small and there were differences in patients’ age in the elderly group, as well as in gender prevalence, which might be a confounding factor for the results. However, the exclusion of any study from the analysis using the “leave one out” methodology made some outcomes not significant. Thus, some publication bias might possibly have influenced these results. Furthermore, the duration of any comorbidity was not elucidated among the pooled studies, and this may be a negative factor for the chance of resolution. Unfortunately, the literature on this topic is still scarce, particularly on comparative studies. The types of complications were mostly not classified. Only one study adopted the Clavien–Dindo Classification (17). Therefore, we pooled together all major and minor complications. In addition, follow-up time and adherence percentage were different or not elucidated among the included studies, and the comorbidity resolution rates were measured at the last follow-up control.
Further original studies on this topic are warranted, particularly comparing different bariatric procedures in elderly patients, in order to optimize the guidelines, as SG might appear a safer procedure (37). In addition, there is a need for quality-of-life measurements as well as for studies on the prognosis of type 2 diabetes mellitus and its complications after bariatric procedures in elderly.
Conclusion
This meta-analysis of comparative studies demonstrated that LRYGB in elderly patients results in increased postoperative morbidity and lower effectiveness regarding resolution of comorbidities compared to the corresponding outcomes in younger patients. A bariatric surgery procedure should not be refused only because of advanced age, but elderly patients should be carefully counseled for individual patient risks, about the enhanced risks of complications, and the possibility of inadequate outcomes following LRYGB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.