
Abstract
Background and Aims:
The indications for operative treatment of lateral tibial plateau fractures are still controversial. The objective of this study was to determine whether residual articular surface depression and valgus malalignment of plated lateral tibial plateau fractures at medium-term follow-up affect the clinical and radiographic outcomes.
Material and Methods:
A chart review of patients with operatively treated (AO type B3.1) tibial plateau fractures that were admitted to our level I trauma center between 2002 and 2008 was performed. Out of 123 patients, 73 were available to participate in a clinical and radiographic follow-up examination. The mean follow-up time was 54 months. Patients were clinically assessed and completed the Lysholm knee score and Western Ontario and McMaster Universities Osteoarthritis Index. Maximal articular surface depression, radiological mechanical axis, and degree of posttraumatic osteoarthritis were evaluated from standing radiographs.
Results:
Patients with valgus malalignment of 5° or greater at follow-up developed more advanced osteoarthritis (Kellgren–Lawrence grade 3–4) than patients with a normal mechanical axis (p = 0.006). Similarly, patients with articular depression greater than 2 mm at follow-up also developed more advanced osteoarthritis compared to patients with a depression of 2 mm or less (p = 0.001). The degree of valgus malalignment or articular depression had no effect on the Western Ontario and McMaster Universities Osteoarthritis Index or Lysholm scores.
Conclusions:
The postoperative articular congruity and normal mechanical axis of the lower leg after plate fixation in lateral tibial plateau fractures seem to have a role in prevention of posttraumatic osteoarthritis but does not appear to predict clinical outcome at medium-term follow-up. The role of initial dislocation and associated cartilage damage in the development of osteoarthritis following these fractures is still unknown.
Introduction
Fractures of the lateral tibial plateau (AO type B3.1) are usually a consequence of combined valgus and axial forces to the knee. In magnetic resonance imaging (MRI) studies, lateral tibial plateau fractures are often associated with meniscal and ligamentous injuries of the knee (1). Tibial plateau fractures compose approximately 1% of all fractures with lateral plateau fractures being the most common type (2, 3). Posttraumatic osteoarthritis develops in 9%–44% of patients following a tibial plateau fracture (4–7). This may be caused by initial trauma to the tibial plateau cartilage (8–10). Furthermore, an altered axial loading pattern to the tibial plateau caused by articular incongruence can influence the development of osteoarthritis (3–6).
The optimal treatment of lateral tibial plateau fractures remains controversial. Most authors have advocated operative fixation if an articular surface depression of more than 2–3 mm or a valgus deformity of more than 5° is identified (11, 12). There are still little data on the medium- and long-term outcomes following operative treatment of these fractures using such criteria. Some evidence indicates that long-term outcome depends less on the fracture reduction per se, but rather on the achieved stability of the knee (2, 3, 13, 14). However, previous studies have often included heterogeneous fracture types, a combination of both operative and non-operative treatment, as well as rigid and non-rigid fixation with varying periods of immobilization (2–7). Moreover, most of these studies have lacked validated outcome measures.
The primary objective of the study was to determine the medium-term functional and radiographic outcomes of operatively treated AO B3.1 lateral tibial plateau fractures. The secondary objective was to evaluate how surgery and patient-related factors influence these outcomes.
Material and Methods
A chart review of all patients with operatively treated tibial plateau fractures that were admitted to our Level I trauma center between 1 January 2002 and 31 December 2008 was performed. A total of 389 patients were identified from the hospital database and their knee x-rays and computed tomography (CT) scans were reviewed and classified according to AO Foundation and Orthopaedic Trauma Association (AO/OTA) classification system. From this group, we identified 123 patients with AO/OTA type 41-B3.1 (split and compression) fractures treated with plate fixation. All patients had preoperative CT scans for accurate evaluation of fracture morphology. The indication for operative treatment of tibial plateau fractures in our clinic was articular displacement or step-off of more than 2 mm, condylar widening of more than 5 mm, malalignment of greater than 5°, or instability in full extension.
From these 123 patients, 73 (59%) were able to participate in a clinical and radiographic follow-up examination, 7 had died, 1 had undergone a total knee arthroplasty, 1 had suffered a pathological fracture, and 41 were lost to follow-up (11 were untraceable, 22 refused to participate, 3 had emigrated, and 5 had a language barrier). Hospital records, including operative reports and clinical notes, were reviewed to determine the nature of the injuries and complications of either the fracture or its treatment. The local Ethical Committee approved the study and informed consent was obtained from each subject.
The patient demographics are summarized in Table 1. Categorical data included patient gender and affected side; continuous data included patient age, follow-up time, time from injury to operation, duration of operation, and body mass index (BMI). The most common mechanism of injury was a same-level fall in 32 patients (44%). Other injury mechanisms were sports-related injury in 11 patients (15%), automobile collision with a pedestrian in 11 patients (15%), a fall from a height greater than 1 m in 7 patients (10%), and a road traffic accident in 6 patients (8%).
Patient demographics at medium-term follow-up of 73 patients with lateral tibial plateau fractures.
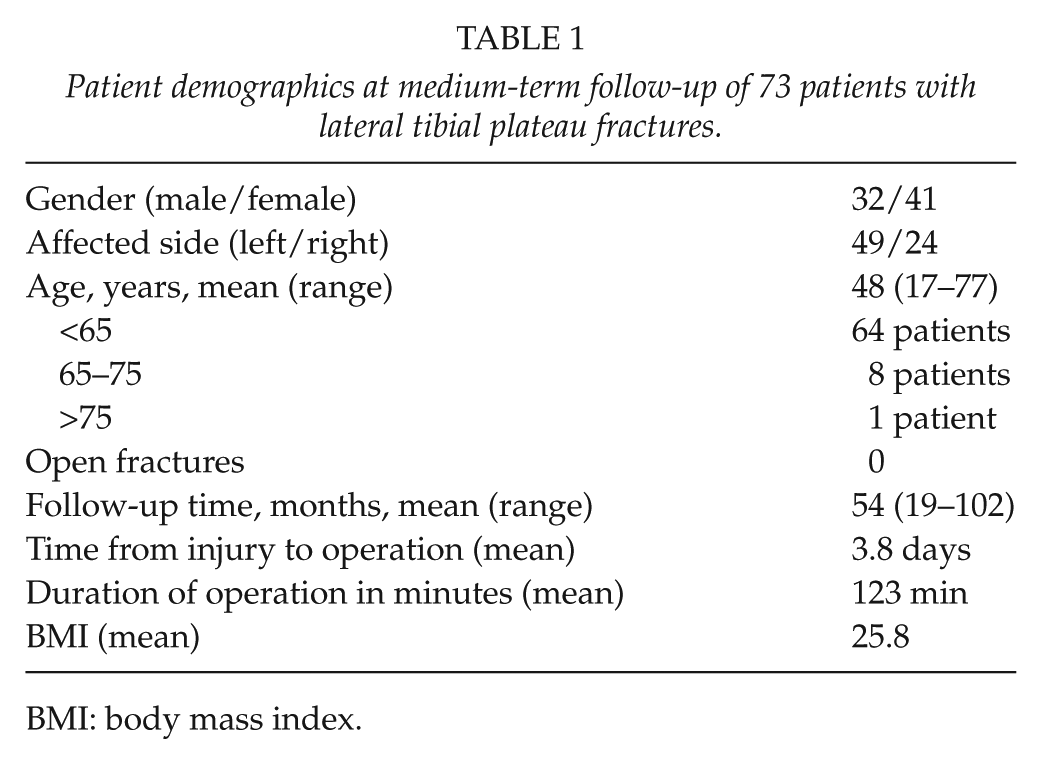
BMI: body mass index.
Operative Technique
All patients were treated by open reduction and internal fixation (ORIF) using an anterolateral incision, and an arthrotomy was performed beneath the lateral meniscus. Depression of the joint surface was elevated under visual control and the bone defect was filled with either autograft from the iliac crest (44 patients) or synthetic bone material (21 patients). In eight patients, the defect was minimal and no filling was used. In 28 patients, a conventional L-shaped buttress plate (Synthes, Bettlach & Grenchen, Switzerland) was used, and in the remaining 45 patients, internal fixation was performed using an angular stable locking plate (Less Invasive Stabilization System (LISS) Plate; Synthes, Bettlach & Grenchen, Switzerland; or L-shaped Locking Compression Plate; Synthes, Elmira, NY, USA). The postoperative management protocol included early mobilization using an orthosis. All patients were instructed to be non-weight bearing for the first 6–10 weeks, followed by partial weight bearing for a further 2–6 weeks, depending on the intraoperative assessment of fracture comminution and stability by the operating surgeon.
Clinical and Functional Evaluation
One independent orthopedic surgeon examined all patients at the follow-up visit. Valgus and varus laxity were evaluated using manual testing in extension and in 30° of flexion (15, 16). To assess anterior laxity, the Lachman, anterior drawer, and pivot shift tests were used (15). Posterior laxity was evaluated using the posterior drawer test (15). Range of motion was measured using a goniometer. Results were compared to the uninjured contralateral knee. All patients completed two validated functional outcome measurement tools: the Modified Lysholm knee score (17–19) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (20, 21).
Radiological Analysis
Conventional standing knee radiographs were taken to evaluate the stage of posttraumatic osteoarthritis at the end of follow-up. Radiographs were obtained with the knees extended and the tibias in neutral rotation. Standing knee radiographs were also obtained from the contralateral uninjured knee for comparison. Additionally, full-leg radiographs of the injured lower extremity were taken to evaluate the mechanical axis. The images were independently evaluated on clinical picture archiving and communications system (PACS) workstations (IMPAX DS 3000, version 4.5; Agfa-Gevaert N.V., Mortsel, Belgium) by two musculoskeletal radiologists and mean measurement values were used.
The stage of posttraumatic osteoarthritis was assessed according to the Kellgren–Lawrence classification (22): Grade 1—unlikely narrowing of the joint space, possible osteophytes; Grade 2—small osteophytes, possible narrowing of the joint space; Grade 3—multiple, moderately sized osteophytes, definitive joint space narrowing; and Grade 4—multiple, large-sized osteophytes, severe joint space narrowing, sclerosis, and/or deformity. The maximal depression of the tibial articular surface was also measured from anteroposterior and lateral view radiographs at the follow-up visit.
Statistical Analysis
Associations between categorical variables were tested with the chi-square test. Kruskal–Wallis or Mann–Whitney U-test was used to test the differences in continuous and ordinal variables between the levels of categorical variables. The correlation coefficients were calculated using Spearman rank-order correlations; p-values less than 0.05 were considered statistically significant. Statistical analyses were performed using SAS System for Windows, release 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
The mean WOMAC pain score was 10 (range = 0–66), stiffness score was 14 (range = 0–61), and function score was 10 (range = 0–59). The mean modified Lysholm score was 80 (range = 41–100). A total of 13 patients (18%) had medial collateral ligament (MCL) laxity, and 4 patients (5%) had anterior cruciate ligament (ACL) laxity. MCL laxity did not have an effect on Lysholm or WOMAC functional outcome scores (p = 0.086). ACL instability resulted in lower Lysholm scores (p = 0.011), but did not affect WOMAC scores (p = 0.112). There was full range of knee motion in 50 patients. Three patients demonstrated a minor extension limitation (5°–15°). Six patients had a flexion limitation of 20° or more (range 20°–45°). The mean sick leave from work was 3.8 months (range = 1.5–8.1 months). Full weight bearing was achieved at a mean of 10.9 weeks (range = 8–14 weeks).
Mechanical Axis
The mean mechanical axis of all 73 patients was 2° of valgus. The mechanical axis at follow-up did not correlate with WOMAC or Lysholm scores (Table 2). In all, 6 out of 12 patients (50%) who had more than 5° valgus malalignment at follow-up had developed severe (Kellgren–Lawrence grade 3–4) secondary osteoarthritis, compared to 1 out of 20 patients (5%) who had normal mechanical axis (p = 0.006). The measured amount of mechanical axis malalignment was not associated with clinical collateral ligament instability (p = 0.158).
The association between mechanical axis malalignment and clinical outcomes as well as the developed osteoarthritis at the end of medium-term follow-up in patients with lateral tibial plateau fractures.
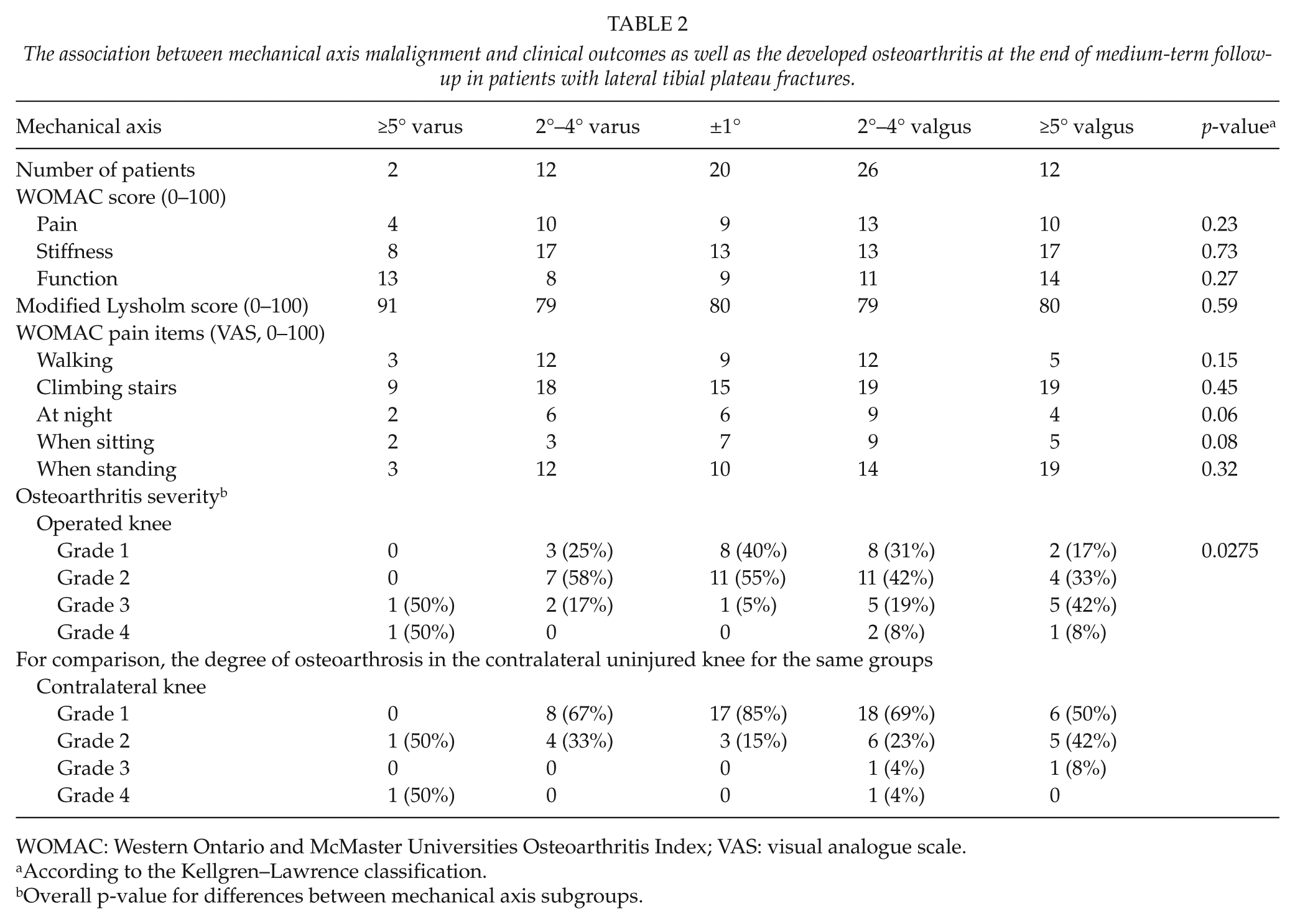
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; VAS: visual analogue scale.
According to the Kellgren–Lawrence classification.
Overall p-value for differences between mechanical axis subgroups.
Residual Articular Surface Depression
In all, 13 out of 29 patients (44%) who had more than 2 mm articular surface depression at follow-up had developed more advanced osteoarthritis (Kellgren–Lawrence grade 3–4) compared to 5 out of 44 patients (11%) who had a depression of 2 mm or less (p = 0.001) (Table 3). Articular surface depression of more than 2 mm was also found to be associated with more pain at night (p = 0.027) and pain while sitting (p = 0.013), and standing (p = 0.027). Similarly, articular depression of more than 2 mm was also associated with poorer WOMAC functional scores (p = 0.020). None of the patients had an articular depression greater than 7 mm.
The association between articular surface depression and clinical outcomes as well as developed osteoarthritis at the end of medium-term follow-up in patients with lateral tibial plateau fractures.
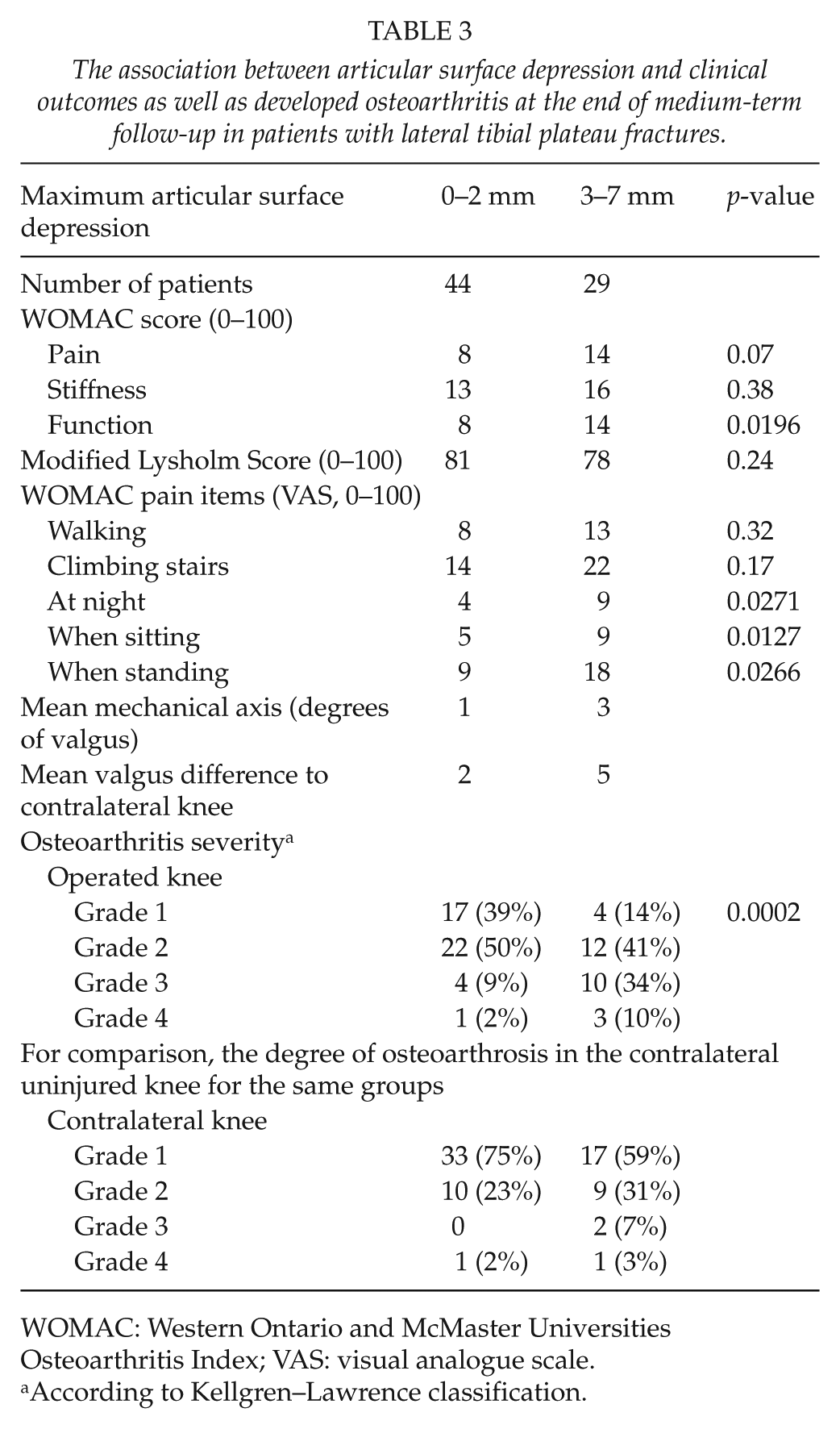
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; VAS: visual analogue scale.
According to Kellgren–Lawrence classification.
Bmi and Age at Trauma
BMI at the time of trauma was not found to be associated with valgus deformity (p = 0.697) or with joint depression at follow-up (p = 0.568), nor did it correlate with the functional outcome (p = 0.550, R = 0.07). Age at the time of operation was found to correlate with the stage of posttraumatic osteoarthritis. The older the patient, the more severe was the osteoarthritis seen at the follow-up (p = 0.002, R = 0.36). There was also a trend for older patients to have poorer WOMAC functional scores (p = 0.039, R = 0.24).
Bone Substitute, Surgeon, and Fixation Method
The type of void filler used (p = 0.537) or operative surgeon (resident or specialist) (p = 0.075) was not associated with mechanical axis, articular depression, or posttraumatic osteoarthritis. The use of an angular stable plate or buttress plate did not have an effect on radiological (p = 0.243) or functional (p = 0.361) results.
Complications
There were five early re-operations following index surgery due to postoperative malreduction or loss of reduction. Two patients developed compartment syndrome. Despite fasciotomy, this resulted in significant muscle necrosis of the anterior compartment due to delayed diagnosis. One of these patients also developed deep infection and required implant removal at 3 months postoperatively. Two patients sustained a permanent peroneal neuropathy probably due to distension of the nerve. Three of the patients suffered a deep vein thrombosis (DVT) despite pharmacologic prophylaxis (subcutaneous enoxaparin 40 mg/day).
Discussion
The first aim of this study was to determine the medium-term functional outcome and radiographic results of operatively treated lateral tibial plateau fractures. Overall, the patients in this study had a good recovery following surgical treatment of their injury. The mean WOMAC score at follow-up was similar to population-based normative values (23). The mean modified Lysholm score was good, and similar to other studies evaluating patient recovery after operative treatment of lateral tibial plateau fractures (24, 25).
The second objective of the study was to evaluate how surgery and patient-related factors influence the clinical and radiographic outcomes. In this study population, 18% of patients had MCL laxity at follow-up. This was a similar level to what has been previously noted in a study by Ali et al. (11) evaluating failure of fixation after operatively treated AO types B and C fractures of the proximal tibia. Knee instability has previously been noted to be important factor influencing the functional outcome following tibial plateau fractures (12). However, residual MCL instability was not found to be associated with functional outcome scores in this study. On the other hand, 5% of the patients in this study had residual ACL laxity, which was associated with poorer Lysholm scores.
In the study by Rademakers et al. (6), it was also noted that 31% of patients had secondary osteoarthritis that had developed at a mean of 14 years follow-up time. They found that patients with mechanical axis malalignment of more than 5° developed a moderate to severe grade of osteoarthritis more often than patients with an anatomic knee axis as evaluated from standing knee radiographs (27% vs 9.2%). A noteworthy finding of this study was that patients with residual valgus malalignment of 5° or more had already developed significantly more severe posttraumatic arthritis at medium-term follow-up. This would suggest that the detrimental consequences on the articular surface due to such a mechanical disadvantage may begin at a very early stage.
Several studies have found that residual depression of the articular surface is not an important factor in predicting the functional outcome (2, 3, 26, 27), or the development of secondary osteoarthritis (6). We found that when there was more than 2 mm depression on the articular surface, there was significantly more severe posttraumatic osteoarthritis according to the Kellgren–Lawrence classification. Articular depression of more the 2 mm was also associated with poorer WOMAC functional scores and visual analogue scale (VAS) pain scores in this study. However, these results should be interpreted with caution since the differences in mean VAS pain and WOMAC scores were statistically significant but differences were small and probably not clinically relevant (28, 29).
The age of the patient at the time of trauma has previously been noted to be an important factor in predicting the functional outcome at follow-up. It has been noted that older age predicts worse functional outcome (26). Similarly, we found that older patients had more advanced secondary osteoarthritis and poorer WOMAC functional scores at follow-up when compared with younger patients.
Russel and Leighton (30) have shown in a prospective randomized study of 119 patients with Schatzker I–VI type of fracture that bioresorbable calcium phosphate cement gives better results defined as prevention of fracture subsidence compared to autogenous iliac bone graft. We found no difference in the radiological results (articular depression, mechanical axis) according to used void filler. However, the use of angular stable fixation in the majority of patients may be a confounding factor.
To our knowledge, this is the largest study examining the medium-term outcomes of AO type B3.1 fractures of proximal tibia. An important strength of this study was the use of two validated patient-reported outcome assessment tools (WOMAC and Lysholm). Furthermore, pain severity was assessed in several clinically relevant situations using a VAS. An additional strength was the use of a standardized operative technique and postoperative rehabilitation protocol for all patients.
This study had some limitations. Being a medium-term follow-up study, the follow-up time was relatively short. Another limitation was that 33% of the patients were lost to follow-up, yet this level is similar to other studies (6, 12, 25). Measurement of articular depression at the follow-up visit was performed from plain radiographs. This is challenging and can be associated with errors and is acknowledged as a limitation (31, 32). Furthermore, due to the variable quality of postoperative supine radiographs, it was not possible to reliably determine whether the articular depression at follow-up had resulted from initial fracture malreduction or postoperatively. The use of CT both postoperatively and at the follow-up visit could have enabled a more reliable assessment of articular depression in the prospective setting (32). Finally, the retrospective study design has inherent limitations with regard to adjustment for all possible confounders. Factors such as initial dislocation, cartilage injury, and trauma energy as well as patient comorbidities may also affect the outcome of these fractures. However, the selection of only one specific fracture type in this study was done to minimize the effects of heterogeneous fracture patterns on these outcomes.
Based on the findings of this study, there is an association between both articular surface depression and valgus deformity with the development of posttraumatic osteoarthritis. Osteoarthritic changes develop slowly in years. It is possible that with longer follow-up, progression of posttraumatic changes in the joint surface will reach a clinically relevant threshold with associated effects on functional outcome. The development of severe posttraumatic osteoarthritis may eventually even require total joint arthroplasty. There are very little data on the incidence of total knee replacement following fractures of the tibial plateau and this would be an interesting focus for future studies.
Conclusion
The postoperative articular congruity and normal mechanical axis of the lower leg after plate fixation in lateral tibial plateau fractures seem to have a role in prevention of posttraumatic osteoarthritis but does not appear to predict clinical outcome at medium-term follow-up.
Footnotes
Acknowledgements
The authors would like to thank Tero Vahlberg (biostatistician at the University of Turku) for performing the statistical analyses.
Declaration of Conflicting Interests
The study sponsor had no influence or involvement in the study.
Ethical Approval
The local Ethical Committee approved the study (DNRO 423/13/03/02/2009) and an informed consent was obtained from each subject.
Funding
This work was supported by Helsinki University Central Hospital (EVO).