
Abstract
Introduction:
Emergency surgery is performed on patients with appendicitis in the belief that inflammation of the appendix may progress to necrosis and perforation. Many cases of appendicitis, however, resolve with conservative treatment, and necrotic appendicitis may represent a different disease rather than the end result of inflammation of the appendix. We wished to explore the relationship between the interval to surgery after admission to hospital with appendicitis and the proportion of patients developing necrosis.
Methods:
Appendicectomy operations performed between 2005 and 2010 were reviewed. End points included age, sex, interval from admission to surgery, and final pathological diagnosis.
Results:
A total of 2403 evaluable patients were identified (1266 females). Necrotic appendicitis occurred more commonly in children (17.5%) and the elderly (25.4%) compared with adults (10.5%). The median interval to surgery of patients with normal histology (17.1 h) was longer than the time to removal of inflamed (13 h) or necrotic (13.5 h) appendices (p < 0.001).The ratio of necrotic to inflamed appendicitis in the entire cohort was 0.24. Multivariate analysis reveals that necrosis of the appendix is more common in children and the elderly and that the proportion of patients with necrosis does not change with increasing interval to surgery.
Discussion:
Our observations show that appendicitis is not more likely to lead to perforation if a short delay prior to surgery is allowed. In addition, our findings add weight to the increasing volume of data showing that necrosis of the appendix is a disease different from simple inflammation.
Keywords
Introduction
The management of patients presenting with the clinical features of acute appendicitis is a common and challenging surgical problem. Most surgeons intervene early in patients where appendicitis is suspected, and removal of a normal appendix is considered to be an acceptable price to pay to avoid leaving a necrotic appendix in situ. This aggressive surgical policy is adopted because of the belief that inflammatory appendicitis is a progressive disease leading to necrosis and perforation, a complication with a high mortality (1). The hypothesis that appendicitis is a single disease entity with progressive inflammation leading to necrosis and perforation has not been tested, however, as it is difficult to study the natural history of the disease in the era of readily available surgery. An alternative explanation is that inflammation and necrosis of the appendix represent different disease processes. Rarer pathological processes can also occur in the appendix, including carcinoid disease and infestation (2, 3).
Evidence for a different aetiology of inflammatory and necrotic appendicitis comes from different incidence across age groups. Necrotic appendicitis has consistently been shown to be more common in children (4) and the elderly (5). This difference is often explained by the difficulty in making a diagnosis in these age groups leading to a longer interval to surgery with progression of the inflammatory process to necrosis and perforation (6–9). The evidence supporting this disease mechanism comes from small series examining the onset of symptoms retrospectively and is subject to recall bias.
Patients presenting with symptoms suggestive of appendicitis in the United Kingdom are rarely subjected to surgery immediately. One of the standard treatment options in patients presenting with right iliac fossa pain and tenderness is to adopt a policy of active observation with reassessment of clinical signs as these can become clearer and more helpful in making a diagnosis of appendicitis. Furthermore, in the United Kingdom, most emergency surgery is avoided between the hours of 24:00 and 08:00 following implementation of national guidelines (10). This leads to many patients waiting overnight for surgery. Therefore, there is potentially a significant time interval between admission with symptoms and surgery for patients with suspected appendicitis. This allows us to explore the relationship of the time interval to surgery with the proportions of patients suffering inflammation and necrosis of the appendix.
Methods
Derriford Hospital Performance Information System was interrogated for discharge dates between January 2005 and December 2010. Details of all patients with a recorded procedure of appendicectomy during their hospital stay were retrieved. Demographic details were scrutinized along with time of admission, time of surgery, and reason for appendicectomy. Details were cross-referenced with final pathology reports and the pathological diagnoses categorized as “normal,” “inflamed,” “necrotic,” or “other.” Inflammation of the appendix was identified by the presence of infiltrating neutrophil polymorphs within the appendix beyond blood vessels and necrosis by the loss of cellular structure and nuclei. Patients with perforation of the appendix were included in the “necrotic” category. Patients in whom the appendicectomy was performed as part of another procedure or as an elective operation were excluded. To assess the age effect on pathology outcome, the cohort was split into groups determined by age decades. For categorical analyses, the cohort was split into three age groups: 0–10 years (“children”), 11–50 years (“teenagers and adults”), and 51–90 years (“elderly”). Children above the age of 10 years were included in the middle category as an initial study revealed that above this age, the rate of appendicectomy increases dramatically and is closer to that of young adults than younger children (Fig. 1). In addition, the mean age of menarche in the United Kingdom is 12 years and is rare in girls under 10 years (11). There is also a decline in the rate of appendicectomy after the age of 50 years, and these intervals include women of reproductive age in a single category. Between-group analyses were performed by chi-square test. The median time interval to surgery between groups was compared using Kruskal–Wallis test. The closest curve was fitted to the scatter plot data by the locally weighted scatter plot smoothing (LOWESS) method (12). Multivariate logistic regression analysis was used to investigate the effect of the interval to surgery and patient age on the final pathology outcome. In the regression model, the pathology outcome was calculated as log ratio (necrosis count/inflammation count) for different age groups and intervals to surgery. In order to assess the performance of the model, it was fitted to 70% of the dataset and used to predict the outcome probability for the remainder of the dataset. The goodness of fit (GOF) was assessed by the Hosmer and Lemeshow GOF test (13), and Pearson chi-square test was used to show any difference between predicted and observed ratios. A p-value below 0.05 was considered significant. The statistical analysis of data was performed with the statistical software R 2.14.1 (14).
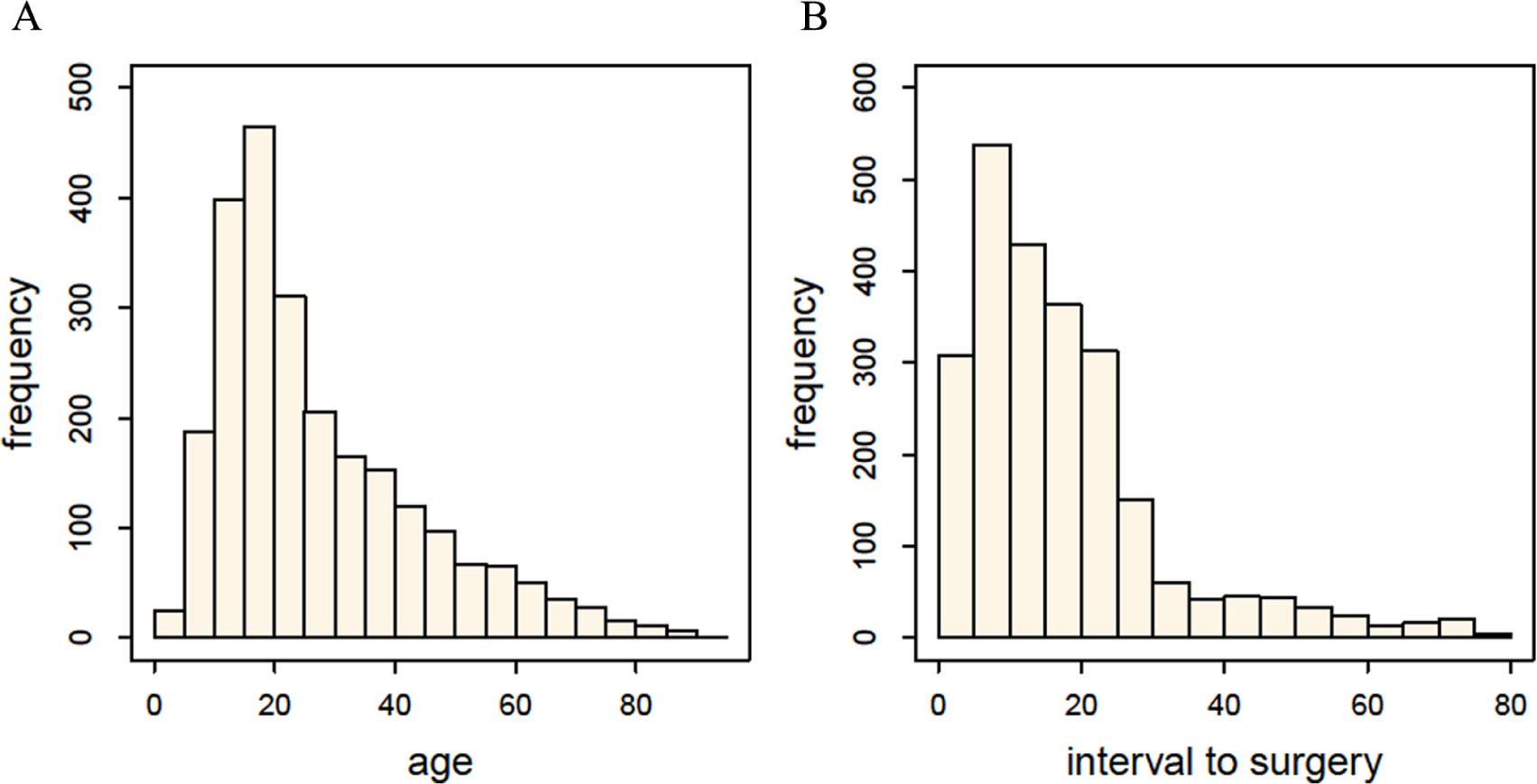
Histogram of A) age of patients and B) interval to surgery among 2403 patients undergoing emergency appendicectomy.
Results
Initial analysis revealed that 2692 patients underwent appendicectomy between 2005 and 2010. The excluded patients were 225 patients in whom the appendicectomy was not the main procedure, 16 patients for whom the histology report could not be located, and 13 patients in whom the procedure was performed electively. In addition, 35 patients with an interval to surgery of more than 84 h were also excluded to facilitate statistical analysis, leaving 2403 patients who form the study group. The diagnoses of the excluded group were similar to the cohort as a whole, revealing 13, 11, 7, and 4 cases showing inflammation, normal appendix, necrosis, and “other” diagnoses, respectively. The distributions of patient age and interval to surgery are shown in Fig. 1. The median age of the cohort was 22 years, and 95% of patients were aged between 7 and 71 years. The median interval to surgery was 14.4 h, and 95% of patients had surgery between 2 and 60 h after admission.
The study group included 1266 females (median age = 22 years) and 1137 males (median age = 22.5 years) in the following age groups: 0–10 years (n = 212), 11–50 years (n = 1912), and 51–90 years (n = 279). Review of histology reports revealed inflammation only in 1292 (53.8%) patients, a normal appendix in 662 (27.6%) patients, necrotic or perforated appendicitis in 308 (12.8%) patients, and other diagnoses in 141 (5.8%) patients. Among the last group, the most common diagnoses were parasitic infestation (43), fibrous obliteration (24), and carcinoid disease (18). Among the 1600 patients with appendicitis, the ratio of necrosis (308) to simple inflammation (1292) was 0.24 and did not differ between males (0.25) and females (0.22). Significant variations in pathology outcome of appendicectomy specimens were noted, however, according to patient age and gender subsets (Table 1 and Fig. 3A). The highest rate of removal of a normal appendix occurred in adult females (39.1%), and the rate of removal of normal appendices was low in elderly males (9.2%) and females (9.5%). The rate of removal of inflamed specimens is similar across age groups (52.4%–57.3%). Necrotic appendicitis occurred more commonly in pathology specimens from both children (17.5%) and the elderly (25.4%) compared with adults (10.5%) (p = 0.01 and p < 0.001).
Number (percentage) of children, adult, and elderly patients with different pathological diagnoses identified after 2403 emergency appendicectomy operations.
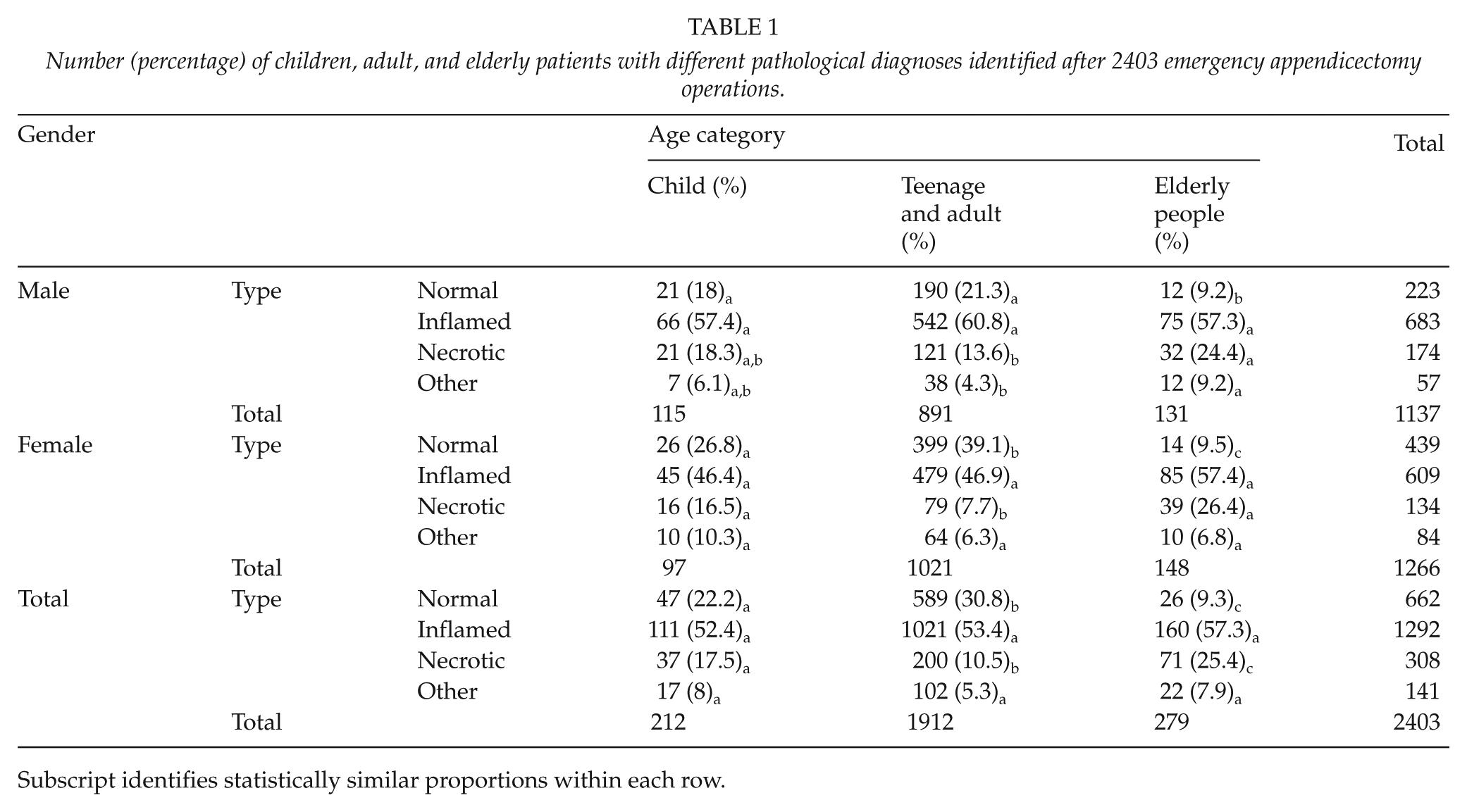
Subscript identifies statistically similar proportions within each row.
The median time to surgery from admission was 11.7, 13.9, and 17.2 h for the 0–10, 11–50, and 51–90 age groups, respectively (p < 0.0001). For adult age groups, the median interval to surgery was longer for female patients (16.75 h) than male patients (11.53 h) (p ≤ 0.001). The median interval to surgery of patients with normal histology (16.8 h) was significantly longer than the time to removal of inflamed (12.8 h) or necrotic (13.4) appendices (p < 0.001) in the whole population. The median interval to removal of a necrotic appendix was similar to that of removal of an inflamed appendix in children (11.2 vs 10 h; p = 018), adults (11.8 vs 12.6 h; p = 0.62), and the elderly (15.3 vs 18.4 h; p = 0.5) (Fig. 2). The ratio of necrotic appendicitis to simple inflammation was 0.24, 0.22, 0.27, 0.34, 0.21, and 0.10 among appendicectomy specimens removed in the consecutive time intervals addressed in the study (the final two time interval categories were combined for analysis purposes as there were no cases of necrotic appendicitis in the >72-h category) (Fig. 3B).
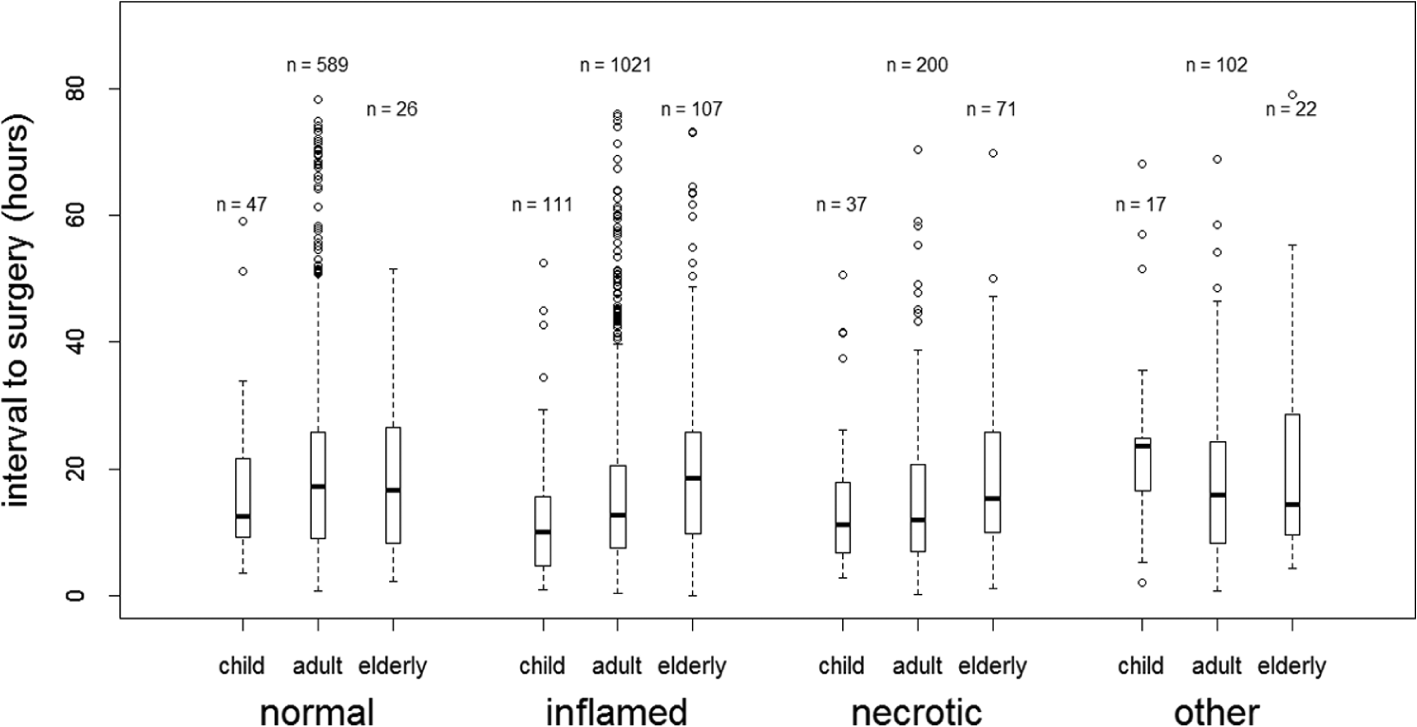
Median interval to surgery determined by age group and pathology outcome in 2403 patients undergoing emergency appendicectomy.
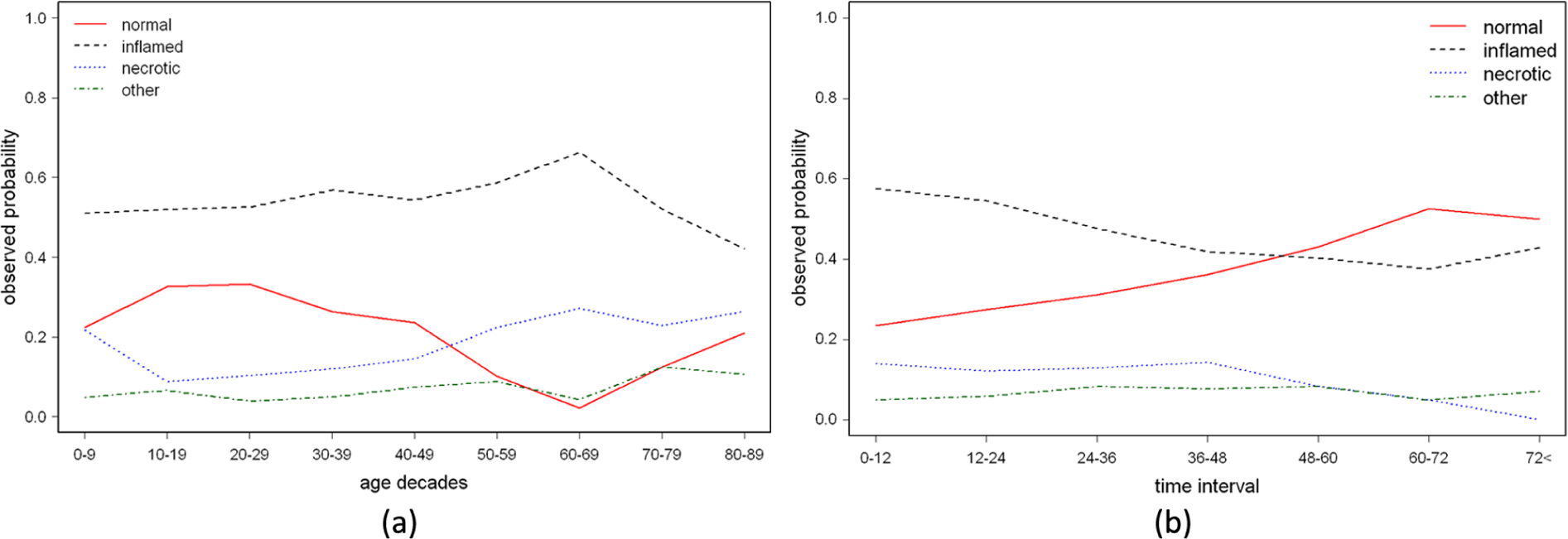
Variation of the probability of the occurrence of different pathology outcomes with A) age and B) time interval to surgery among 2403 patients undergoing emergency appendicectomy.
Evaluation of Effect of Age and Interval to Surgery on Pathology Outcome
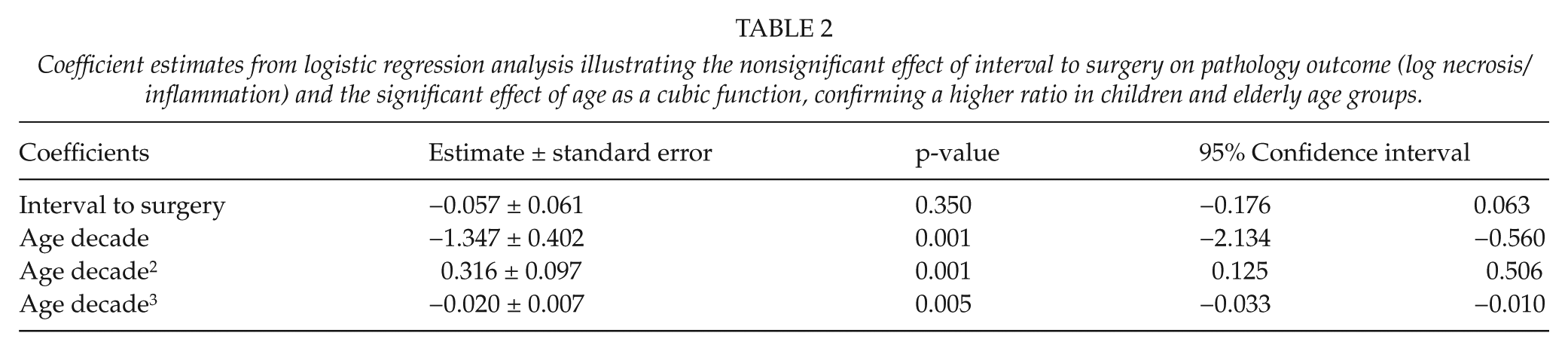
Fig. 4A,B illustrates the log ratio (necrosis count/inflammation count) against patient age and interval to surgery with fitted LOWESS curves of the 1600 patients with appendicitis. The curves show a small fall in the ratio of necrotic specimens to inflammatory specimens with increasing interval to surgery and that the proportion of necrotic specimens is higher in children and the elderly. Results from logistic regression analysis shown in Table 2 confirm a significant variation of the log ratio of necrotic specimens to inflammatory specimens with age. The curve equation is cubic, confirming a higher proportion of necrotic specimens in children and the elderly (p = 0.001). In contrast, logistic regression analysis reveals that the pathology outcome does not change significantly with increasing interval to surgery (p = 0.35).
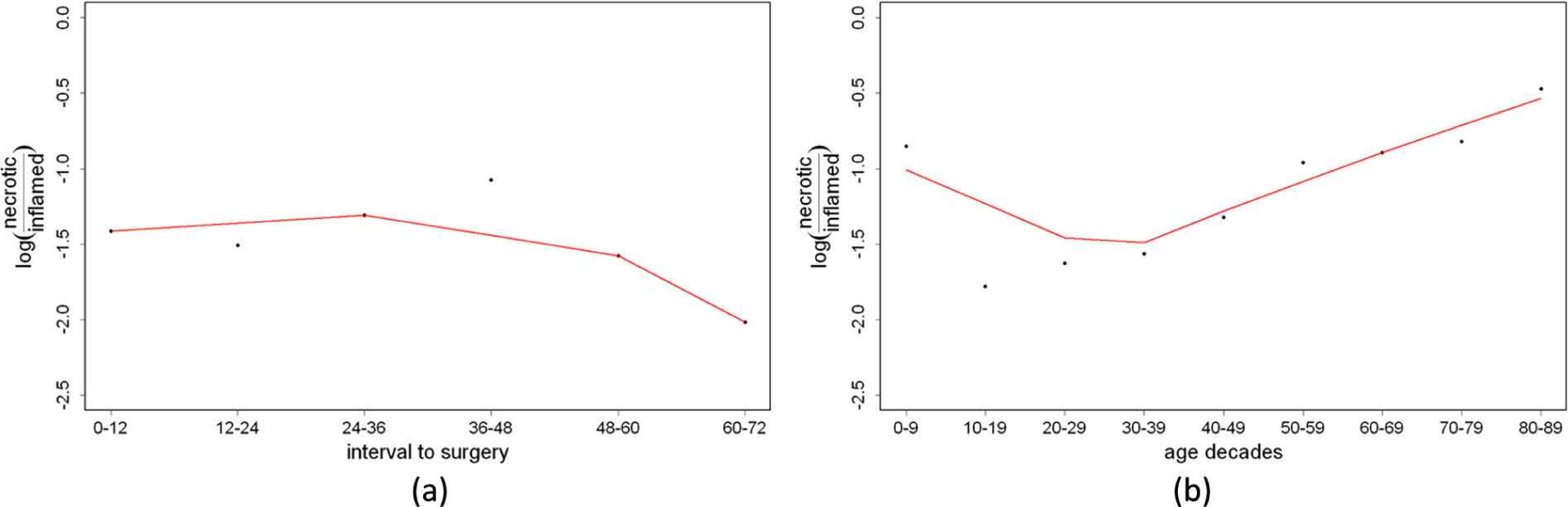
Scatter plot of the ratio of necrotic to inflamed appendicectomy specimens against A) time interval to surgery and B) age.
Coefficient estimates from logistic regression analysis illustrating the nonsignificant effect of interval to surgery on pathology outcome (log necrosis/inflammation) and the significant effect of age as a cubic function, confirming a higher ratio in children and elderly age groups.
Discussion
This study describes a systematic examination of the influence of age, gender, and interval to surgery on the pathological outcome of the resection specimen in a large cohort of patients undergoing appendicectomy and reveals a number of findings:
There is a higher proportion of necrotic appendicitis in children and the elderly people.
Children undergo surgery more quickly after admission than adults or the elderly.
A longer interval to surgery after admission is associated with a higher chance of removal of a normal appendix.
The proportion of patients with appendicitis who have necrosis is not affected by the interval to surgery after admission.
We used hospital performance data to identify patients who have undergone an appendicectomy. This study is unusual among registry-based studies, however, in that the pathology details were checked for all patients in the register to confirm the diagnosis and to exclude patients undergoing an incidental or elective appendicectomy. After this validation process, 237 patients (8.1% of the initial group) were excluded. The study used the time of hospital admission as the start point of the interval to surgery as this is a fixed time point which is prospectively recorded by audit staff. Although the start of symptoms is also a logical starting point of this interval, it is not routinely recorded, may be gradual in onset, and is subject to recall bias. Use of the interval from admission to surgery allowed assessment of a portion of the natural history of the disease by a consistent technique in a large number of patients.
The most important findings of this article relate to the pathology of acute appendicitis. The study confirms earlier findings that there is an increased proportion of necrotic or perforated appendicitis in children and the elderly (4, 5). These data do not, however, allow us to make any comment regarding the incidence of necrotic appendicitis in different age groups as our data are shown as a proportion of patients having an appendicectomy and therefore can be affected both by the incidence of patients with inflammatory appendicitis and the size of the population at risk. A large meta-analysis of studies examining the natural history of appendicitis in 53,143 patients, however, showed no association between age and the incidence of necrosis of the appendix (15).
Previous studies have shown that necrosis of the appendix occurs relatively more commonly in children and the elderly because of the difficulty in making a diagnosis in these age groups, leading to a delay in treatment and progression of the disease (6, 16–18). An alternative hypothesis is that simple inflammatory appendicitis and necrosis represent different diseases, or different patient response to disease, with distinct epidemiology and natural history. Support for this hypothesis comes from population studies which have revealed a steady decline in the incidence of simple inflammatory appendicitis between 1970 and 1995 while the incidence of necrosis of the appendix slowly increased (19). More recently, an increase in the incidence of simple inflammatory appendicitis has been noted which has coincided with the increasing use of computed tomography (CT) scans in the diagnosis of the disease. This imaging modality has had a dramatic effect on the rate of appendicectomy in areas where it is used routinely, suggesting that many patients are now operated on whom previously would have been treated conservatively (20). Population studies have also revealed that the incidence of inflammatory appendicitis, but not necrotic appendicitis, varies in a similar fashion to acute diverticulitis and may have a similar aetiology (21). The incidence of inflammatory appendicitis varies across geographical areas and appears to be related to the number of appendicectomy operations undertaken (15). There is good epidemiological evidence, therefore, that inflammatory and perforated appendicitis represent different diseases. Further clinical evidence supports the two-disease hypothesis of appendicitis. Trials have shown that surgery is not essential in the treatment of appendicitis, and a number of series have shown similar outcomes with conservative management (22, 23), which have been summarized in a systematic review (24). In all such series, however, a proportion of cases fail with conservative treatment, often due to the development of necrosis. It is likely that conservative treatment is effective and appropriate for patients with simple inflammation but not for patients with necrosis.
The view that inflammation of the appendix leads inevitably to perforation is the justification for undertaking surgery as an emergency. Indeed, the rate of necrosis of the appendix has even been used as an indicator of quality in the care of pediatric patients with appendicitis (25). Our data, however, show clearly that the risk of developing necrotic appendicitis is not related to the time interval to surgery after admission. This finding has important implications for clinical practice as it removes the justification for performing an emergency appendicectomy immediately after admission to hospital, or at night, in order to prevent perforation of the appendix. The largely constant ratio of necrosis to simple inflammation in appendicectomy specimens removed in the first 72 h of hospital admission in our series suggests that the pathological outcome of the disease is determined before patients are admitted to hospital. If necrosis of the appendix presented with more striking clinical features, we would expect to see a decline in its incidence over time after admission as the more severe cases were treated quickly. The data show, however, that surgeons are no better at diagnosing and treating necrosis of the appendix than simple inflammation, suggesting that their presenting features are similar. Similarly, the view that necrosis of the appendix is proportionately more common in children due to difficulty in making a diagnosis is not supported by this evidence, as children undergo surgery more rapidly after admission than adults or the elderly.
Our results add weight to the increasing volume of data showing that necrosis of the appendix is a disease different from simple inflammation and provide evidence to support guidelines which allow a short delay prior to surgery. These results also have implications for a policy of treating appendicitis conservatively, as it appears to be difficult to distinguish the two pathological processes by clinical evaluation.
Footnotes
Acknowledgements
The authors would like to acknowledge Mr Alex Wilkins, Mr Stephen Fry, Mr Daniel Couch, Mr James Brewer, and Dr Mark Mordue for their efforts and assistance in reviewing and collating the pathological reports for this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.