
Abstract
Background and Aims:
Appendicitis is a common presentation to hospital with appendectomy being the treatment of choice. Pre-operative administration of broad-spectrum antibiotics is common, but obtaining intra-abdominal pus samples is not. After an initial 6-month retrospective audit and departmental teaching on the importance of intra-peritoneal pus sampling, we aimed to determine whether intra-operative pus samples changed antibiotic management.
Materials and Methods:
Following the initial audit cycle, a 6-month prospective cohort study was conducted. Clinical data were collected on a predetermined proforma to assess the effectiveness of the intervention and antibiotic prescribing practice. The data collected during the whole 1-year period was analyzed.
Results:
During the 1-year period, 440 patients were identified as undergoing a laparoscopic procedure. After exclusion, 261 patients were identified as undergoing laparoscopic appendectomies, of which 141 (54%) were classified as complicated laparoscopic appendectomies. A total of 35 out of 141 (25%) pus samples were sent of which 24 (17%) resulted in positive cultures, with only nine of these positive cultures reported prior to the patient being discharged. No patient had their antibiotic regimen changed as a result of the culture results. There were three cases of cultures resistant to local antibiotics, but without significant clinical outcome. One of these patients developed a post-operative complication, but the antibiotic regimen was changed to broad spectrum rather than a specific antibiotic based on culture sensitivity. Of the 141 patients with complicated laparoscopic appendectomies, five (3.5%) developed post-operative complications: one readmission requiring a laparoscopic washout for pelvic collection, three (2%) cases of pelvic collections managed conservatively, and one case of prolonged paralytic ileus managed non-operatively.
Conclusion:
Overall, none of the patients with positive cultures had a change in prescribed antibiotics based on culture results. Hence, the routine practice of intra-peritoneal pus sampling following complicated appendicitis remains of little clinical value.
Introduction
Appendicitis is the commonest cause of an acute abdomen, with a lifetime risk of 6%–20% in the United Kingdom (1). Appendectomy is the treatment of choice and is increasingly being performed as a laparoscopic procedure (1). Patients managed non-operatively have more subsequent visits to the emergency department and frequently have an appendectomy performed (2).
Pre-operative administration of intravenous broad-spectrum antibiotics is common practice (3). Current guidelines in our hospital suggest co-amoxiclav and a single dose of gentamicin initially, followed by ongoing co-amoxiclav only in complicated appendicitis. Pre-operative administration of broad-spectrum antibiotics is common practice, but some surgeons advocate abandoning intra-peritoneal cultures during appendectomy (4). The development of intra-peritoneal abscess collection is a well-known complication of appendicitis post-operatively which is associated with increased morbidity, and the use of pus samples may allow us to target antibiotics in its management and reduce readmissions. Antibiotic use in appendicitis started when bacterial etiology was demonstrated in studies where culture swabs were obtained routinely during appendectomies and guided antibiotic use (5). Although current antimicrobial therapy use has become prophylactic, empirical, and broad spectrum, this age-old practice still remains.
An initial 6-month (January 2016–June 2016) retrospective audit on outcomes of patients with complicated appendicitis was conducted. Due to low pus sampling and continued post-operative complications, it was postulated that the complications could be as a result of inappropriate antibiotic usage from lack of intra-peritoneal sampling. Departmental teaching was delivered on the significance of pus sampling during laparoscopic appendectomy for complicated appendicitis to increase the number of intra-operative pus samples sent for microbiological analysis. Our study sought to understand the relevance of traditional practice of pus sampling in complicated appendicitis and to assess whether there is a change in antibiotic prescribing practice in accordance with culture sensitivity.
Materials and Methods
All patients who had a laparoscopic appendectomy over a 1-year period (January 2016–December 2016) were identified using TheatreMan software (a prospectively maintained electronic record of all hospital operations maintained by theater staff, Trisoft, United Kingdom), combining both the pre- and post-intervention groups. Patients who were listed for a laparoscopic appendectomy, diagnostic laparoscopy, or a combination of both were included.
Data on histology, microbiology cultures, and post-operative imaging were collected from Integrated Clinical Environment (Sunquest, USA). Data from operation notes, drug charts, and clinical notes were collected from Evolve (Kainos, UK). Particular data points recorded included intra-operative findings, histology results, microbiology results, antibiotic use, complications, length of stay, and readmissions.
Data from pre- and post-intervention regarding the collection of pus samples from patients with complicated appendicitis were analyzed. Culture results from pus samples, over the whole 1-year period, were compared with antibiotics given to the patient. All patients with complicated appendicitis, defined as macroscopic free pus or perforation on operation note, or perforation or gangrenous on histology report, were included for analysis. Mean and range were calculated for statistics. The study was reported in accordance with the STROBE (strengthening the reporting of observational studies in epidemiology) guidelines (6).
Ethical approval was not necessary for this study due to its initial retrospective observational nature. It assessed clinical practice and no changes were made to patient clinical management as a result of the study during the prospective period.
Results
Over the 1-year period, 440 patients undergoing laparoscopic procedures were identified from TheatreMan. Of the 440 patients, 142 were excluded for having a different diagnosis, normal appendix, or other reason for the operation. A further 37 patients were excluded for having a previous appendectomy, operation cancellation, no availability of notes or pathological sample and being listed wrongly. Finally, 120 patients were excluded for having uncomplicated appendicitis leaving 141 patients with complicated appendicitis to be analyzed (Fig. 1).
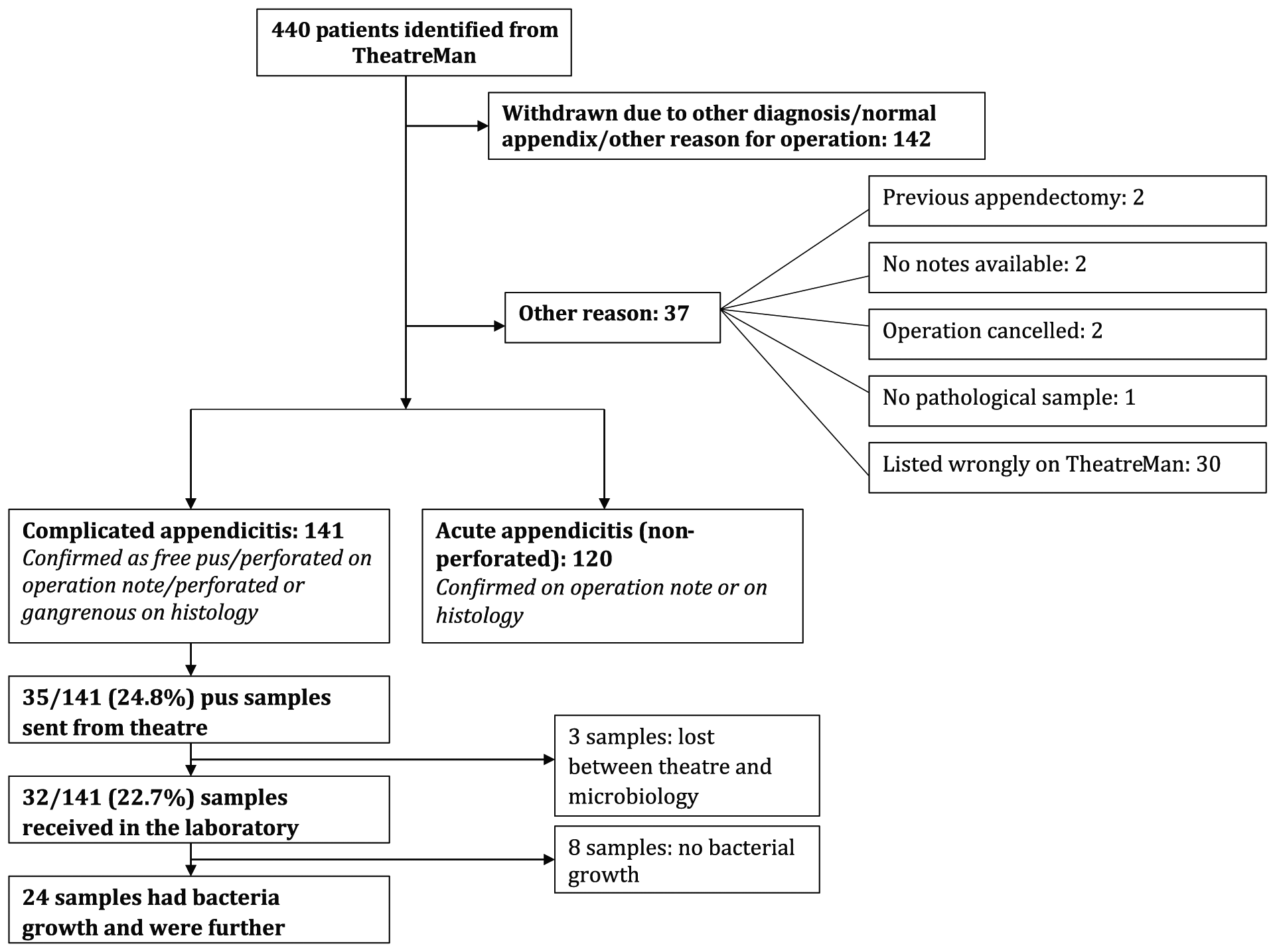
Patients included and excluded from this study.
The notes and clinical details of 81 male and 60 female patients were reviewed. The mean age was 37.2 (range: 4–90 years old, Table 1). The pus-sampling rate in the retrospective audit was 17.8%. This increased to 50% in the first month following intervention. However, the sampling rate dropped to 28.6% over the subsequent 5 months.
Patient demographics and overall complication rate.
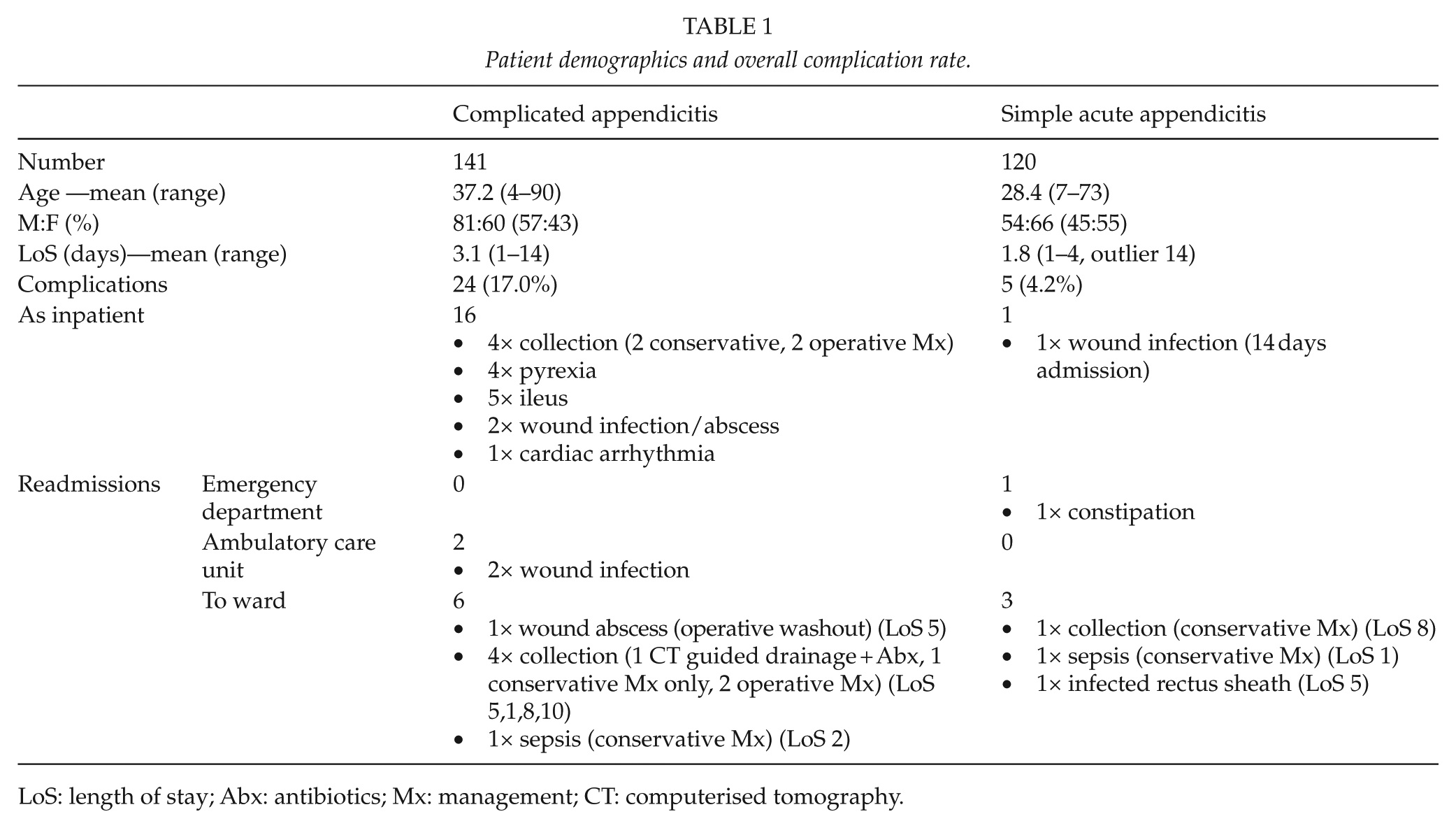
LoS: length of stay; Abx: antibiotics; Mx: management; CT: computerised tomography.
Of the 141 patients with complicated appendicitis, 35 (25%) had pus samples collected intra-operatively. Three of these samples were unfortunately not received at the laboratory. Bacterial growth was present in 24 of the samples; however, nine of these had no sensitivities reported. Fifteen pus samples were therefore analyzed and compared with antibiotics received by the patient. Culture growth was sensitive to the prescribed antibiotics in 11 of the 15 patients. Therefore, four patients were given antibiotics that were ineffective against the organism grown in their sample. Only one of these four patients developed a complication post-operatively which was a collection. However, the patient was treated with a broad-spectrum antibiotic, Tazocin (piperacillin and tazobactam), rather than an antibiotic listed on the sample sensitivities.
Of the 24 patients with pus samples sent, complications occurred in five of them. Intra-abdominal collections developed in four of the patients, of which one patient required intra-abdominal washout, and another received drainage under computed tomography guidance. The other two patients were managed conservatively with broad-spectrum intravenous antibiotics (co-amoxiclav). They all made an uneventful recovery and their pus culture results did not alter the management of these patients (Table 2).
Pus culture results summary.
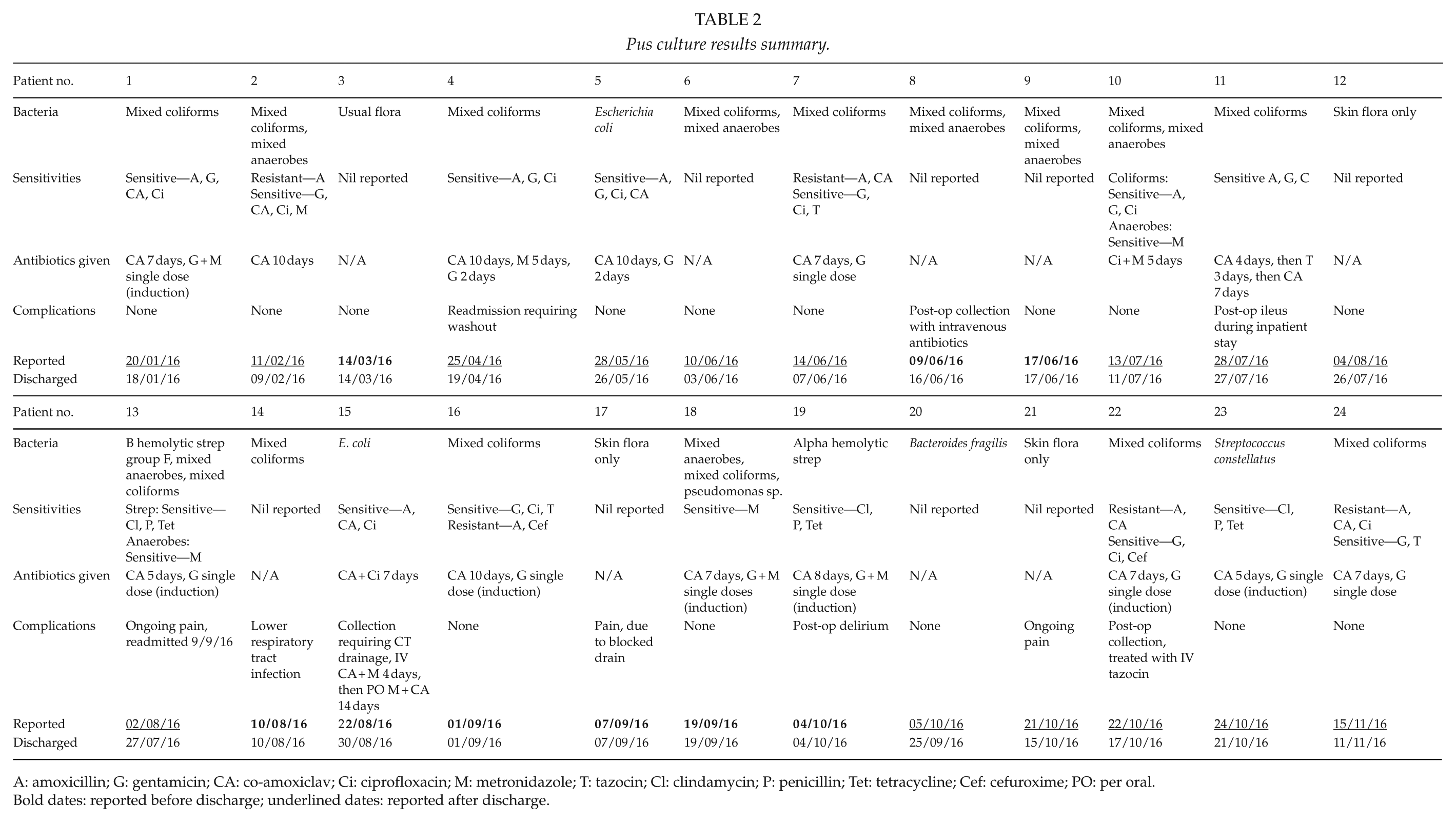
A: amoxicillin; G: gentamicin; CA: co-amoxiclav; Ci: ciprofloxacin; M: metronidazole; T: tazocin; Cl: clindamycin; P: penicillin; Tet: tetracycline; Cef: cefuroxime; PO: per oral
Bold dates: reported before discharge; underlined dates: reported after discharge.
Only nine of the 24 positive cultures were reported prior to discharge of the patient, with seven of these reported on the day of discharge.
Discussion
Obtaining pus samples to send off for microscopy, culture and sensitivity is often carried out in clinical practice to enable targeted antibiotic prescribing, effective against the causative organism. Our study found that of the 141 patients undergoing laparoscopic appendectomy for complicated appendicitis, 15 of the 35 pus samples sent had positive growth and sensitivities reported, and therefore analyzed. No patient had their antimicrobial regimen changed in light of the culture results.
The commonest organisms in appendicitis have been suggested by previous studies to be Escherichia coli and Bacteroides fragilis (5). Previous studies have shown that the majority of causative organisms are sensitive to empirical antibiotics prescribed with a sensitivity rate of 68%–97% (7–10). This correlates with the findings of this study, which found a sensitivity rate of 73% to empirical antibiotics.
Issues arise when patients develop a collection post-operatively or when their causative organism is resistant to the antibiotic they received. However, in our study, four patients had culture results which were resistant to the antibiotics they had been prescribed. Despite this, they did not have their antibiotic regimen changed in light of their culture results due to the results being reported after discharge in three cases, on the day of discharge in one case and the patients appearing clinically well. They developed no complications. This may be due to other interventions such as pre-operative antibiotics and thorough intra-abdominal washout which precludes the need for microscopy, culture, and sensitivity (11). Another study had five cases where bacteria were resistant to the antibiotics given pre-operatively. However, this did not affect the incidence of post-operative complications (12).
The other patient who had pus samples resistant to the prescribed antibiotic developed a collection post-operatively. However, the patient was treated with Tazocin, an antibiotic that was not listed on the sensitivities obtained from the pus samples. The results of this study suggests that obtaining routine pus samples in complicated appendicitis for cultures and sensitivity can be abandoned which is similar to findings in previous literature (4, 5, 11–15).
However, some studies suggest that there are other benefits in obtaining pus samples which include allowing epidemiologic tracking in hospital and identifying less common organisms that may cause serious disease such as Clostridium (13). Also, with increasing antibiotic resistance, routine culture testing may be useful in identifying changes in susceptibility of organisms to antibiotics and help us select an appropriate antibiotic (16). One study in 2010 reported that 25% of children with gangrenous or ruptured appendicitis were insensitive to the antimicrobial regime used at that hospital during that time, and with on-going concerns regarding antibiotic resistance worldwide this is only likely to increase (17).
Furthermore, there is a medicolegal implication with obtaining peritoneal swabs. There is no other way of identifying the causative organism in the pre-operative phase and therefore, antibiotic prescribing is essentially empirical. If a patient failed to improve on empirical therapy, there would be no direct evidence to guide the change of antibiotic therapy if pus samples were not obtained intra-operatively. Obtaining peritoneal swabs would indicate that all possible effort to define causative organism has been made. This is particularly important in high-risk patients such as those with multiple co-morbidities and frailty as they may deteriorate rapidly without guided antibiotic treatment.
The limitations of this study include a low number of pus samples sent in complicated appendicitis, with surgeons also reporting difficulty in gaining a sufficient sample in some cases. Also, as the data were collected from a single district general hospital, the data may not be representative of the entire UK population. It also suffers from bias due to differences in surgeon skill or experience, and variations in quality of medical notes (18).
Of note, the incidence of complicated appendicitis in our study was higher than in the literature (19), but this is likely due to the broad definition used in our sample—any evidence of free pus of appendix origin, and inclusion of gangrenous appendix without gross perforation. We also excluded patients that pre-operatively were thought to have appendicitis, but had normal findings on laparoscopy.
Conclusion
Routine use of microbiology cultures from pus samples in the treatment of complicated appendicitis confers little or no benefit in terms of clinical outcome. Nevertheless, there may be some value when identifying uncommon organisms which can cause significant disease, and epidemiological trends, especially with the rising concerns of increasing antimicrobial resistance worldwide.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.