
Abstract
Background:
Skeletal dysplasias have been associated with upper cervical instability. Many patients are initially asymptomatic, but the instability may progress to subluxation and dislocation and complications thereof, including death. Surgery is hampered by petite osseous structures and low bone formation rate.
Aim:
To review the outcomes of surgical fusion of upper cervical instability in children with rare skeletal dysplasias.
Material and Methods:
A retrospective study of eight children with five different rare skeletal dysplasias needing upper cervical instrumented stabilization. Cases were evaluated for clinical, radiologic, and quality-of-life outcomes, with median follow-up time of 5 years.
Results:
Six patients underwent posterior, segmental cervical spine instrumentation and fusion (three C1/C2 fusions, three occipitocervical fusions), one anterior cervical instrumented spinal fusion, and one anteroposterior fusion. Autogenous bone grafting was used in all patients, and seven were immobilized using a halo body jacket. Nonunion in occipitocervical fusions was common in these patients (3/8 patients). Rib autograft from occiput to cervical spine with recombinant human BMP-2 was used to salvage nonunions.
Conclusions:
Surgical fixation in the pediatric cervical spine is hampered by fragile posterior structures. A postoperative immobilization by halo vest for 4 months is customary. Selective anterior corpectomy and plate fixation is not recommended in pediatric patients with skeletal dysplasias.
Level of Evidence:
Level 4, Case Series
Keywords
Introduction
Skeletal dysplasias are a clinically and genetically heterogeneous group of disorders characterized by disturbances in the formation and/or growth of bone (1–3). Skeletal dysplasias such as spondyloepiphyseal dysplasia (SED), spondyloepimetaphyseal dysplasia, pseudoachondroplasia, Kniest syndrome, and chondrodysplasia punctata have been associated with a high incidence of cervical instability (1, 2, 4–7). Although many patients are initially asymptomatic, the instability of the upper cervical spine may progress to subluxation and dislocation and subsequently lead to cervical myelopathy, quadriparesis, and possible death (3, 8, 9).
There are only a few adequate follow-up studies on cervical spine fusions in patients with skeletal dysplasias (3, 6, 10). Surgical treatment is complicated by petite and fragile bony spinal elements with low bone formation rate. In addition, most studies include both child and adult patients with upper and lower cervical spine fusions as well as noninstrumented and instrumented spinal fusions. None of these studies have reported quality-of-life outcomes. Outcome evaluation is complicated since not only spine disorders but also other orthopedic problems, such as small stature and early joint degeneration, may affect outcomes.
We critically evaluated clinical, radiographic, and health-related quality-of-life outcomes of upper cervical spine fusions in children with skeletal dysplasias. Here, we describe the surgical treatment of progressive upper cervical instability in eight patients with skeletal dysplasia using modern instrumentation.
Material, Methods and Results
Patients
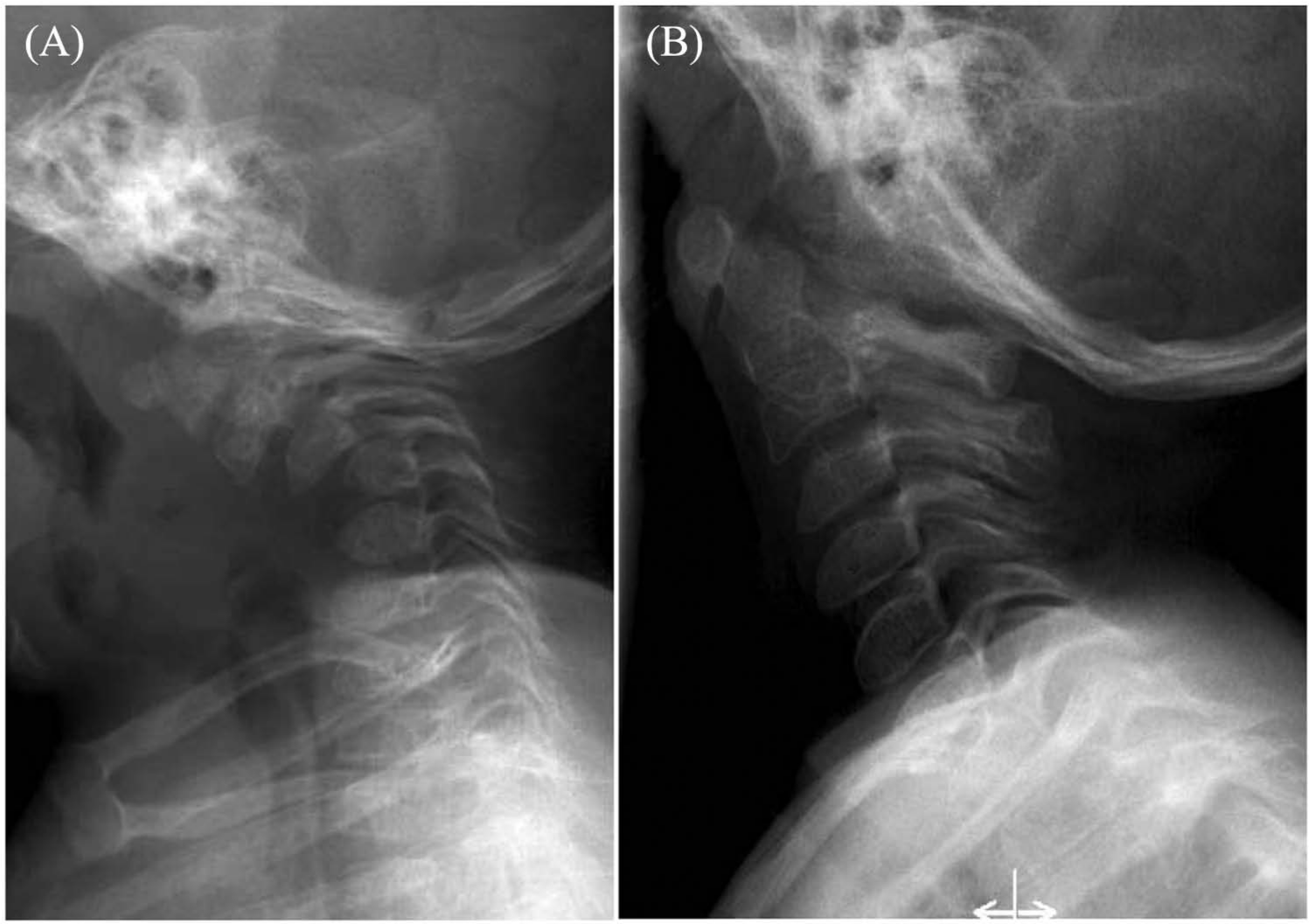
Eight children with upper cervical instability due to skeletal dysplasia underwent cervical spine stabilization with or without decompression in our hospitals (Table 1). Three had SED with marked C1/C2 or C0/C2 instability, one had osteogenesis imperfecta (OI) with severe basilar invagination, one had chondrodysplasia punctata with mid-cervical (C3–C5) instability and tetraparesis since birth, one patient had diastrophic dysplasia with upper cervical kyphosis associated with medullary compression, one had metaepiphyseal chondrodysplasia with C1/C2 instability and asymptomatic spinal cord compression, and one had C1/C2 instability with asymptomatic spinal cord compression due to metatropic dysplasia. The disability caused by the cervical spine disorder was evaluated by the Scoliosis Research Society 24 (SRS 24) questionnaire (11). The SRS scores are presented in Table 1.
Patients and methodological details.
SED: spondyloepiphyseal dysplasia; CD: campomelic dysplasia; MD: metatropic dysplasia; DD: diastrophic dysplasia; OI: osteogenesis imperfecta; MRI: magnetic resonance imaging; SAC: space available for the cord; SRS: Scoliosis Research Society.
Surgical Techniques
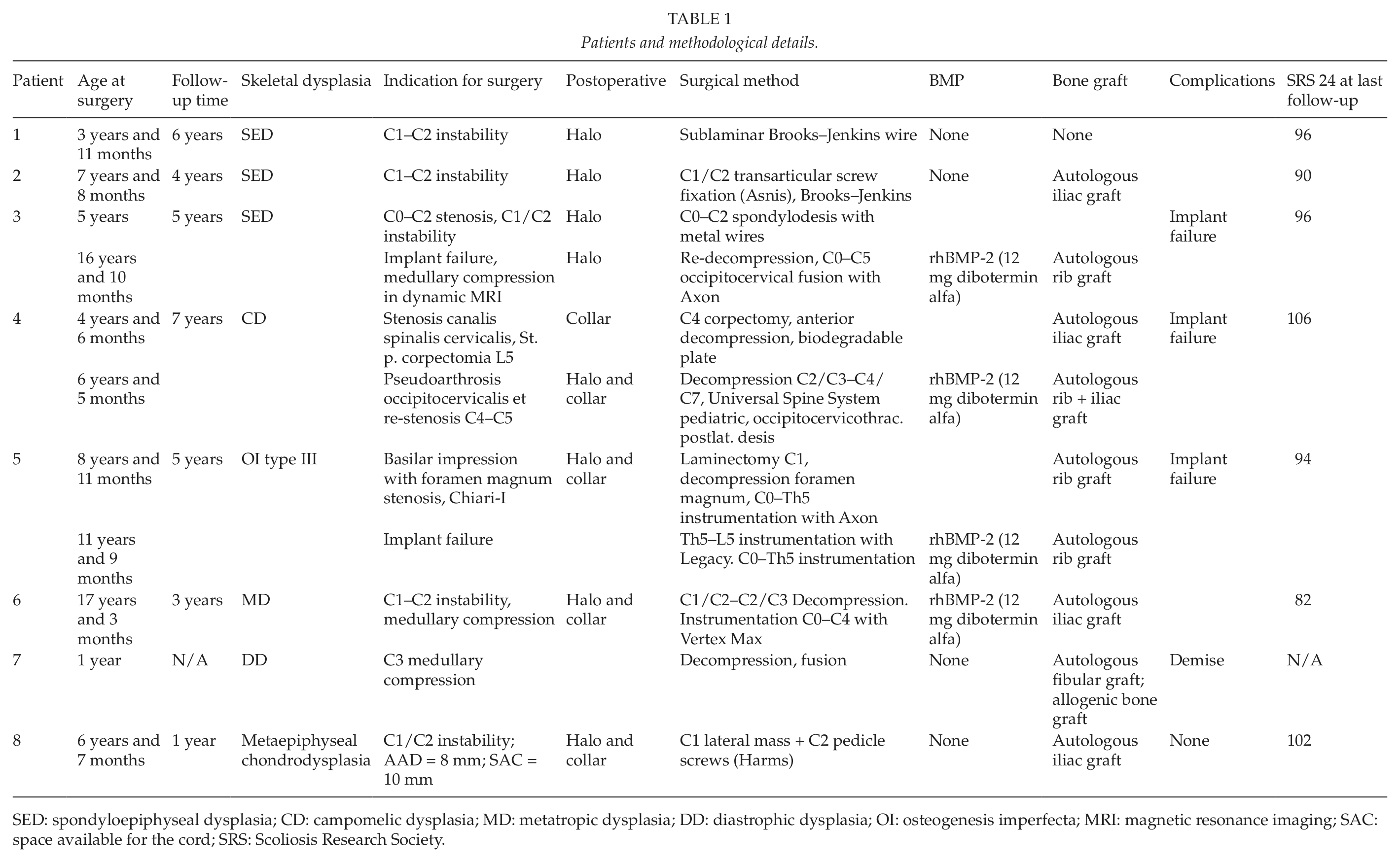
C1/C2 fusions were performed for two girls with SED aged 4 and 7 years, respectively. C1/C2 transarticular screw fixation was preferred preoperatively for both. The first patient had atlantoaxial instability (8 mm) and a hypoplastic dens on flexion–extension magnetic resonance (MR) images. In the first patient, left-sided vertebral artery tapping occurred and sublaminar wire fixation according to Brooks and Jenkins (12) was performed. Computed tomography (CT) angiography performed immediately after surgery showed no vertebral artery lesion. Patient 2 at the age of 3 years presented with a hypoplastic C2 vertebra and a 5-mm instability during flexion–extension radiographs. She was followed up at 2-year intervals. At 7 years of age, the instability was found to increase, with compression of the spinal medulla during cervical flexion on dynamic cervical magnetic resonance imaging (MRI). She underwent one-sided C1/C2 transarticular fixation due to a high-riding vertebral artery on the other side. Fixation was strengthened using Brooks–Jenkins-type sublaminar wires and autologous bone iliac graft (Fig. 1). Both patients were immobilized using halo body jacket for 4 months, and solid spinal fusion could be verified radiologically during follow-up.
A 7-year-old girl with spondyloepiphyseal dysplasia: A) On flexion–extension MR image C1/C2 instability. B) Two-year follow-up radiograph after C1/C2 fusion using one-sided transarticular screw (high-riding vertebral artery on other side and Brooks–Jenkins-type sublaminar wires fixation with solid posterior spinal fusion).
Patient 3 presents with SED. For C1/C2 instability, he underwent a C1 laminectomy and a C0–C2 spondylodesis using metal wires at the age of 5 years. At the age of 15 years, he presented with fatigue in the lower extremities and left upper arm. Implant failure with upper cervical instability was suspected, and in flexion–extension dynamic MRI, the upper cervical spinal cord was compressed during flexion. In somatosensory evoked potential (SSEP), the cortical response was found delayed and slowed. He underwent C0–C2 re-decompression and instrumented occipitocervical fixation. A single structural rib autograft with recombinant human BMP-2 (rhBMP-2) (InductOs; Pfizer Inc, New York, NY, USA (off-label use)) was used. Postoperatively, he wore a halo body jacket for 3 months followed by a cervical brace for 1 year. On follow-ups, he has remained symptom-free regarding his cervical spine.
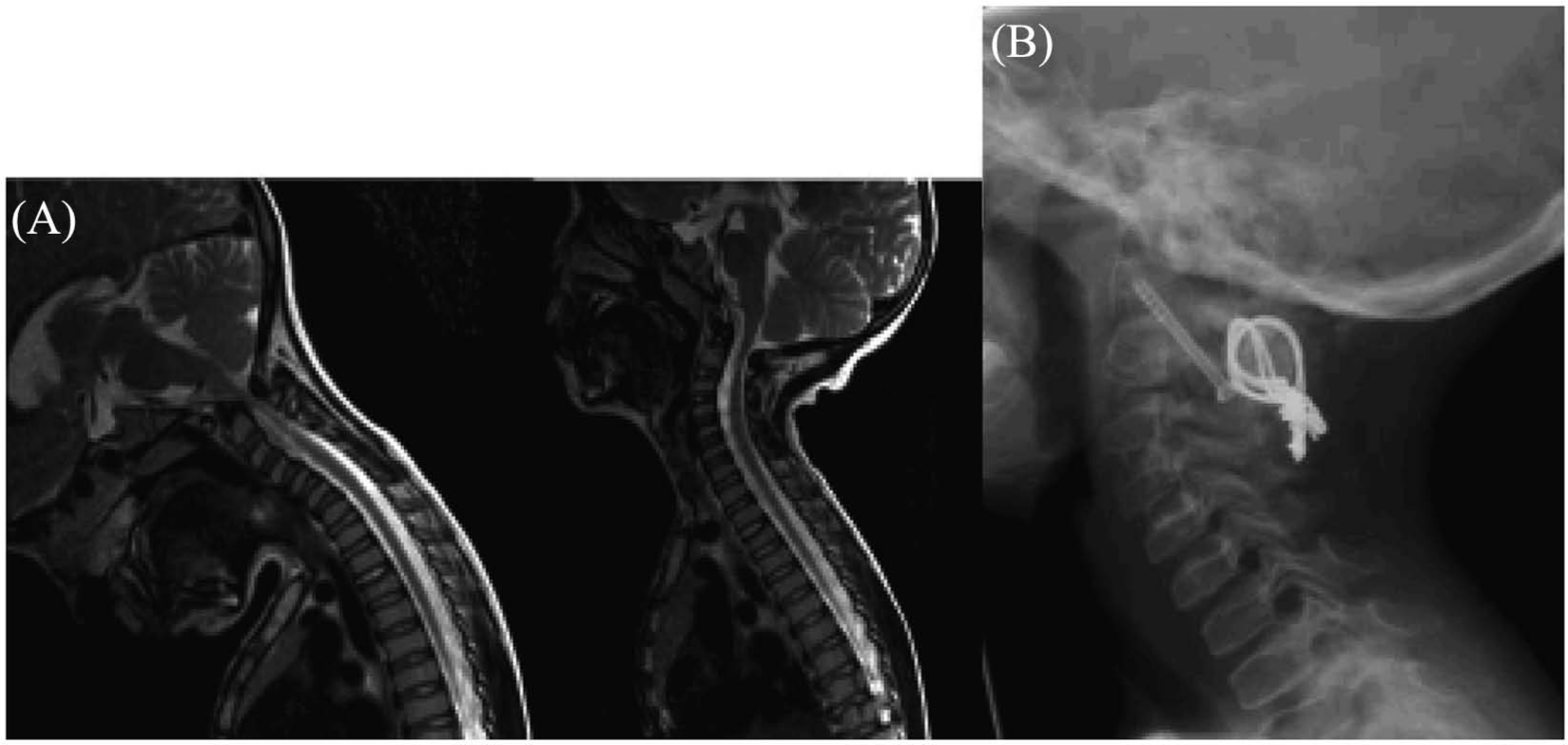
Patient 4 has chondrodysplasia punctata with mild tetraparesis since birth. MR images showed mid-cervical instability with significant high-intensity medullar lesions on T2-weighted images. At the age of 5 years, C4 corpectomy for anterior spinal cord decompression was performed, and spinal fusion was attempted using autologous structural iliac graft with anterior biodegradable plate fixation for reconstruction at another hospital. Immediately postoperatively, the fixation failed and he became tetraplegic (Fig. 2). He was transferred to our unit, where, on the first postoperative day, he underwent posterior decompression C2/3–C6/7 with occipito-cervico-thoracic fusion (C0–Th5) using CerviFix with Universal Spine System (USS) pediatric (Synthes GmbH, Zuchwil, Switzerland) and posterolateral autologous bone grafting. Due to severe respiratory distress, he was not placed into a halo body jacket but was instead immobilized using a custom-made hard collar. His postoperative rehabilitation was uneventful, and his locomotive skills improved accordingly. At 12 months postoperatively, he was able to walk assisted and lift his arms head-height. At 22 months postoperatively, however, the instrumentation had failed at the cervicothoracic region and during cervical flexion, and cervical spinal cord compression was verified by MRI.
A 5-year-old boy with chondrodysplasia punctata: A) First MR image immediately after index surgery: fixation has failed and space available for cord was only 3 mm. B) MR image after first revision surgery showing wide posterior decompression. C) MR image showing moderate pinching of the cord when occipitocervical fusion did not fuse. D) CT after second anteroposterior revision. E) Radiograph 2 years after last revision surgery showing solid posterior spinal fusion.
A reoperation was performed, where the occipitocervical spine was fused using a single autologous rib graft with rhBMP-2, and re-cervicotomy with anterior decompression C3–C6 with reconstruction with autologous bone graft (iliac crest) without plate fixation due to small cervical vertebral bodies was performed (Fig. 2). Postoperatively, he wore a halo body jacket for 3 months, followed by a cervical brace. On follow-ups, he is walking assisted, performs fine motor skills manually, and solid spinal fusion has been verified using radiographs.
Patient 5 is diagnosed with OI type III. Basilar invagination associated with foramen magnum stenosis, Chiari-I malformation, and mild hydrocephalus was detected at the age of 7 years. He did not present any symptoms, neurological exams were normal, and SSEP was normal. However, he felt that his exertional levels were declining. Surgery was elected, and he had a halo traction for 5 days preoperatively. C1 laminectomy was performed, with decompression of the foramen magnum with occipito-cervico-thoracic instrumentation from C0 to Th5 using occiput plates, cervical hooks, lateral mass screws, and thoracic pedicle screws (Axon; Synthes) with slight lifting of occiput from cervical spine. A posterolateral spondylodesis with allogenic bone grafting was performed. Postoperatively, he wore a halo vest for 3 months, followed by a cervical brace. He fell from his wheelchair 2 days after halo body jacket removal, and one of the stabilizing cervical rods broke. During follow-up, he developed a 50° thoracolumbar kyphoscoliosis needing posterior instrumented total pedicle screw fixation from upper thoracic spine (continuing previous instrumentation with dominos) to L5 (CD Legacy 5.5; Medtronic, Memphis, TN, USA). Two and half years postoperatively, the other cervical rod failed and basilar invagination presented. Halo traction was immediately instituted. A posterior revision using instrumentation from occiput to upper thoracic spine taking advantage of previous fixation points was performed using a single rib strut autograft between occiput and upper cervical spine; rhBMP-2 (InductOs) was applied. Postoperatively, he was immobilized using halo body jacket and with a custom-made collar thereafter. Solid fusion was verified radiologically during follow-up.
Patient 6 is a 16-year-old girl with metatropic dysplasia who had C0/C2 marked instability (C1 assimilation to C0) and cervical spinal cord compression on MRI. The medulla was compressed without signal changes on T2 images. Besides neck pain, she was asymptomatic. Posterior decompression with C1 laminectomy and partial C2 undercutting decompression were performed with C0–C4 instrumented fusion (Vertex Max; Medtronic) using occiput plates and cervical laminar hooks. Autogenous bone grafting from posterior iliac wings and a single dose of rhBMP-2 (InductOs) for spinal fusion were applied. Postoperatively, she used a halo body jacket for 4 months followed by a custom-made hard collar.
Patient 7 had diastrophic dysplasia and tetraparesis including respiratory problems since birth. She had a 76° cervical kyphosis on MR images with severe cord compression at C3 level at the age of 3 months. Circumferential cord decompression with anteroposterior cervical spine fusion from occiput to lower cervical spine was attempted at 12 months. Autologous fibular strut graft was used anteriorly and allogenic bone graft posterolaterally. Her symptoms did not improve, and she died soon after surgery due to respiratory complications.
Patient 8 presented with C1/C2 instability due to metaepiphyseal chondrodysplasia. Stabilization was performed with C1 lateral mass screws and C2 pedicle screws, augmented with autologous iliac crest bone grafts at the age of 6.5 years without peri- or postoperative complications. Postoperative immobilization was with a halo body jacket, followed by a custom-made collar.
Discussion
Seven out of eight patients survived through the immediate postoperative period. One patient died soon after attempted cervical cord decompression and fusion at an early age. One patient (patient 4) developed significant neurologic deterioration after anterior medullar decompression (C4 corpectomy) and biodegradable plate fixation. Three of four occipitocervical fusions, all without strut autografts or rhBMP-2, resulted in nonunion and required revision surgery, one of them 2.5 years postoperatively.
Bony elements in these children are extremely tiny and fragile. Transarticular screws seem to produce the best fixation points, but a high-riding vertebral artery or a diminutive C2 pedicle may prevent their use. Lateral mass screws can sometimes be used, while in most cases, laminar hooks provide the easiest and safest way for cervical anchor points. Occiput and upper thoracic spine provide the most reliable fixation points. A single rib structural autograft fixed using sublaminar wires between occiput plates and cervical laminae with a single dose of rhBMP-2 resulted in fusion in all revision cases. Use of the halo body jacket did not increase the risk of significant postoperative complications.
Flexion–extension MR images provide detailed evaluation of cervical instability and spinal cord compression, and we recommend investigations to be done before the age of 8 years for all patients with skeletal dysplasias, known to be associated with cervical spine instability. CT imaging can be used not only for operative planning, such as cervical pedicles, location of vertebral artery channels, and posterior laminar elements, but also for postoperative evaluation of fixation and spinal fusion.
In patients with craniovertebral anomalies, neurological findings usually present in the third and fourth decades (13). In a study on congenital osseous anomalies of the cervical spine, 31% of pediatric patients presented with neurological symptoms, and the incidence of myelopathy was estimated to increase on follow-up (9). The authors recommend periodic follow-up for all patients, with dynamic lateral radiographs to identify segmental instability. In our series, we chose to follow-up the patients regularly and opted for surgery when instability was evident or when progressive neurological findings necessitated intervention.
In the largest series published thus far, Ain et al. (3) reported outcomes of 25 patients (aged 1.75–46.9 years) with skeletal dysplasias undergoing cervical spine fusion. Of them, 21 (84%) achieved solid bony union. This is strikingly different from our study, with only three patients out of seven developing solid bony union. Our patient population included rare skeletal dysplasias with one previous case report available for cervical spine fusion on a patient with chondrodysplasia punctate (5) and one report with six cases (6) (three SED, one Morquio’s syndrome, one pseudoachondroplasia, and one chondrodystrophia calcificans congenita) and no previous reports for cervical spine fusion in patients with diastrophic dysplasia. However, both our C1/C2 instrumented fusions in SED patients were successful. Bisphosphonate treatment may interfere with fusion of femoral osteotomy healing (14). Our OI and metatropic dysplasia patients received bisphosphonates before surgery, but did not receive them for a 1-year period after surgery.
Occipitocervical spinal fusion in combination with neural element decompression appears problematic. The occiput usually contains no cancellous bone in these patients. After halo removal, forces acting between occiput and cervical spine are large. Therefore, our current practice in these instances is to invariably use rhBMP-2 (15) and single rib structural autograft whenever possible. The use of rhBMP-2 has recently been discussed in the literature and is of concern, as associated adverse reactions are encountered in 10%–50% of cases in spinal surgery (16). Rib harvesting did not produce any sequelae, but use of rhBMP-2 produced mild to moderate posterior neck swelling during the immediate postoperative period. Therefore, all three patients who received rhBMP-2 remained intubated for the first 24 h to follow neck swelling. By this approach, we were able to obtain fusion in all patients in this series, except for the one who died soon after surgery. The use of rhBMP-2 should, however, be evaluated individually for each patient.
Atlantoaxial instability is known to associate with SED. Nakamura et al. (17) evaluated 16 SED patients (aged 3–37 years). Six (38%) of them showed atlantoaxial instability and five of them presented changes suggestive of myelopathy. Risk factors for cord compression included short stature (−7 standard deviation (SD)) and severe coxa vara. Ain et al. (3) reported seven SED patients with upper cervical spine fusion. Spinal fusion occurred in five patients during follow-up, one patient required revision surgery due to nonunion, and one patient presented implant loosening. Three had C1/C2 fusion with two undergoing solid spinal fusion. Svensson and Aaro (6) reported solid fusion in three patients with SED during follow-up (3/3 patients).
Chondrodysplasia punctata has been associated with three types of spinal deformities, of which a C2 dentocentral disruption affects the cervical spine (18). Spinal instability and a case report with cervical spine stenosis in chondrodysplasia punctata have been previously reported (19). He underwent vertebrectomies of C4 and C7 with a fibular strut graft. We report a similar case with anterior spinal cord decompression and anterior plate fixation resulting in immediate failure and severe neurological deterioration. Combining Violas et al.’s (19) and our findings, we suggest a combined anteroposterior approach for full spinal cord decompression with long posterior occipitocervical fixation, when necessary continued to the upper thoracic spine.
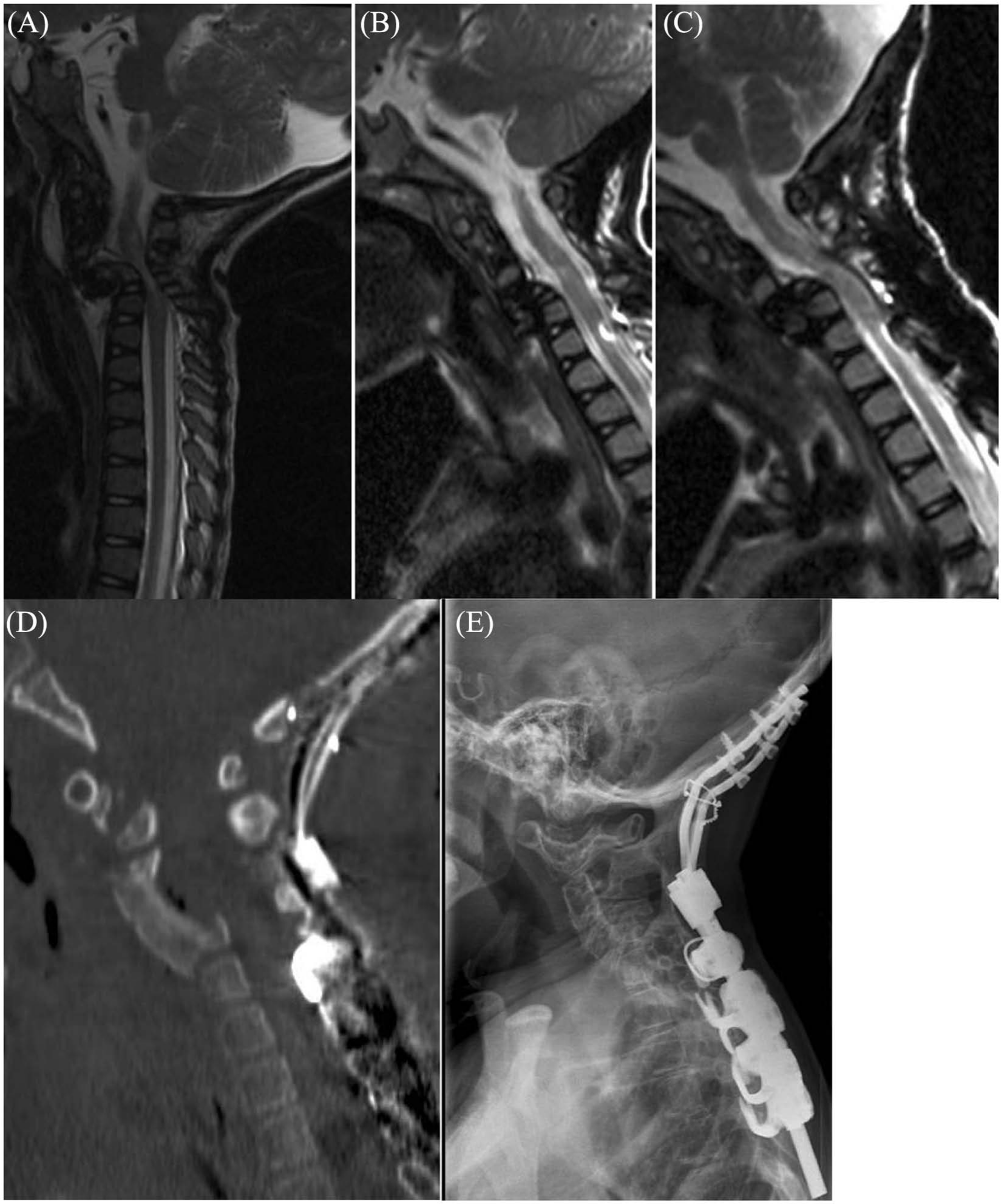
Most patients with diastrophic dysplasia show resolving mid-cervical kyphosis before the age of 18 months (Fig. 3) (20). Cervical kyphosis in patients with diastrophic dysplasia is associated with increased mortality, and thus, living adult diastrophic dysplasia patients with severe cervical kyphosis are rare. In our patient, severe neurologic compromise resulted in death despite active surgical treatment.
Resolving mid-cervical kyphosis on a patient with diastrophic dysplasia: A) First plain radiograph at the age of 1 year. B) At the age of 4 years, kyphosis is fully resolved.
In total, 8%–25% of patients with OI develop basilar impression (21). Ibrahim and Crockard (22) reported long-term outcomes of 20 patients (one 12-year-old child) treated using ventral decompression and staged occipitocervical instrumented fusion. At the end of follow-up, 25% of the patients had recurrence of brainstem symptoms or had died, and 15% showed no neurologic improvement. In our 8-year-old boy, the indication for surgery was a progressive basilar invagination, causing clinically neck and head pain and disturbance of cerebrospinal fluid circulation. To our knowledge, he is the youngest OI patient operated for this condition. He had preoperative halo traction making anterior odontoid resection unnecessary. After a 3-year follow-up, he has not needed a ventriculoperitoneal shunt and is free from head and neck pain.
Leet et al. (23) evaluated cervical spine in 13 patients with metatropic dysplasia. Nine had spinal stenosis (space available for the cord (SAC) < 11 mm). Two children had myelopathy. Atlantoaxial instability (Atlanto-dens interval (ADI) > 5 mm) was additionally noted in 5 patients. Nine patients underwent posterior upper cervical fusion and decompression of the spinal cord. Three patients developed nonunion and four patients developed other complications. In our patient, atlantoaxial instability resulted in fixed anterior position of C1 on C2 and spinal cord compression without neurological compromise. Instrumented occiput–C2 fixation with wide neural element decompression resulted in bony fusion.
Conclusions
Surgical fixation in the pediatric cervical spine is hampered by fragile posterior structures, and true cervical spine fixation is at times established only via the occiput and the laminae of the cervical vertebrae with laminar hooks and upper thoracic pedicle screws. At times, C1/C2 transarticular screw fixation may be successful, necessitating a thicker isthmus of the C2 vertebrae. A postoperative immobilization by halo vest for 4 months is customary. Selective anterior corpectomy and plate fixation is not recommended in patients with skeletal dysplasias. Upper cervical instability in a patient with skeletal dysplasia must be evaluated and treated on an individual basis.
Footnotes
Declaration of Conflicting Interests
None declared.
Funding
This study was supported by Medtronic International, Synthes, Baxter Finland, Finnish Pediatric Research Foundation, and Turku University Central Hospital.