
Abstract
Background and Aims:
Treatment of scapular neck fractures remains controversial. Advantages of surgical treatments, such as anatomical restoration of fracture displacement, are counterbalanced by approach morbidity. We conducted a meta-analysis of 463 scapular neck fractures and compared clinical, functional, and radiographical outcomes in operatively and nonoperatively treated scapular neck fractures.
Material and Methods:
A literature search was conducted, including the databases PubMed/MEDLINE, Embase, and the Cochrane Database of Systematic Reviews. Manuscripts were included if they reported a precise description of treatment, complications, functional outcomes, and/or radiographic evaluation. Data about day-to-day activities, level of pain-freeness, range of motion, functional grading, and radiographical assessment were pooled and compared using fixed effects models.
Results and Conclusions:
A total of 22 manuscripts were relevant, including 1 prospective cohort study and 21 retrospective studies. The studies showed a high heterogeneity in the result assessment. Most patients had concomitant injuries. In total, 234 out of the 463 fractures were treated operatively. Pain-freeness and radiographic outcome measurements were significantly better in the operatively treated group, whereas range of motion was significantly improved in the nonoperative treated patients. Complication rate for surgical treatment was about 10%. From the achievable data, there was no bias detected when comparing the two treatment groups. However, those data could not be analyzed for all included studies. For the same reason, the role of additional surgical treatment for concomitant injuries to the shoulder girdle could not be cleared completely. Caution should be exercised, and individual injury patterns have to be taken into consideration when considering the best treatment options.
Keywords
Introduction
Most scapula fractures result from severe blunt forces to the body. They account for 3%–5% of all fractures of the shoulder girdle (1). Polytraumatized patients (5%–10%) present fractures in this region (2). Through the underlying high-energy trauma, these patients usually have concomitant injuries with higher treatment priority. As a consequence, management of scapular fractures is often delayed. Even late or missed diagnosis is frequent and increases the number of conservatively treated patients (3).
Because of good blood supply and a high tolerance for malalignment, the fractures of the scapula body are mainly treated conservatively. Operative treatment is the gold standard for glenoid fractures, based on their articular involvement. Open reduction with internal fixation or arthroscopically based techniques is described.
Scapula neck fractures are extra-articular. However, muscular deforming forces and the effect of gravity on the upper limb pull the lateral fragment anteromedial and distally. This results in a displacement and malrotation of the glenoid fossa in total, affecting the glenohumeral joint function. Operative treatment promises a sufficient restoration of the glenopolar angle (GPA), with the disadvantage of approach morbidity and operative risks.
When reviewing clinical studies regarding the treatment of scapula neck fractures, we are dealing with a complex patient cohort, heterogeneity of different scoring systems and assessment tests, and various follow-up time points. Zlowodski et al. (4) compared operative with nonoperative treatment in a systematic review of scapula fractures, whereas Lantry et al. (5) focused on the operative treatment using the same method. Our study, however, to the best of our knowledge, is the first one dealing specifically with the scapular neck region. We retrieved the available literature of the last 25 years regarding scapula neck fractures and performed a meta-analysis. The purpose of this study was to compare clinical, functional, and radiographic outcomes of operative and nonoperative treatment of scapular neck fractures.
Material and Methods
Starting with a search of electronic databases, the different phases of a meta-analysis were conducted according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement. Inclusion criteria were all articles, in English or German language, from 1984 onward, which presented data concerning treatment of scapula neck fractures. The following databases were searched: PubMed/MEDLINE (from 1984 to January 2012), Cochrane Database of Systematic Reviews (January 2012), and Embase (from 1984 to January 2012) to identify all studies describing the treatment to scapula neck fractures. The PubMed/MEDLINE search strategy was “fracture” AND (“scapula” OR “scapular neck”) OR “floating shoulder” OR “disruption” AND (“superior shoulder suspensory complex” OR “SSSC”). The search was independently performed by two reviewers (T.D. and K.H.). The references of retrieved publications were also manually checked to add studies fulfilling the inclusion criteria, missed by the electronic search. Unpublished data, abstracts from scientific meetings, or review articles were excluded. The full manuscript was retrieved when title, keywords, or information from the abstract revealed information potentially meeting the inclusion criteria. Manuscripts outside English or German language were considered if translation was possible. After preliminary screening of the included databases, we found a lack of original randomized controlled or controlled clinical trials. Therefore, all study types found, with more than five presented cases, were considered if they fulfilled inclusion criteria. All identified studies were independently assessed according to the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines by two reviewers (T.D. and A.B.). From the included studies, data for meta-analysis were extracted by one author (T.D.) using a prepiloted data sheet. Extraction was verified by a second author (K.H.). Disagreements were resolved in a consensus meeting and with third-party adjudication (A.B.) (Fig. 1).
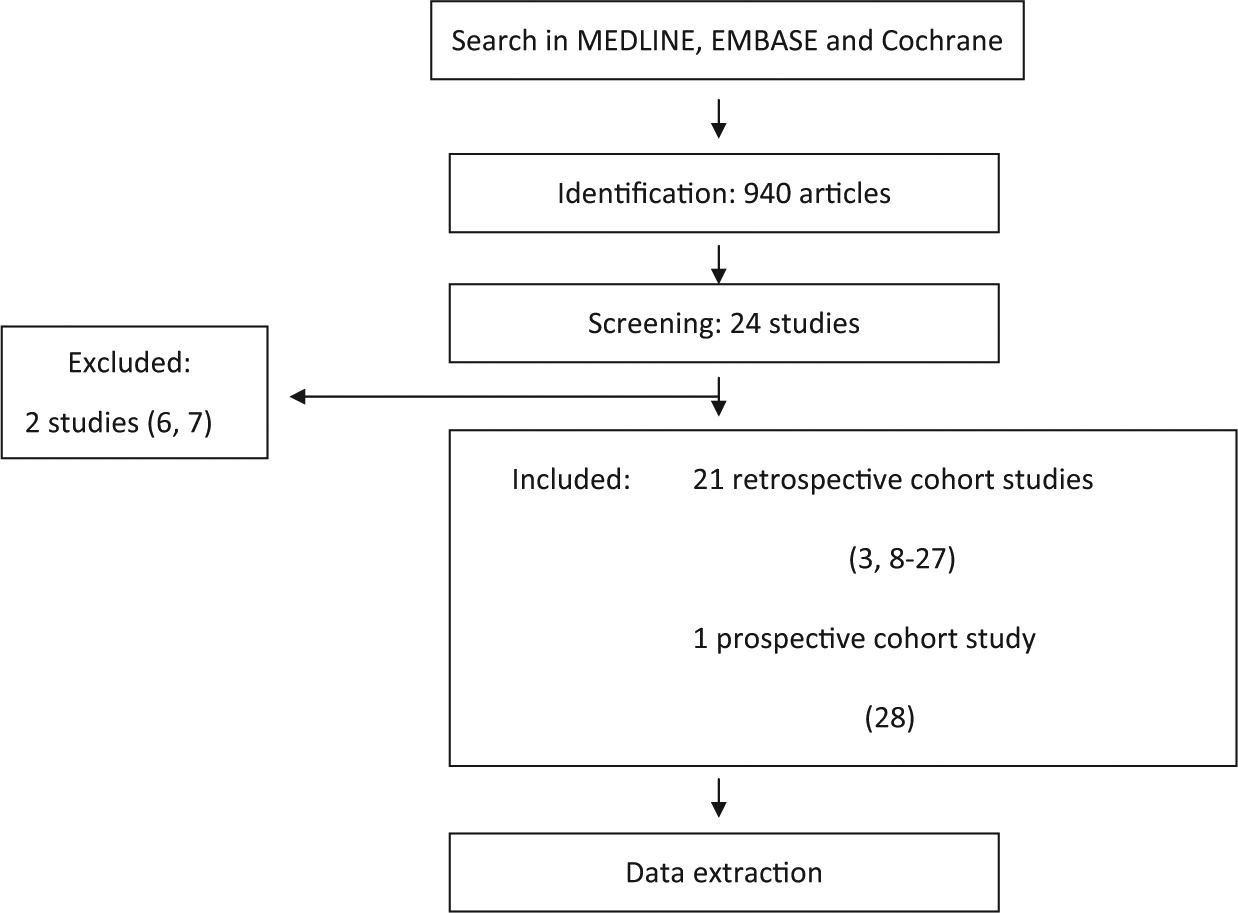
Search strategy according to the PRISMA guidelines.
Included were all patients, regardless of age or gender, with a scapular neck fracture except those with periprosthetic fractures, documented congenital deformities or metabolic syndromes. Bilateral fractures were included and counted as two fractures. No restrictions were made regarding the time point of surgical treatment. Anatomical location of the fracture, treatment modalities, functional, and radiographic results at follow-up were assessed. Additionally, demographic data, time of follow-up, concomitant injuries, and complications were noted.
Fractures through the anatomical neck and through the surgical neck were classified as scapular neck fractures (14). The term “floating shoulder” was initially defined as scapular neck fracture combined with an ipsilateral distal clavicular fracture (29). Later, the definition of the superior shoulder suspensory complex (SSSC) was established and a disruption in two regions of this complex was classified as floating shoulder (30). As we were focusing on the scapular neck region, we included both injury definitions, as long as the scapula neck was involved.
Data were sought for the following outcome measures:
Restrictions in day-to-day activities.
Pain in day-to-day activities.
Range of motion compared with the unharmed side.
Grading of function.
Radiographically assessed GPA at follow-up.
Radiographically assessed translational displacement at follow-up.
A free range of motion or an identical range of motion compared with the unharmed side was assumed when this was stated clearly by the authors, or the noticed degrees for different ranges of motion were those of normal population values.
The grading of function was assessed using the Constant score. When other validated scores were used (Rowe, Herscovici), the patients were grouped either in the category excellent/good or in the category fair/bad.
A normal GPA ranges between 30° and 45° and is defined as the angle between a line connecting the most cranial with the most caudal point of the glenoid cavity and the line connecting the most cranial point of the glenoid cavity with the most caudal point of the scapular body. According to Romero et al. (23), a GPA < 20° was defined as a severe glenoid rotational malalignment. A translational displacement of over 1 cm was defined as severe (26).
Fractures were grouped into an operative treatment group when the scapular neck fracture was treated operatively or in a nonoperative treatment group when the scapular neck was treated conservatively regardless of possible other surgeries in the ipsilateral shoulder girdle.
The results of comparable studies were pooled using fixed effects models when appropriate. The odds ratio (OR) was calculated and reported with 95% confidence intervals (CIs) for dichotomous outcomes and weighted mean differences and 95% CIs for continuous outcome measurements. Data were pooled using Review Manager 5.0.
Results
Among the 940 citations initially identified by our search, 24 manuscripts were relevant by title and abstract and suitable for evaluation. There were 21 retrospective cohort studies and one prospective cohort study included. According to the time frame of our search strategies, the oldest one was from 1984 and the newest from 2011. Excluded were two studies: one study because the treatment for all patients was not exactly defined (6) and one study clearly stating that only scapula body fractures were included (7).
There were in total 706 patients with fractures in any region of the scapula included in the follow-up, leading to 463 fractures of the scapular neck region. A total of 249 fractures were classified as isolated scapular neck fractures, 207 were accompanied by an ipsilateral clavicula fracture, and seven were neck fractures with accompanying coracoid, acromion, body, spine, or glenoid fractures. The mean patient age was 39 years with 13% of the patients being female. Minimal to maximal follow-up was 9 months to 14 years. In all, 67% of all included patients had concomitant injuries. Thoracic injuries were found in up to 59%. Dominant injury mechanism was motor vehicle or motorcycle accident, followed by fall from great height. Less than 5% of all fractures were open injuries inflicted by gun shots (8).
A comparison of demographic data and pretreatment measurements of the GPA and the initial fracture translational dislocation can be found in Table 1 for those patients with clearly identifiable parameters.
Comparison between patients with surgical and nonoperative treatment regarding gender ratio, age, i-GPA, and initial translational dislocation.
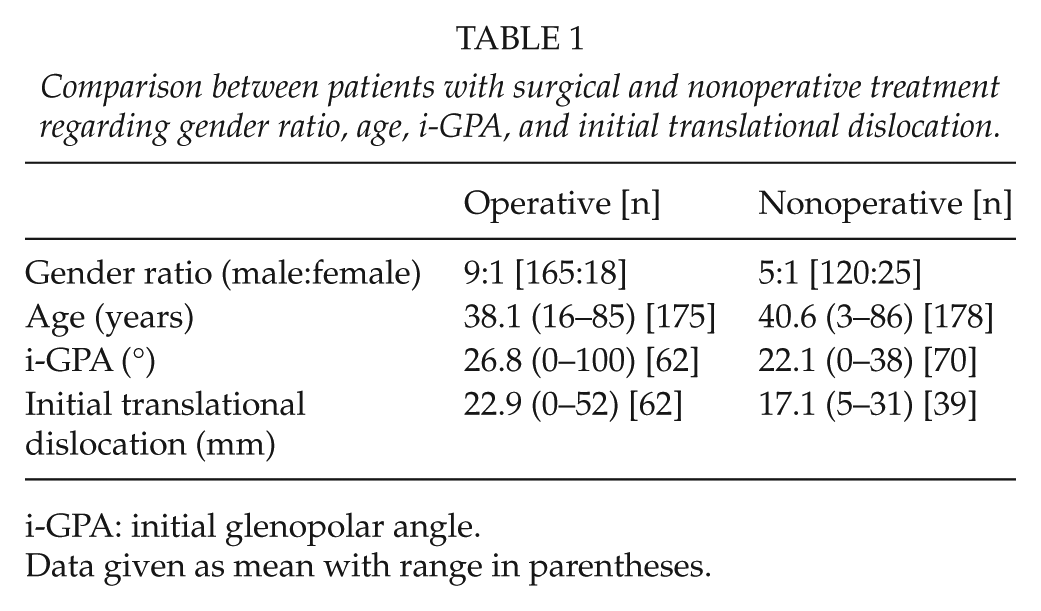
i-GPA: initial glenopolar angle.
Data given as mean with range in parentheses.
A total of 234 scapula neck fractures were treated operatively and 229 were treated nonoperatively. From the operatively treated group, six authors used preoperative computed tomography (CT) (10, 18, 28) and three-dimensional (3D) CT (9, 15, 17) scans to analyze the fracture type. Another six relied on conventional X-rays only (3, 14, 16, 19, 20, 22). One author used magnetic resonance imaging (MRI) for diagnosis of integrity of the brachial plexus (18).
An anterior approach was used for anterior or inferior rim fractures of the glenoid and for fractures of the coracoid processes. Here, the incision went through the deltopectoral sulcus and reached the joint through dividing the subscapularis tendon near its insertion. For neck fractures or complex glenoid fossa fractures, the Judet approach or minor modifications of its origin description were used. Here, a skin incision curved from the acromion over the spine to the inferior angle and a dissection was performed through the interval between the infraspinatus and the teres minor muscle, protecting the suprascapularis nerve and the vessels entering in the superior portion. Only a few patients required a combined anterior/posterior approach because of a mix of fracture patterns.
Operative treatment produced the following complications: nine patients with postoperative stiffness (14, 15), two with intraoperative corrected insufficient reduction (9), one with intraoperative corrected entrapment of the suprascapular nerve (9). Furthermore, there were three postoperative hematomas with the need of revision surgery to evacuate (9, 14), one heterotopic ossification (18), two implant failures (22), four malunions (22), and two superficial wound infections (14). The calculated overall rate for postoperative complications was 10.2%.
From the numbers of treatment available, no statistically relevant differences in the restriction in day-to-day activities (OR = 1.63, favoring operative treatment, p = 0.16) or the constant score (OR = 1.4, favoring nonoperative treatment, p = 0.62) at time point of follow-up could be seen. There were more patients pain-free during day-to-day activities in the groups undergoing surgery (OR = 2.77, p < 0.00001). There was a higher rate of patients with free range of motion compared with the unharmed side (OR = 0.28, p < 0.00001) treated without surgical intervention in the scapula neck region. There were no patients in the surgically treated group with a translational dislocation over 1 cm (OR = 27.28, p = 0.02) or without a normalized (>20°) GPA (OR = 17.64, p = 0.05) at follow-up examination (Fig. 2A to F). From the available data, no comparisons could be made regarding different physiotherapy activities or differences in the time of immobilization between the patients with or without surgery for the scapula neck fractures.
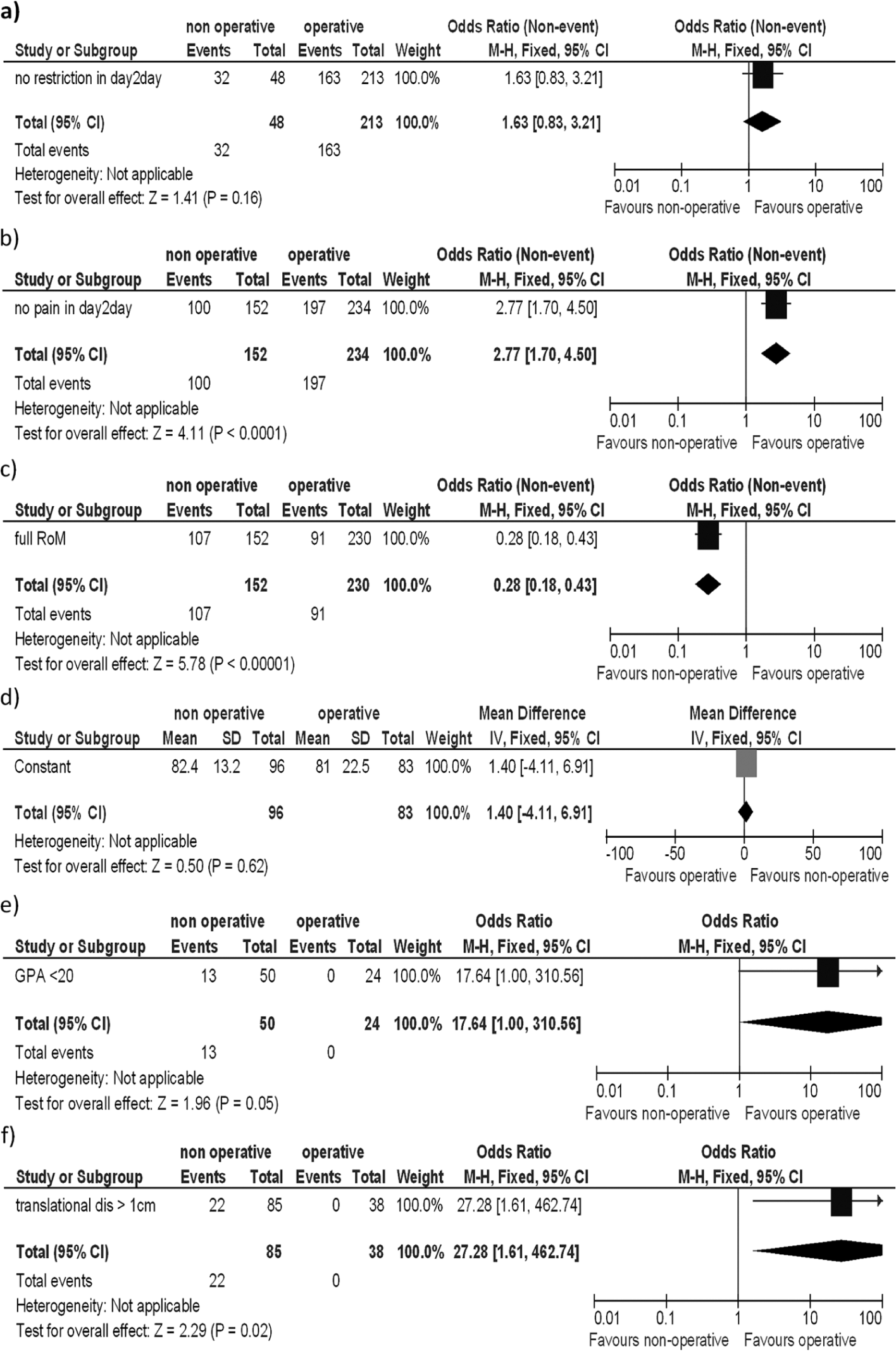
Number of patients with A) No restrictions. B) No pain during day-to-day activities. C) Full range of motion. D) Mean constant score. E) Normalized (<20°) glenopolar angle (<20°). F) Remaining translational dislocation of over 1 cm.
In total, 207 combined fractures of the scapula neck and the clavicula were documented. Out of these, 127 clavicular fractures were treated nonoperatively and 80 were treated by open reduction and internal fixation.
Discussion
Patients with scapular neck fractures have a high percentage of concomitant injuries. Most of these patients were severely injured. Accompanying thoracic injuries in the included patients were common, with up to 59% of patients with multiple rib fractures (15). The effect of concomitant injuries is eagerly discussed. Whereas Schofer et al. (24) deducted no influence, Bozkurt et al. (12) summarized that these were important factors to be considered when evaluating the reasons for different functional outcomes. There was no influence of gender in any study.
The rate of involved scapula neck fractures compared with all scapula fractures was 55% in our meta-analysis. Ada and Miller (6) in 1991 described a portion of 21%–44%. This might be explained through our bias in the literature search. However, as most studies included in this meta-analysis involved multiple fractures of the scapula, there might be also an explanation in a general increase in high-energy trauma mechanism. In addition, nowadays, the use of multislice detector CT scan diagnostic is implemented in most clinics in the initial diagnostic phase of severely injured patients, and therefore, the missing of such fractures might be minimized.
The localization of the scapular neck fracture (anatomic neck: lateral to the base of coracoid process versus surgical neck: medial to the base of coracoid process (14)) showed no influence, although most studies did not distinguish between these locations.
Restricted movement after scapula neck fractures is described (6). Although arbitrary, a GPA under 20° and a translational displacement over 1 cm are graded as severe in multiple studies (23, 26). A correlation was seen between a persisting rotational malalignment (GPA < 20°) and a less favorable long-term outcome (23). There is a high correlation between function and GPA (12). Even after 10–20 years, one-quarter of patients with displaced scapula fractures had residual shoulder disabilities with less favorable results in scapular neck fractures. Nordqvist and Petersson (21) suggested early operative treatment in scapular neck fracture patterns. With the thick muscular envelope and rich vascular supply surrounding the scapula, a rapid formation of callus is seen even in displaced situations. Herrera et al. (15) described the delayed surgical treatment of fractures at least 3 weeks after the time point of injury. To line up, the lateral border reduction maneuvers were necessary, with Schanz pins as joystick, with the use of a lamina spreader or a small external fixator as minidistractor. All fractures could be realigned in this study.
There are contradictory studies, if a severe displacement and rotational malalignment of scapular neck fragment can occur even without a double disruption of the SSSC. Romero (23) reports three of those cases, whereas van Noort (26) could not detect a significant glenoid displacement in 13 patients without a double disruption of the SSSC.
The amount of tolerable displacement leading to an indication for surgical treatment is controversial in literature. Labler (19) indicated a scapular neck displacement of more than 25 mm (Herrera et al. (15) indicated a displacement of more than 15 mm) or a GPA under 30° as a trigger for surgical treatment. Many authors declare that it is of paramount importance to restore an accurate articular reduction and a restoration of alignment and rotation of the lateral margo of the scapula to gain a sufficient orientation of the glenohumeral joint (15). Bauer et al. (10) recommended early operative treatment in displaced fractures of the anatomical and unstable fractures of the surgical neck, based on the findings of 20 patients and a mean follow-up of 6 years. Other authors proclaim that conservative treatment is appropriated at least for patients without associated ipsilateral shoulder injuries. Questioning the indication of 1-cm translational displacement, good functional outcome (expressed in a constant score of 90) was achieved despite significant translational displacement (26). Leung and Lam (20) found significant pain and abduction dysfunction in conservatively treated scapular neck fractures; this was not seen in other studies (12). Bozkurt et al. (12) concluded that the decreased GPA and the degree of instability are the best predictors for functional outcome.
Good or excellent scoring results (constant score) were achieved in conservative treatment with absolute scores from 78 (12) up to 96 (13). However, the highest score in this category reported by Edwards et al. (13) could not be reached even in the control groups (contralateral uninjured upper limb) of other studies (24).
A significant better outcome regarding pain-freeness was achieved in the patients undergoing surgery and in patients with restoration of a normal GPA and minimized displacement. However, caution should be exercised as this finding might not be directly correlated and multiple factors add up to the results.
Authors of the underlying publications were very vague with the time point of surgery. Only five studies included a specific time frame from injury to surgery. All mean time periods were between 4 and 12 days with a range from the day of injury up to 54 days. The study by Herrera et al. (15) was an exception; Herrera et al. classified their time of treatment as “delayed” with a mean of 30 days (range from 21 to 57 days). All other authors did not specify the time range between injury and surgery, stating mostly that they waited for soft tissue normalization.
There was one study with level of evidence 3 (28). In this study, each treatment group (surgery versus nonoperative treatment) included 31 patients. The authors reported a similar outcome regarding healing, pain-freeness, and complications with the bias of having more displaced fractures in the surgical treatment group. They did not recommend surgery in mildly displaced fractures (less than 2 cm).
No sufficient comparison could be made regarding the need of or the time frame of immobilization. Nearly all authors express the need for physiotherapy; however, no recommendation could be drawn from the present studies when to start or which early limitations in the range of motion might be suitable. There was no faster start in physiotherapy in the operative treated group. Herrera et al. (15) described the start of physiotherapy at 2 weeks and reaching the state of removal from all restrictions at 3 months after surgery. Some authors were more progressive starting physiotherapy at day 5 (14), while others reported removal of movement limitations when pain relief was reached (28).
Normal X-ray seems to be sufficient, as only half of the studies relied on CT scans. This might be based on the fact that numerous studies were started at a time when CT scans were not standard in primary trauma care. However, modern 3D reconstructions of complex scapula fractures might help to better understand the underlying pathomorphology and guide treating surgeons. This tool seems mandatory when the glenoid was involved (Fig. 3) (12, 15). Besides authors favoring a 3D scan preoperatively (31), others deny a positive effect of CT diagnostic in the understanding of scapula neck morphology (32). All therapeutically important diagnostic measurements such as the GPA or translational displacement were based on conventional radiographs. A true anteroposterior view perpendicular to the plane of the scapula, a lateral view, and if possible, an axillary view were used for accurate classification (Fig. 4).

Three-dimensional computed scan of a multifragment scapular body fracture producing a malrotation of the intact glenoid fossa.
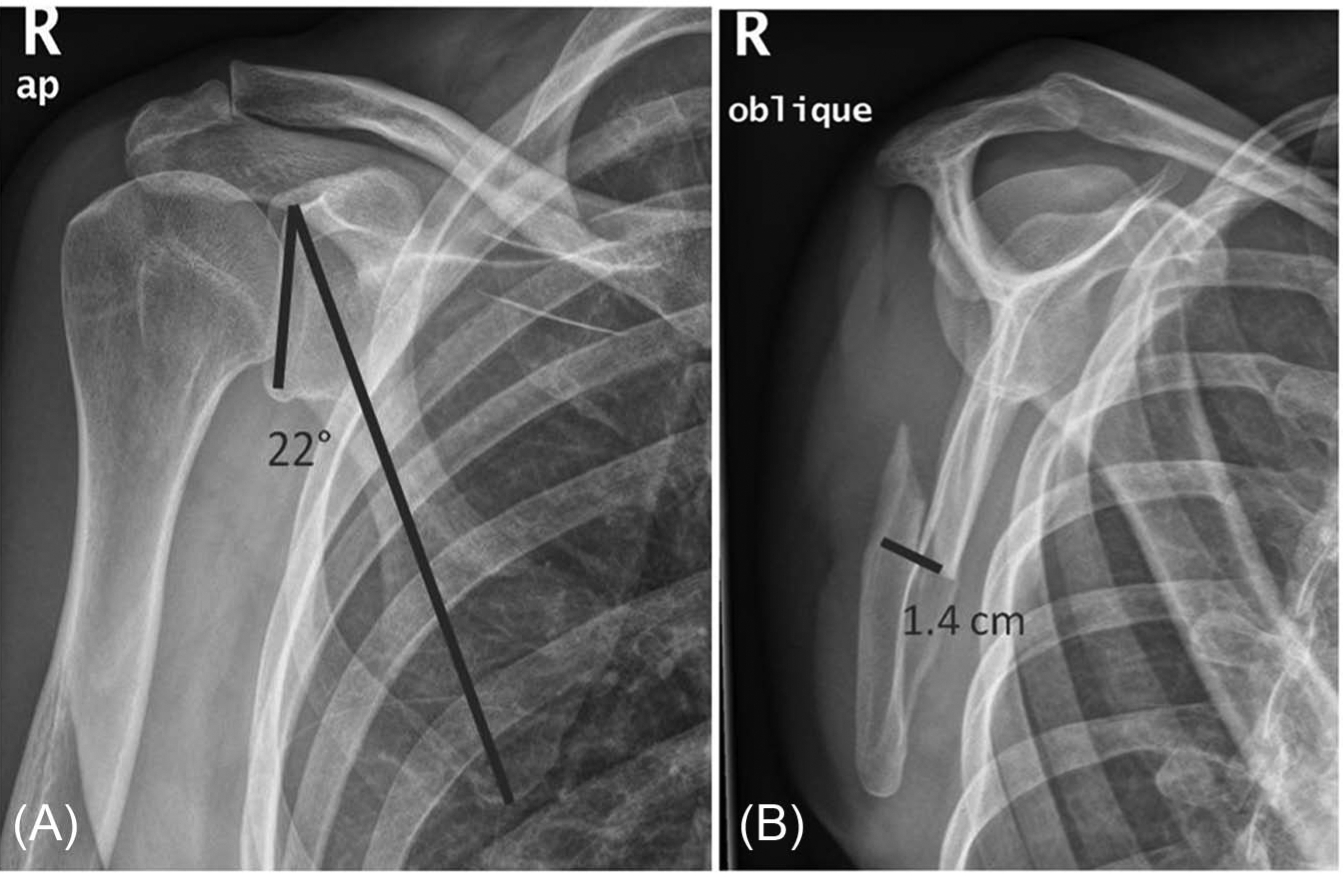
A) Anteroposterior radiograph. B) Y view of a fracture in the scapula wing region. The glenopolar angle as well as the fracture dislocation is marked.
One major restriction of our study is the heterogeneity of treatment in patients with a scapula neck fracture and a concomitant clavicula fracture. As our study focused on the scapula neck only, all patients without osteosynthesis in the scapular neck region, which includes those with operative treatment of clavicula fractures as well, were grouped in the nonoperative group. We acknowledge that an additional subgroup analysis of patients with and without operative treatment of concomitant clavicular fractures would have been valuable. However, this was not possible because of lack of adequate data in the analyzed studies. Scapular neck fractures with combined clavicula fractures could be divided into 127 patients without surgery to the clavicular bone and 80 patients with osteosynthesis of the clavicula.
Another restriction was the use of various outcome measures so pooling of data was not always possible. Furthermore, the definition of some outcome parameters was not clearly defined, like the overall function, where numerous scores were assessed.
The purpose of this study was to isolate effects of operative versus nonoperative treatment in scapula neck fractures. Given the limitations mentioned above, we think it is justified from our results to summarize the following conclusions:
Scapular neck fractures are associated with a significant number of concomitant injuries, influencing the treatment options and the timing of shoulder injuries. The influence of the functional outcome is not clearly understood but with a trend to worse outcome in multiple injured patients.
The rate of neck fractures compared with all scapula fractures is high and seems to be underestimated when only analyzing previous studies.
Pain-freeness was seen in a higher rate in the patient group undergoing surgery for surgical neck fractures.
GPA and translational dislocation are minimized in the operative treatment groups. There are indications that this might lead to better long-term outcome.
The overall rate of complications for surgical treatment was 10%.
However, as there was a wide heterogeneity of the underlying studies, caution should be exercised extrapolating these findings in the clinical decision-making process. The authors wish to express their need for future multicenter studies with a coherent evaluation system and clearly defined outcome variables to give more precise advices regarding the treatment of scapula neck fractures.