
Abstract
Background:
Clubfoot is one of the most frequent congenital malformations in the world. Non-operative methods follows limiting surgery to a minimum. The modified Copenhagen method has not been studied enough.
Study Design:
longitudinal retrospective study.
Objectives:
To evaluate prognostic factors for clinical rehabilitation with the modified Copenhagen method in a 10-year follow-up period.
Methods:
A retrospective study was carried out on a 10-year follow-up of 82 children diagnosed with clubfoot at birth and treated with the modified Copenhagen method. Their sex, side, severity, bilaterality, forefoot orientation, and age when the nonoperative treatment was started were registered, and a cluster analysis was performed to determine which variables were most significant for predicting whether surgical treatment was needed.
Results:
Of the clubfeet, 13.4% were grade I, 65.9% were grade II, and 20.7% were grade III according to the Harrold and Walker classification. In total, 58 patients needed surgery at some point during the follow-up period. The severity and talo-first metatarsal angle made it possible to determine whether the patients required surgery in 68% (56/82) of the cases.
Conclusion:
The results of the study suggest the possibility of providing physicians with an algorithm which might facilitate assessing whether the children will require surgery or not, depending on the data obtained from the cluster analysis.
Clinical relevance
This study provides health professionals with an algorithm that might facilitate assessing whether the children will require surgery or not.
Background
Along with developmental hip dislocation and scoliosis, clubfoot is one of the most frequent congenital malformations in the world.1–6 The worldwide prevalence of clubfoot is approximately 1/1000, with higher frequencies in Polynesia (6.8/1000), South Africa (3.5/1000), and Malaysia (4.5/1000).7–9 It appears less often in other Asian countries (0.57/1000), and its prevalence in the Caucasian population is similar to the world average (1.2/1000).7–9 In Spain, the prevalence of clubfoot, registered in the last year (2010) in the Cooperative Study of Congenital Malformations (ECEMC), was 3.1 for every 10,000 live newborns. 10 The high average frequency of the appearance of clubfoot in newborns reflects the significance of this congenital malformation, as well as the importance of its proper diagnosis and early treatment.
The treatment of clubfoot needs to be started as early as possible after birth,2,3 especially rehabilitation. Untreated children usually walk on the outer part of their feet, which leads to the formation of hyperkeratosis, arthritis, significant limitations in mobility and, consequently, abnormal psychomotor development. With regard to the initial treatment applied in clubfoot cases, several studies have examined the aftereffects of surgical treatment in the long term, including overcorrection, recurrence, or pain.3,6–11 These results have revived interest in nonoperative treatment methods for clinical rehabilitation, especially the Ponseti method11–17 and French method.17–23
At the “Virgen Macarena” University Hospital in Seville (Spain), children with clubfeet have been treated nonsurgically for over 30 years using the modified Copenhagen method (MCM; Figures 1–3).24,25 Currently, the aforementioned method shares the same basic objectives with Ponseti and French methods: limiting surgery to a minimum and, if surgery be necessary, using minimally aggressive techniques.

One-day-old child with bilateral clubfoot grade II.

Child shown in Figure 1 after 1½ months under nonsurgical treatment using the MCM method (front view).

Child shown in Figure 1 after 1½ months under nonsurgical treatment using the MCM method (rear view).
The objectives of this study were to know what were the characteristics of congenital clubfoot treated with MCM at “Virgen Macarena” University Hospital between 1989 and 2003 and to know whether there were any prognostic variables of the cases treated in this hospital during that time that could have determined the need for or avoidance of surgery.
Methods
This was a longitudinal retrospective study that involved all the patients with clubfeet who received MCM treatment at the “Virgen Macarena” University Hospital, between 1989 and 2003. The reason for selecting this time period was that throughout those years, the children with clubfeet were treated by the same multidisciplinary medical team, so it could reduce the risk of bias related to the clinician who applied rehabilitation. The study was approved by the Virgen Macarena Hospital’s Ethical Committee.
The inclusion criteria were as follows: children diagnosed with clubfeet who had not received any previous surgical or nonsurgical treatment. Children who met these criteria, but evidenced other congenital syndromes, such as Larsen syndrome, Freeman–Sheldon syndrome, diastrophic dysplasia, congenital multiple arthrogryposis, Streeter bands, or other associated congenital diseases, were excluded, as were those with incomplete medical records or who had not completed their treatment.
In total, 95 children with clubfoot were initially identified. After reviewing their medical records, 5 were excluded due to missing data, 3 because the patients showed signs of clubfeet associated with another congenital syndrome, and 5 because their treatment was not completed. The final sample included 82 children.
The variables used in this study were laterality of the deformity (unilateral or bilateral); severity (grades I, II, and II, per the Harrold and Walker scale 26 ); sex; and whether surgery was performed or not and, if so, the type of surgical treatment. The orientation of the forefoot (normal or adducted based on a measurement of the talo-first metatarsal angle in dorsoplantar x-rays, with angles below 20 degrees considered to be normal)26–28 was also recorded. These variables were measured 1, 3, and 10 years after the start of clubfoot nonoperative treatment. Harrold and Walker 26 established three grades of severity for this deformity: If the foot could be held at or beyond the neutral position, the deformity was described as mild or grade I; if the foot could not be pushed to neutral and yet the fixed equinus or the angle of varus was 20 degrees or less, it was considered the deformity to be moderate or grade II; when the fixed deformity was of more than 20 degrees of varus or equinus, the deformity was considered severe or grade III.
The MCM treatment involved a first stage aimed at the flexibilization of the clubfoot by means of soft, passive mobilization of the foot joints. Then, a second phase was applied in which the correction of the deformity components was begun by progressively stretching the ligaments, the joint capsules, and the contracted muscles in physical therapy sessions that were conducted 5 days a week for approximately 30 min per foot. Stretching and manipulating the foot were performed starting by correcting adduction; then cavus; hindfoot varus; and, finally, equinus. This was combined with muscular stimulation to prompt active movement of the foot in all its planes, with special emphasis on the hypotonic muscle groups. Muscular stimulation was done with a toothbrush applied to the lateral area of the foot. In the time between the physical therapy sessions, the feet were fixed in the position of the maximal correction attained. To complete the session, a 5-cm-wide cotton bandage and two strips of plaster were applied to maintain the obtained correction. Initially, this corrective bandage was used, and when the foot was totally corrected (approximately 1 month after physical therapy was started), an active Larsen’s splint (knee ankle foot orthosis (KAFO)) was customized to each patient. This splint consists of three elements: a part made of thermoplastic that is fixed to the upper third of the thigh, a lower part of the same material adapted to the desired correction of the components of the foot, and a third part consisting of a metal plate that joins them laterally. The plate has a system of screws and holes in the upper side, which allow lengthening it as the child grows. The splint forces the knee to be placed in 90 degrees flexed and has a tensioning system on the lateral side to act more directly on the stretching of the Achilles tendon. That is, the splint maintained the foot in a reduced position through three support points (anterior-lateral and anterior-medial border of the foot and anterior face of the middle third of the thigh) and through a system of elastic straps that control and correct supination, adduction, and equinus.
The data were analyzed using SPSS v.20 (SPSS Science, Chicago, IL). 29 A general descriptive analysis was carried out, including an assessment of averages and standard deviations of the quantitative variables, as well as the absolute and relative frequencies of the qualitative variables expressed as percentages. To quantify the magnitude of this congenital malformation in the hospital’s area and to compare these data with data from previous studies, the prevalence of clubfeet during the period under study was calculated. The association among qualitative variables was evaluated using the chi-square test or, in the case of 2 × 2 contingence tables, Fisher’s exact test. An inferential analysis using the Mann–Whitney and Kruskal–Wallis statistical tests was also performed to determine how some of the variables were distributed. Finally, a cluster analysis was made in two phases to determine whether different groups could be established to determine whether a surgical treatment would be required or not and, if so, when it would be performed within the 10 years being studied. This analysis made it possible to classify groups on the basis of both qualitative and quantitative criteria.
Results
The total number of clubfeet included in the study was 123 (82 patients). Bilateral and unilateral deformities were found to be identical in their percentages at 50% (41/82) each. Among the unilateral deformities, right feet were affected in 41.4% (17/41) of the cases, and left feet were affected in 58.6% (24/41). The sample included 57 males (69.5%) and 25 females (30.5%). The results for clubfeet severity indicated that 13.4% (11/82) of the children evidenced grade I clubfeet, 65.9% (54/82) grade II, and 20.7% (17/82) grade III. Most of the patients, 92.7% (76/82), began treatment with the MCM before they reached 1 week of age. The rest of the patients (six) began a nonoperative treatment when they were 14, 25, 30, 40, 145, and 180 days old, respectively. The forefoot was considered to be normal in 93.9% of the feet treated with the MCM (77 cases) at both the beginning and end of the follow-up period. In the remaining 6.1%, the foot was found to be in adduction throughout the follow-up period. The results of the measurements of the talo-first metatarsal angle in dorsoplantar x-rays at the time of the three reviews are shown in Table 1. The chi-square test was applied to determine the ratio between the qualitative variables. There were no differences by sex in the rest of the qualitative variables considered in the study (uni- or bilateral deformity, normal or adducted forefoot, severity of the deformity).
Results of measurements of the talo-first metatarsal angle in dorsoplantar x-rays during the three reviews.

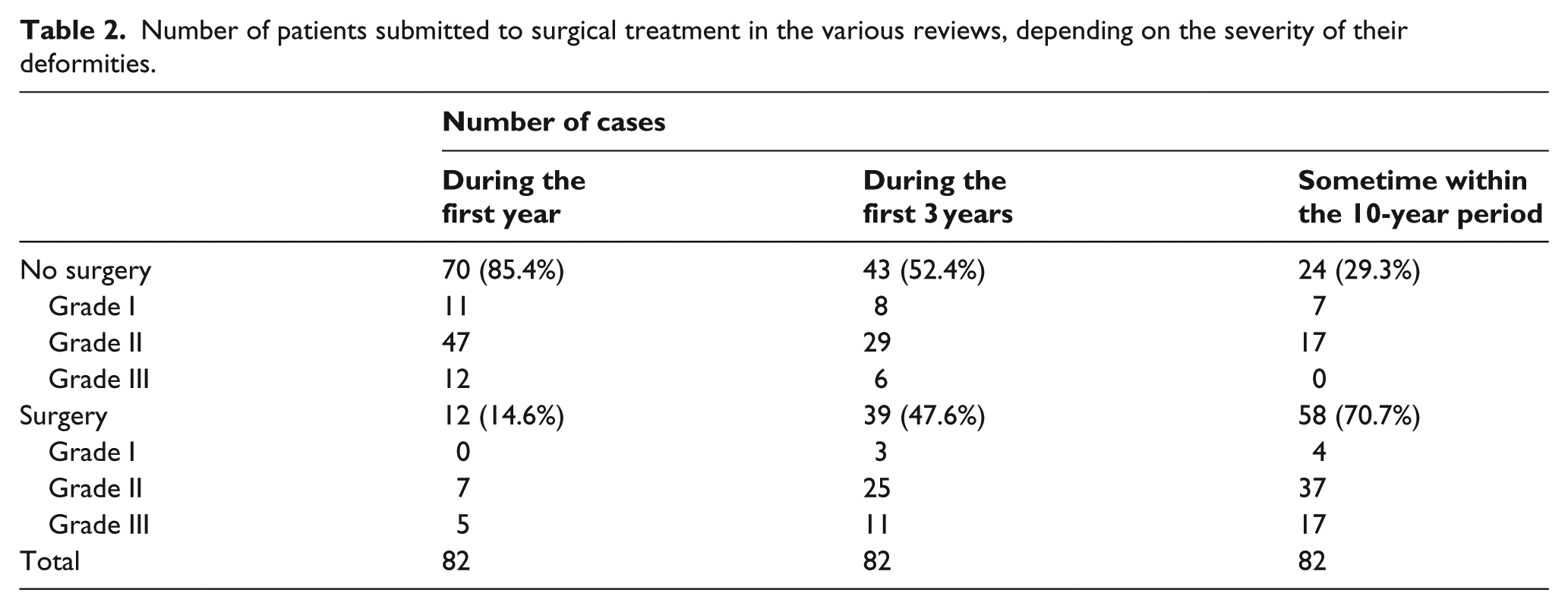
The results for the number of patients who received surgery during the three reviews, based on the severity of their deformities, are shown in Table 2. In total, 58 patients required surgery at some point within the 10-year follow-up period. Surgery on both feet was performed in all cases of bilateral clubfeet. The subsequent release technique (Achilles Z-plasty and talus calcaneous capsulotomy) was applied in all cases, except for two grade III patients who had received percutaneous Achilles tenotomies when they were reviewed 3 years after beginning the nonsurgical treatment.
Number of patients submitted to surgical treatment in the various reviews, depending on the severity of their deformities.
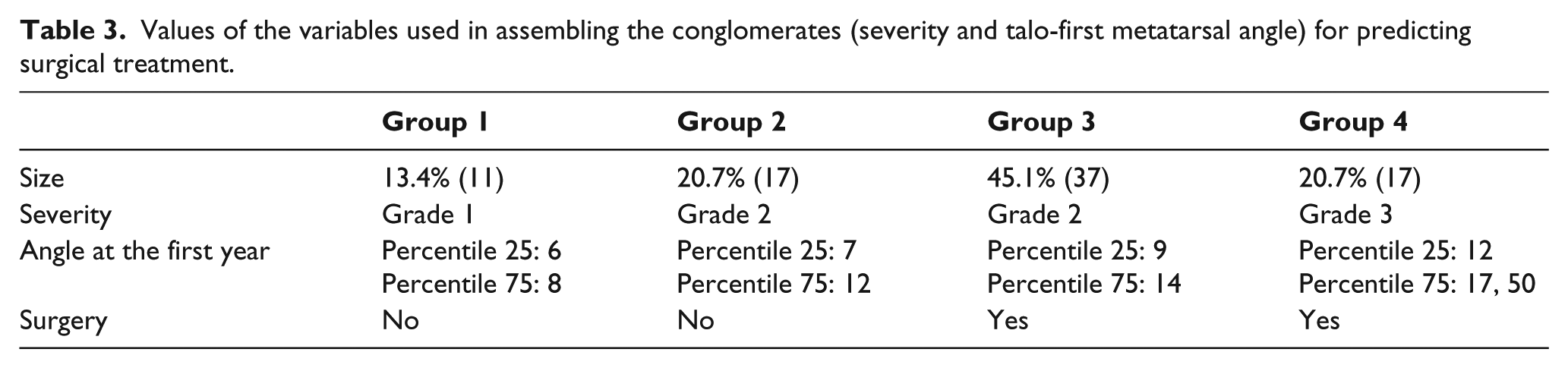
To determine the number of patients who would and would not have required surgical treatment, the data obtained from the registered variables were used in a two-phase cluster analysis. The variables evidencing the greatest relevance were severity and the talo-first metatarsal angle 1 year after the start of the nonsurgical treatment. Using these two variables, the quality value obtained in the groups was 0.7. As this value is higher than 0.5, it was considered to be of good quality. Figures 4 and 5 contain graphs showing the composition concerning the total number of groups obtained. Because there were no lost cases, it was assumed that the number of groups was appropriate for the established purposes. Table 3 shows the size and composition of the conglomerates and the values of the variables used to form them (severity and talo-first metatarsal angle) as variables for predicting surgical treatment. With regard to the values of the talo-first metatarsal angles, the values of percentiles 25 and 75 are shown. As shown in this table, when the talo-first metatarsal angles in the x-rays performed 1 year after the start of treatment were up to 12 degrees and the severity was up to grade II, the patients did not require surgical treatment. In contrast, with a 9-degree angle in their x-rays and at least grade II severity, they did require surgery. Therefore, there is an interval of uncertainty in the cases with grade II severity and an x-ray angle between 9 and 12 degrees.
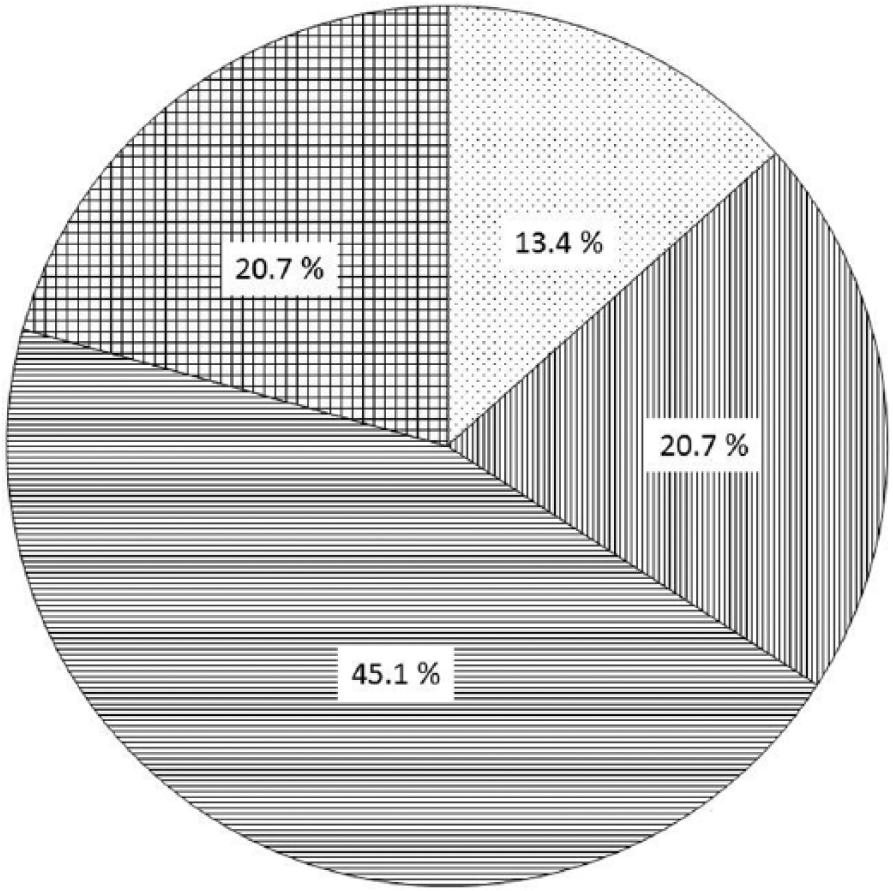
Size and contents of the obtained conglomerates. The smallest conglomerate contained 11 cases (13.4%); the biggest conglomerate contained 37 cases (45.1%). Size ratio (biggest/smallest conglomerates) = 3.36.
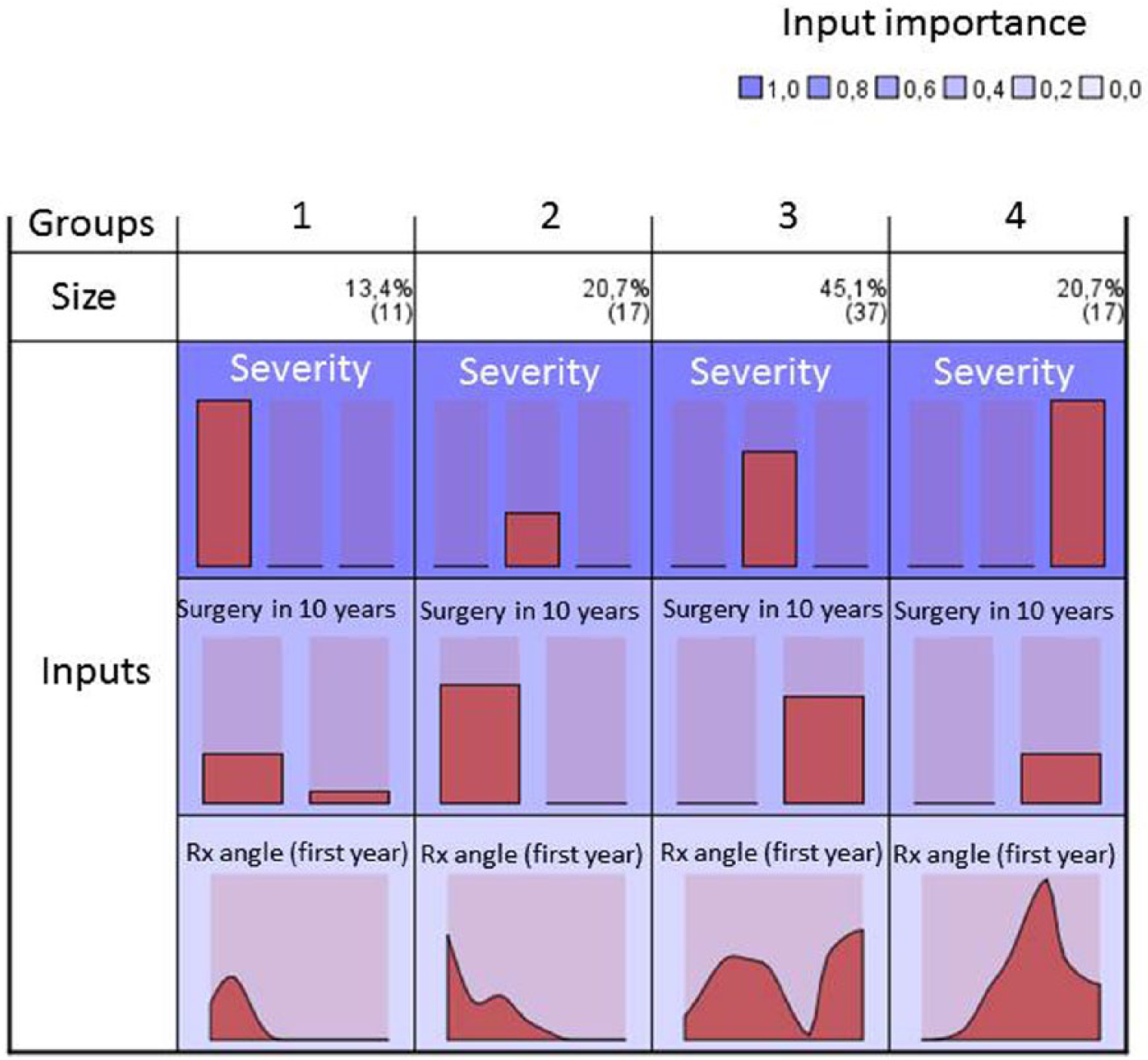
Graph representing the conglomerates on the basis of the significance of the predicting variable.
Values of the variables used in assembling the conglomerates (severity and talo-first metatarsal angle) for predicting surgical treatment.
Discussion
The main objectives of this work were to obtain better knowledge of the behavior and distribution of clubfoot over the years and to identify the variables that provide greater relevance as predictive factors for needing surgical treatment. The authors consider that this study has certain limitations, such as ignoring some additional factors that could influence the results—as they were not included in the available medical records—or the analysis of the MCM in only short and medium terms. In future research, the MCM would need to be explored in the long term, especially on completion of the child’s growth. The design and execution of aleatory clinical tests would also be of interest to compare the efficacy of the most used nonoperative treatment methods in clubfeet and to determine which one is most effective.
Studies carried out in diverse populations worldwide have shown that clubfeet display a homogeneous distribution by sex and laterality.7–9 In this study, it was observed that there were 57 boys and 25 girls, equivalent to a 2:1 ratio. This result coincides with those reported by Torres-Gómez et al. 5 in the Mexican population. Roye et al. 30 carried out a clubfoot review and established that its incidence was twice as high in males as in females. Moorthi et al.’s 31 study of 682 children with clubfeet in Texas (United States) also resulted in a 2:1 male–female ratio. Similar results were obtained by Pietrucin-Materek et al. 32 in children in the United Kingdom with clubfeet who were treated between 1994 and 2004. Ezeukwu and Maduagwu 33 established that the deformity appeared more frequently among males in Nigeria.
Regarding the laterality of clubfeet, this study showed that half of the patients presented with bilateral clubfeet. Similar data were reported by Chung et al. 34 in Hawaii and Lochmiller et al. 35 in Texas. The unilateral clubfeet in our study were on the right side in 17 cases and on the left side in 24 cases, thus differing from the results published by DeValentine 17 or Lochmiller et al., 35 whose studies showed that unilateral clubfeet occurred more often on the right side.
A further objective of this work involved knowledge of predictive factors for the surgical treatment of clubfoot. In total, 58 patients in our sample required surgery at some point during the 10-year period after beginning the nonoperative treatment. Regarding the Ponseti method, good results were obtained in the study by Herzenberg et al. 18 However, 91% of the clubfeet required percutaneous Achilles tenotomy procedures. Morcuende et al. 36 reported that 98% of the studied clubfeet cases were corrected with the Ponseti method, but 86% of them required an Achilles tenotomy to attain the correction. Matuszewski et al. 37 found that when 35 patients were submitted to the Ponseti method, 34 required percutaneous Achilles tenotomies. Regarding the French method, Bensahel et al. 38 reported that 52% of the feet reviewed in their study required surgical treatment. Contrarily, Van Campenhout et al. 39 stated that 75% of the feet included in their study required surgical treatment. Richards et al. 40 and Karol et al.41,42 reported that 48% and 45% of their clubfeet, respectively, did not require surgery to attain good results. Rampal et al. 43 noted that 45.5% of the patients in their study required surgery before completing their third year of treatment.
The severity of clubfeet, as assessed by diverse types of classifications, is the factor that has been studied more frequently. Some studies, such as those by Ponseti and Smoley 21 or Masse 23 , consider the severity of clubfeet to be the factor with the greatest influence on the prognosis. Further studies have led to reports with similar statements relating the results of clubfoot treatment with the severity of their components, which is in agreement with the results of our study.36,40,43–47 The factors taken into account to assess which ones are most relevant as predictive factors for needing surgical treatment were sex, laterality, the condition of the forefoot, and the clubfoot’s severity. The results obtained did not evidence any statistically significant differences in the evolution of clubfeet related to the child’s sex or clubfoot laterality. Contrarily, it was observed that the variables that most influenced the sorting of participants into the designated groups were the talo-first metatarsal angle and severity. Severity in clubfeet is directly related to needing foot surgery. As shown in Table 1, all the patients with grade III clubfeet and 37 of the 54 patients with grade II clubfeet required surgery at some point during the 10-year follow-up period.
Chu and Lehman 48 raised the possibility that other factors—such as the age at which the treatment was started, the splinting time or the parents’ cooperation—might have a more significant role in the prognosis of clubfeet than the ones given so far. In our study, most of the children had begun nonoperative treatments before they were 1 week old. The small number of patients whose treatments were started later hindered the possibility of making comparisons to obtain rigorous conclusions regarding the effect of beginning treatment early on prognosis. Dimeglio and Canavese 49 suggested that improper footwear, the types of physical activity performed by the children, and a lack of cooperation by parents might be factors to be taken into account in the establishment of a clubfoot prognosis.
Conclusion
To conclude, the children with grade I clubfeet and those with grade II clubfeet and a talo-first metatarsal angle ≤8 degrees did not require surgery. The children with grade II clubfeet and a talo-first metatarsal angle ≥12 degrees, as well as those with grade III clubfeet, did require operations. Some amount of uncertainty would remain for children with grade II clubfeet and a talo-first metatarsal angle between 9 and 12 degrees, who could not receive specific diagnoses regarding whether they would need surgery. Discarding these cases, the remaining of the cases would have had a clearer prognosis with regard to their future need for surgery.
Footnotes
Acknowledgements
The STROBE guidelines have been used to structure this article.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.