
Abstract
Background and Aims:
Population-based register data from the National Joint Register of Australia and England and Wales have revealed that the mid-term outcome of cementless large diameter head metal-on-metal total hip arthroplasty is inferior to that of conventional cemented metal-on-polyethylene total hip arthroplasty. The aim of this study was to compare the results of cementless large diameter head metal-on-metal total hip arthroplasty with conventional cemented arthroplasty in Finland. The second aim of this study was to compare the cementless large diameter head metal-on-metal models with each other.
Material and Methods:
Based on the data extracted from the Finnish Arthroplasty Register, the risk of revision of 8059 cementless large diameter head metal-on-metal total hip arthroplasties performed during 2002–2009 was analyzed using Cox regression model. The revision risk of these hips was compared to that of 16,978 cemented metal-on-polyethylene total hip arthroplasties performed during the same time period.
Results:
In the Cox regression analysis, there was no difference in revision risks between cementless large diameter head metal-on-metal total hip arthroplasty and cemented metal-on-polyethylene total hip arthroplasty (relative risk = 0.90, confidence interval = 0.74–1.10, p = 0.3). However, in female patients aged 55 years or above, cementless large diameter head metal-on-metal total hip replacements showed a significantly increased risk of revision as compared to cemented total hip replacements (relative risk = 1.33, confidence interval = 1.04–1.70). Compared to the reference implant in this study (cementless Synergy stem combined with Birmingham Hip Resurfacing [BHR] cup), the CementLess Spotorno (CLS) stem combined with Durom cup had a 2.9-fold (95% confidence interval = 1.17–6.90) increased risk of revision.
Conclusions:
We found that cementless large diameter head metal-on-metal total hip arthroplasty had short-term survivorship compared with cemented total hip arthroplasty at a nation-wide level. However, in female patients aged 55 years or above, cementless large diameter head metal-on-metal total hip arthroplasty showed inferior results. Furthermore, implant design had an influence on revision rates. Longer follow-up time is needed to assess the success of large diameter head metal-on-metal total hip arthroplasty.
Introduction
Results obtained from the Scandinavian arthroplasty registries (1–3) on a nation-by-nation basis indicate that cemented total hip arthroplasty (THA) is the treatment of choice for severe hip osteoarthritis (OA). However, in recent studies, cementless implants as well-defined groups have had comparable survival rates than cemented implants (4). Unfortunately, cementless cups with polyethylene liners have had a common problem of wear, osteolysis, and high incidences of revisions in the medium term and long term (5).
Cementless implants with large diameter head metal-on-metal (LDH MoM) bearing surfaces have gained increasing popularity during the last few years in the hope of reducing wear and osteolysis. The LDH MoM THAs are supposed to have other advantages over conventional THA, such as increased range of motion to impingement and lower dislocation rate. These advantages are, however, only theoretical, as evidence from clinical trials is lacking. The first population-based reports of the short-term survival of cementless LDH MoM THAs have been poor (6). There has been a variety of early complications such as periprosthetic fractures and adverse reactions to metal debris (ARMD).
The aim of this study was to compare the results of cementless LDH MoM THAs with conventional cemented THAs based on the data from the Finnish Arthroplasty Register. The second aim was to compare the cementless LDH MoM THA models with each other.
Material and Methods
The Finnish Arthroplasty Register
Since 1980, the Finnish Arthroplasty Register has been collecting information on total hip replacements (7). Health care authorities, institutions, and orthopedic units are obliged to provide the National Institute for Health and Welfare with information essential for maintenance of the register. An English translation of the notification form used by the Finnish Arthroplasty Register has been discussed in an earlier study (2).
Study Population And Inclusion Criteria
During the study period 2002–2009, 16,978 conventional metal-on-polyethylene cemented THAs and 8059 LDH MoM THAs fulfilling the study criteria were performed in Finland for primary or secondary OA. With an LDH in this study, we consider those heads with diameter 38 mm or above. To reduce the skew in demographic distribution between patients operated with LDH MoM THA and those operated with conventional THA, patients older than 85 years of age were excluded. Also, those patients with a diagnosis of other reasons or rheumatoid arthritis were excluded. Only LDH MoM THA designs used in more than 100 operations during the study period were included. These criteria permitted the inclusion of seven LDH MoM THA designs. The implants (manufacturer), the number of implants included, and the proportion of all implants (%) were as follows: ReCap/Bi-Metric (Biomet), 4202, and 52% of all implants; M2a38/Bi-Metric (Biomet), 2459, and 31% of all implants; ASR/Summit (DePuy), 495, and 6% of all implants; BHR/Synergy (Smith & Nephew), 432, and 5% of all implants; Durom/ML-Taper (Zimmer), 197, and 2% of all implants; Durom/CLS (Zimmer), 154, and 2% of all implants; and ASR/Corail (DePuy), 120, and 1% of all implants.
The survival rate of LDH MoM THAs was compared to that of cemented THAs performed during the same time period. In addition, stratified analyses were performed for males and females aged <55 or ≥55 years. In these subanalyses by age and gender, revision risk of LDH MoM THA was compared to the revision risk of cemented THAs performed during the same time period. The LDH MoM THA group was further analyzed with regard to the influence of LDH MoM THA device, age at surgery, gender, diagnosis, implant design, hospital production volume, and femoral head diameter (classified as ≤44 mm, 45–49 mm, 50–54 mm, and ≥55 mm) on the risk of revision.
Statistics
Kaplan–Meier survival analysis was used to calculate the survival probabilities of implant with 95% confidence interval (CI). These survival data were compared using the log-rank test. Patients who died or left Finland during the follow-up period were censored at that point. Adjusted revision rates were calculated using Cox multiple regression analysis. The proportional hazards assumption was controlled for by visual inspection of the Cox curves.
Inclusion of bilateral cases in a survival analysis violates the basic assumption that all cases are independent. However, it has been suggested that the effect of including bilateral cases in studies of hip and knee joint prosthesis survival is negligible (8). We therefore included all available cases to maximize statistical power. Relative risk (RR) estimates were calculated and presented with 95% CI. The level of significance was 95%.
Revisions were linked to the primary operation by using a personal identification number. The end point for survival was defined as revision when either one component (including the femoral head) or the whole implant was removed or exchanged. Revision for any reason, revision for aseptic loosening, revision for dislocation, revision for infection, and revision for periprosthetic fracture each served separately as an end point. In eight revisions, the recorded indication for revision was “other reason.” Kaplan–Meier survival data were used to construct the survival probabilities of implants. Survival probabilities were determined only if there were at least 20 hips at risk at 3, 5, and 7 years. The survival data were compared using the log-rank test. Patients who died or left Finland during the follow-up period were censored at that point. The Cox multiple regression model was used to study the differences between groups and to adjust for potential confounding factors. The factors studied with the Cox model were age, gender, diagnosis, and implant, when conventional cemented THA group was compared to LDH MoM THA group. The factors studied with the Cox model were the seven LDH MoM THA devices, age, gender, diagnosis, hospital production volume (≥100/<100 procedures), and femoral head diameter (categorized as ≤44 mm, 45–49 mm, 50–54 mm, and ≥55 mm), when other LDH MoM THA devices were compared to the BHR/Synergy. Effect of age on survivorship was also analyzed by dividing the patients into two age groups: those under 55 years and those 55 years of age or older. Cox regression analyses provided estimates of survival probabilities and adjusted risk ratios for revision. Estimates from the Cox analyses were used to construct adjusted survival curves at mean values of the risk factors. The Wald test was applied to calculate p values for data obtained from the Cox multiple regression analysis. Differences between groups were considered to be statistically significant if the p values were less than 0.05 in a two-tailed test.
Results
Demographic data are shown in Table 1.
Demographic data.
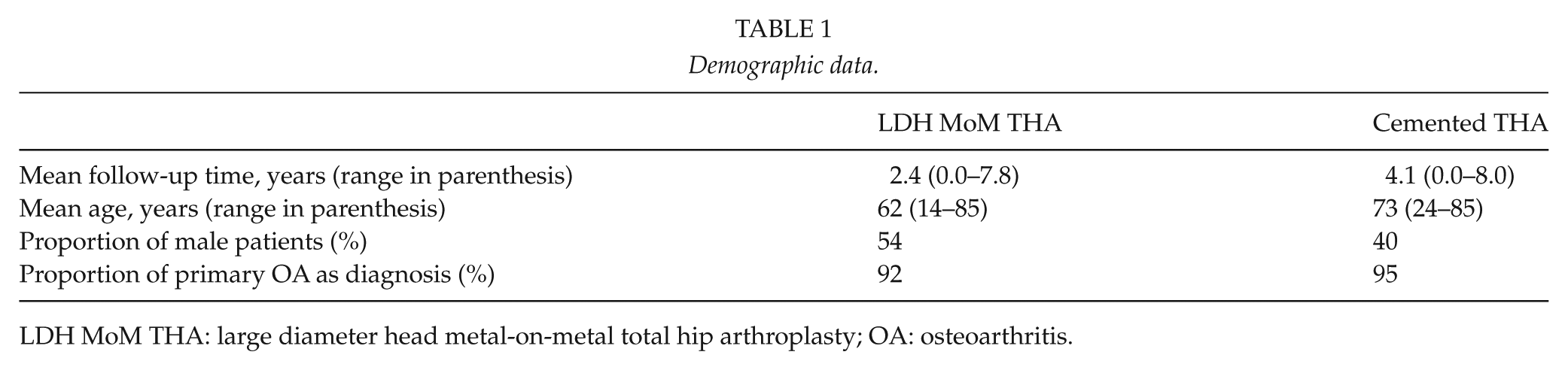
LDH MoM THA: large diameter head metal-on-metal total hip arthroplasty; OA: osteoarthritis.
The main reasons for the revision of LDH MoM THA were aseptic loosening and fracture, whereas cemented THAs were revised most often because of dislocation. Unspecified reasons for revision (“other”) were recorded in 4% of the LDH MoM THA revisions as compared to 3% in THA revisions (Table 2).
Reasons for revision.
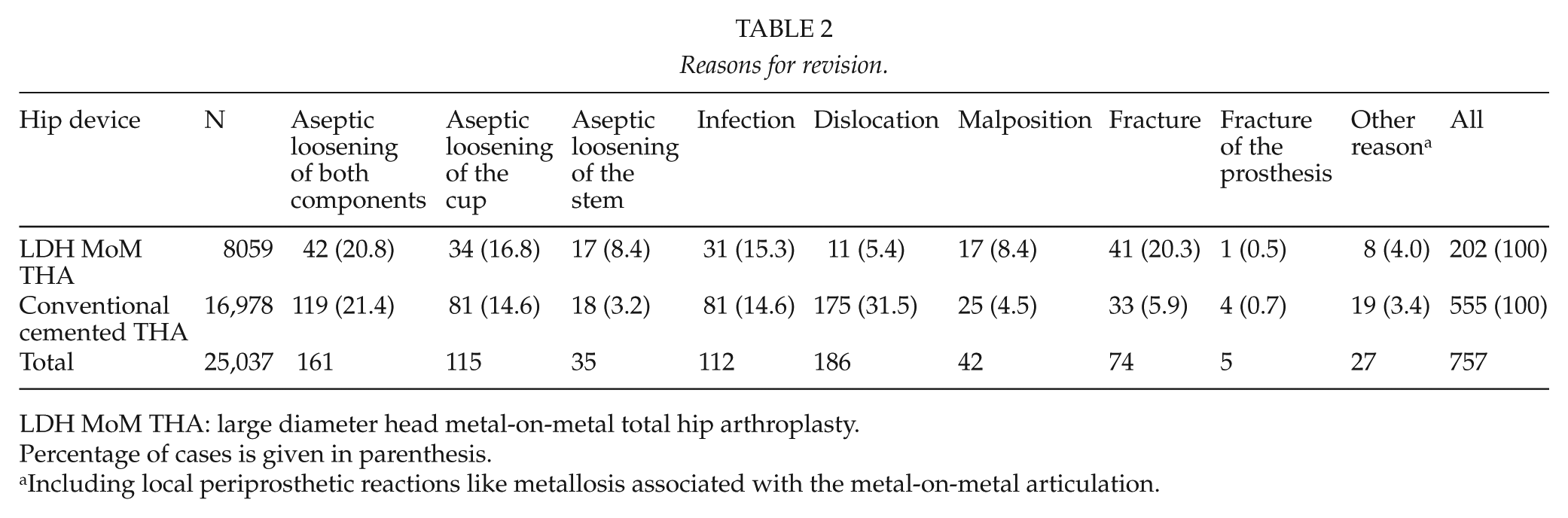
LDH MoM THA: large diameter head metal-on-metal total hip arthroplasty.
Percentage of cases is given in parenthesis.
Including local periprosthetic reactions like metallosis associated with the metal-on-metal articulation.
The 7-year unadjusted Kaplan–Meier survival was 96% (95% CI = 95–97) for LDH MoM THA and 95% (95% CI = 95–96) for the cemented THA (Table 2). In the Cox regression analysis, there was no difference in revision risk between LDH MoM THAs and cemented THA (RR = 0.90, CI = 0.74–1.10, p = 0.3) (Table 3, Figs 1 and 2).
Survival of LDH MoM THA and conventional cemented THA, the reference group.
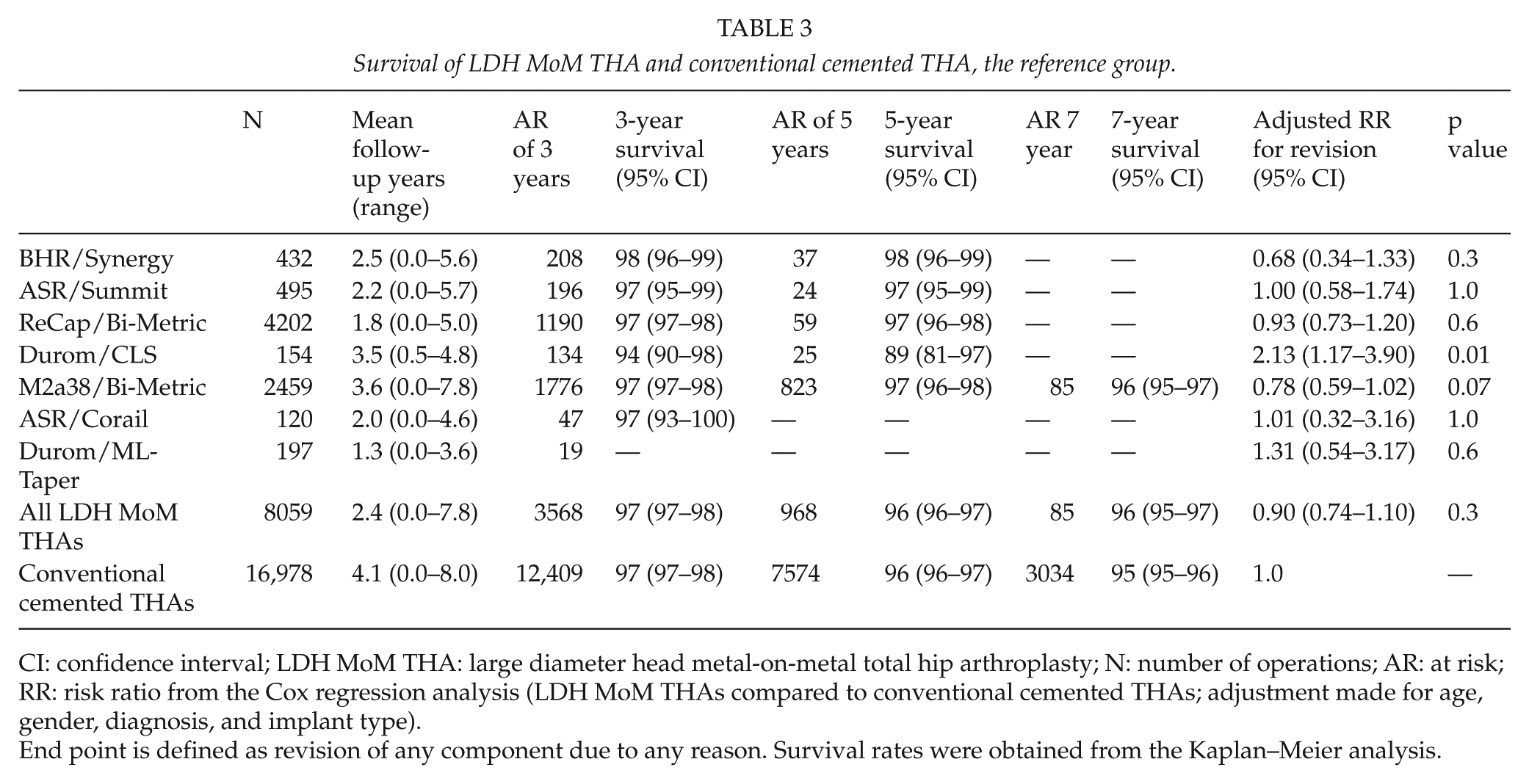
CI: confidence interval; LDH MoM THA: large diameter head metal-on-metal total hip arthroplasty; N: number of operations; AR: at risk; RR: risk ratio from the Cox regression analysis (LDH MoM THAs compared to conventional cemented THAs; adjustment made for age, gender, diagnosis, and implant type).
End point is defined as revision of any component due to any reason. Survival rates were obtained from the Kaplan–Meier analysis.
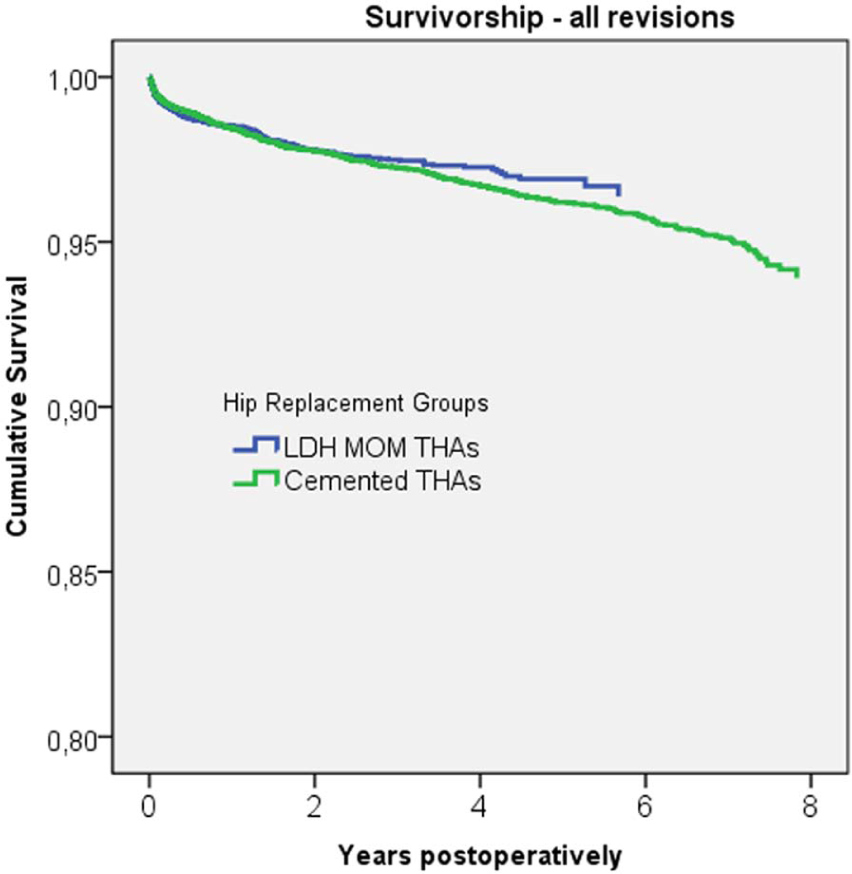
Cox-adjusted survival curves of 8059 cementless LDH MoM THAs and 16,978 cemented THAs. The end point was defined as revision for any reason. Adjustment was made for age, gender, diagnosis, and implant.
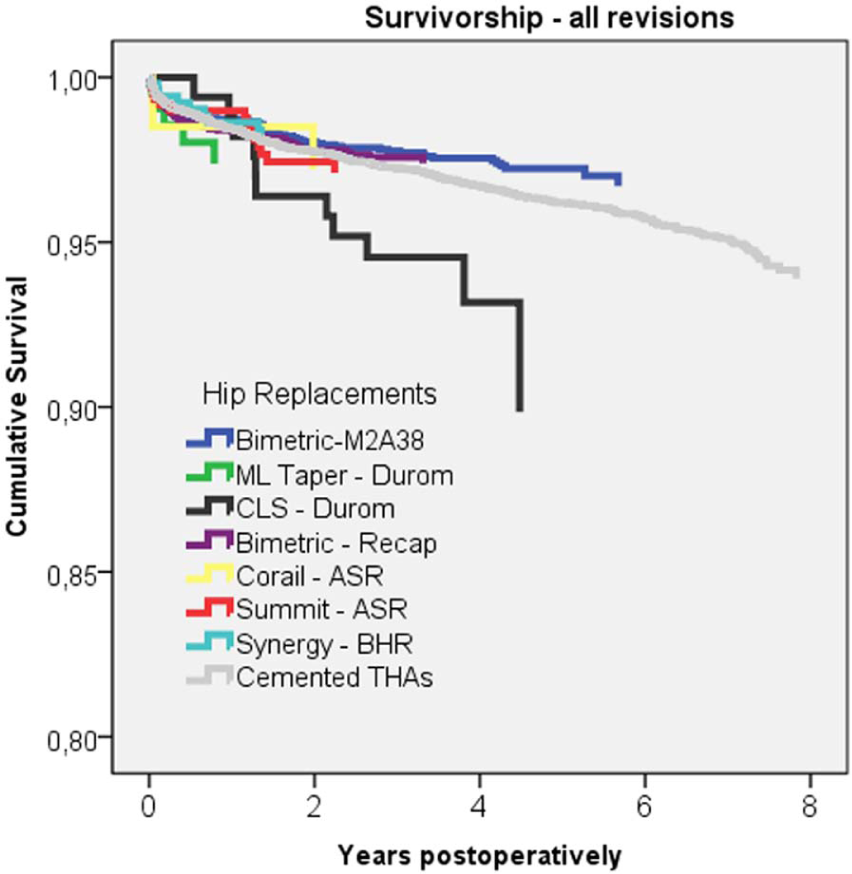
Cox-adjusted survival curves of seven cementless LDH MoM THA designs (432 BHR/Synergy, 495 ASR/Summit, 4202 ReCap/Bi-Metric, 154 Durom/CLS, 2459 M2a38/Bi-Metric, 120 ASR/Corail, 197 Durom/ML-Taper) and 16,978 cemented THAs. The end point was defined as revision for any reason. Adjustment was made for age, gender, diagnosis, and implant.
In both male and female patients aged below 55 years, the revision risk of the cementless LDH MoM THA was decreased compared to that of the cemented THAs (RR = 0.38, CI = 0.17–0.87, p = 0.02 and RR = 0.46, CI = 0.22–0.93, p = 0.03, respectively). However, female patients with LDH MoM THA aged 55 years or above had an increased revision risk compared to those with cemented THA (RR = 1.33, CI = 1.04–1.70, p = 0.02).
When we compared different LDH MoM THA designs using BHR/Synergy as a reference implant, Durom/CLS had a higher risk of revision than BHR/Synergy (RR = 2.82, CI = 1.16–6.82, p = 0.02) (Table 4). CI for the other designs showed considerable overlap, and the analysis does not permit any ranking between them. Femoral head diameter, age group (<55 or ≥55 years), gender, diagnosis, or hospital volume (<100/≥100 procedures) did not have a statistically significant influence on revision rate (Table 4).
Relative risk of revision with 95% CI in 8059 LDH MoM THAs.
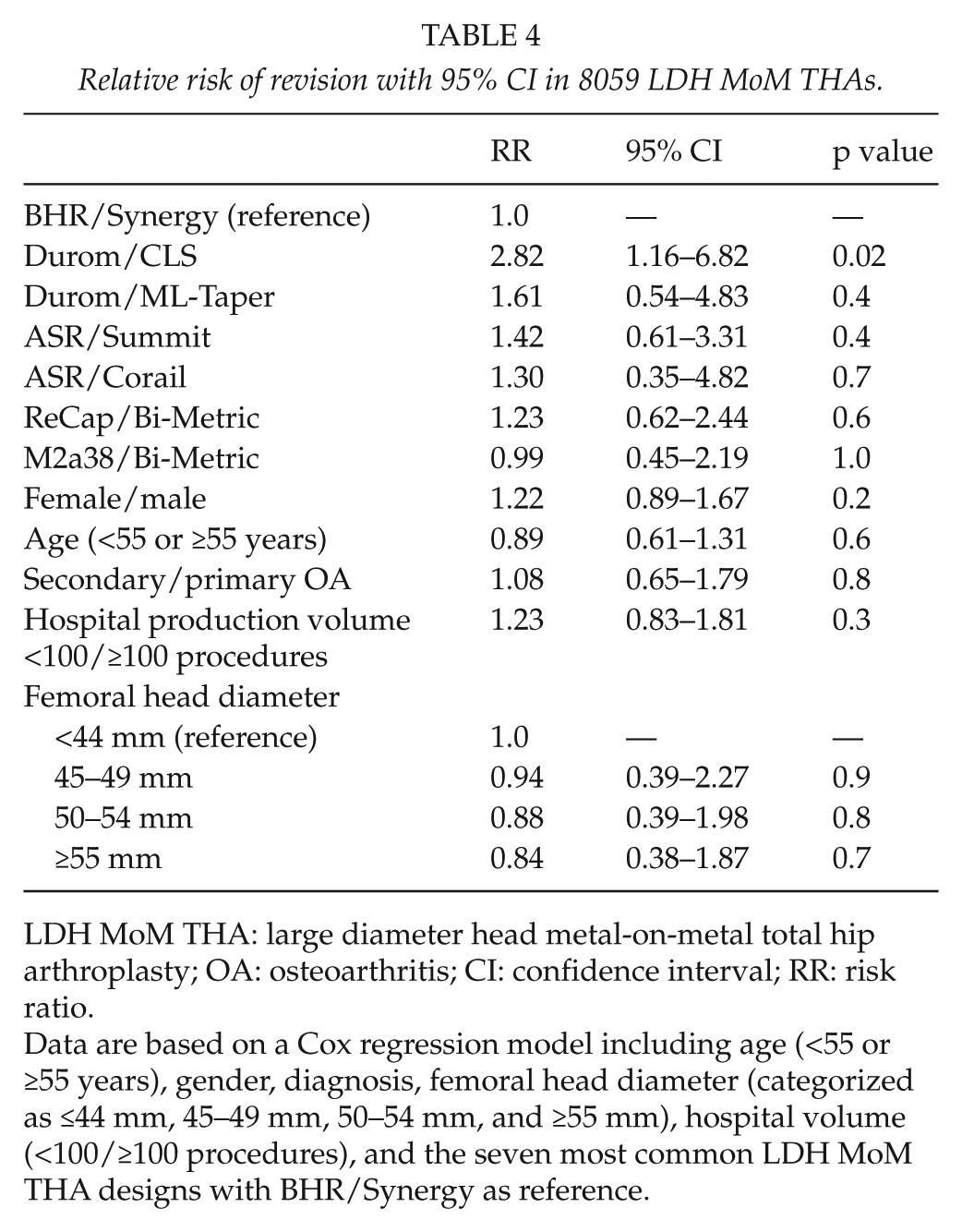
LDH MoM THA: large diameter head metal-on-metal total hip arthroplasty; OA: osteoarthritis; CI: confidence interval; RR: risk ratio.
Data are based on a Cox regression model including age (<55 or ≥55 years), gender, diagnosis, femoral head diameter (categorized as ≤44 mm, 45–49 mm, 50–54 mm, and ≥55 mm), hospital volume (<100/≥100 procedures), and the seven most common LDH MoM THA designs with BHR/Synergy as reference.
Discussion
We found that cementless LDH MoM THA had comparable short-term survivorship than cemented THA at a nation-wide level. However, in female patients aged 55 years or above, cementless LDH MoM THA showed inferior results. Furthermore, implant design had an influence on revision rates. Dislocation tendency was much higher (over sevenfold) in the conventional THA group than in the LDH MoM THA group. This may explain most of the differences in revision rates between cemented and cementless implants. Fracture risk was prominent (twofold) when cementless implants were used.
We acknowledge that this study has some methodological shortcomings. We were not able to perform radiological analyses, which could have detected silent osteolysis or adverse biological reactions linked to MoM articulation (9, 10). Furthermore, we are not aware of the blood chromium or cobalt values of the MoM patients. Patients in the LDH MoM THA group had a lower mean age than patients in the conventional THA group. There were also more male patients in the LDH MoM THA group. These problems were adjusted for as far as possible by the use of regression models.
The follow-up time was short. With longer follow-up, other reasons for revision—and especially those related to wear and ARMD—can be supposed to change the relative distribution of revisions. The total number of revisions was also relatively low, permitting only a minimum of stratified analysis and increasing the sensitivity to random effects of single revision cases.
Recent reports from national joint replacement registers have shown increased revision rates of LDH MoM THAs compared to conventional arthroplasty (6, 11). According to the Australian arthroplasty register, the cumulative revision rate of LDH MoM THAs (head size >40 mm) in 5 years was 6.4% (CI = 5.5–7.4) (11). In our study, the 5-year survival of LDH MoM THAs was 96% (CI = 96–97), which is slightly higher than that published from Australia. The adjusted risk ratio for revision between LDH MoM THAs and conventional cemented THA did not differ significantly in our study. However, implant design had an influence on revision rates. Two designs, namely, M2a38/Bi-Metric and ReCap/Bi-Metric, were used in 82% of all cases. At present, the LDH MoM M2a38/Bi-Metric and ReCap/Bi-Metric implants have performed well in Finland. This is in accordance with the findings from the Australian register of the Recap-cup with M2a head surface.
Register data from Australia have revealed an increased revision rate for women compared to men using LDH MoM THA (11). In our analysis, female patients aged 55 years or above with cementless LDH MoM THA had an increased risk of revision compared to that of cemented THA. In the short term, elderly women with compromised bone quality are prone to periprosthetic fractures and early subsidence of the cementless stem. The supposed advantage of cementless implants is indeed the long-term durability of implant fixation. Femoral head size did not have an independent association with revision risk in our study. In the Australian register data, larger metal/metal head size (>32 mm) was associated with increased risk of revision compared to the smaller metal/metal head size (≤32 mm) (11). However, the most often used cup in Australia was ASR, and the third most often used cup was Durom. In our opinion, these LDH MoM THAs with well-known poor results (12, 13) make the results of the whole group of larger head size worse.
We used a limit of 100 LDH MoM THAs to separate low-volume hospitals from high-volume hospitals. There was a tendency that high hospital production volume was associated with reduced risk of revision, but this finding was not statistically significant.
Survival rates of 95%–100% for follow-ups between 5 and 15 years have been reported for the Bi-Metric stem (14). The amount of ARMD related to M2a38 or Recap acetabular components at this stage in Finland is low. This is in accordance with Australian findings (11). Our data are the largest series we are aware of concerning M2a38 and Recap LDH MoM THAs. However, it is common that the survival of a new implant worsens after 7 to 10 years due to wear problems (4). Longer follow-up is needed to estimate the true success of the Biomet metal-on-metal bearings.
Survival rates of 98%–99% for follow-ups between 13 and 17 years have been reported for the CLS stem (15, 16). The evidence of the ML-Taper stem is scarce, although excellent long-term results have been published for similar cementless tapered titanium stems (17). According to the current data, ML-Taper stem may perform better with Durom cup than the CLS stem. However, the follow-up time of the Durom/ML-Taper was shorter than that of Durom/CLS. Early fixation failure of the Durom cup with smooth porous coating and Metasul MoM bearing surfaces has been reported (12), although not all the results have been that poor (18). Our findings are consistent with previous poor results due to fixation failure of the Durom cup.
Survival rates of 97% for follow-ups of between 15 and 20 years have been reported for the Corail stem (19). The short-term results of the Summit stem have been satisfactory (20). The short-term results of the ASR cup have been poor due to ARMD, although most of these results are related to hip resurfacing arthroplasty (HRA) (21). Most of the ASR cups (both cementless LDH MoM THAs and HRAs) in Finland have been operated in the Coxa Hospital in Tampere, which is one of the largest hip arthroplasty centers in Europe. Although ASR cups have been implanted by high-volume surgeons in Finland, the outcome has been poor (22). In this study, the short-term survival of the cementless ASR LDH MoM THA using Corail and Summit stems was satisfactory. However, most likely, there will be ARMD problems related to ASR LDH MoM THA surgery as well.
The mid-term survival of the cementless Synergy stem has been 100% for average follow-up of 75 months (23). The results of the BHR cup have been published mainly when using the BHR as a hip resurfacing device. Medium-term survival of the BHR device has been 91%–97% for follow-up of 6–10 years (24–26). In this study, the short-term population-based survival of the BHR/Synergy was comparable to that of the conventional cemented THA.
The most common reason for LDH MoM THA revision in Australia was aseptic loosening followed by infection and dislocation (11). In our study, the most common reason for revision was aseptic loosening of both components (21% of all cases, 42 out of 202 revisions). Furthermore, there were 41 revisions for periprosthetic fracture (20%) and 34 cases of aseptic loosening of the cup only (17%). Totally, 93 out of 202 cementless LDH MoM THA revisions (46%) mentioned in the Finnish register were performed for aseptic loosening. Many of the early problems with aseptic loosening in Finland are due to early instable cups because of technical failures or smooth porous coating. Peri- and postoperative periprosthetic femoral fractures are a major problem when using cementless press-fit stems. Despite this, the revision risk of the best cementless implant (the M2a38/Bi-Metric) was lower than that of the conventional cemented implants. The supposed benefit of cementless fixation is the avoidance of late aseptic loosenings.
There were 11 revisions due to dislocation in the LDH MoM THA group (0.1% of all LDH MoM THAs) and 175 in the THA group (1.0% of all THAs). The relatively high dislocation rate of THA should not be forgotten when comparing different devices.
ARMD is a notorious disadvantage of MoM articulations (9, 10). In the Finnish Arthroplasty Register notification form, these bearing surface complications are not yet asked separately. It is probable that some of these LDH MoM THAs metal bearing complications are coded in the Finnish register as revisions performed for “other reason.” However, there were only eight LDH MoM THA revisions performed for “other reason.” It may be that during the past couple of years, surgeons have not yet been as familiar with this metal bearing problem as today and some of these could have been coded falsely as loosening or malposition. Although the short-term results of LDH MoM THA were comparable to those of conventional cemented THAs, longer follow-up time is needed to detect the true incidence of revisions for ARMD. Register-based analyses are not able to detect early problems of new implants immediately when they start to occur.
Footnotes
Funding
This study was supported by Turku University Hospital EVO project and Sigrid Juselius Foundation.