
Abstract
Background and Aims:
Lumbar spinal stenosis (LSS) is the most frequent indication for back surgery in adults aged over 65 years, but about one-third of operated patients have less than good/excellent results from the operation. Awareness of outcome predictors and their predictive values may help clinicians in their assessment of the prognosis of patients when considering surgical treatment. Our aim was to study the preoperative predictors in LSS for a good postoperative outcome (satisfaction with surgery and functional improvement) with a two-year follow-up.
Material and Methods:
LSS patients (n = 102) completed a questionnaire preoperatively and on two-year follow-up. Preoperative patient-related predictors, self-rated health, comorbidities and preoperative treatment were assessed. Satisfaction with the surgical outcome was assessed with a seven-category scale; satisfaction was determined to be good if the patient response was “condition has considerably improved” or “totally cured”. Other responses (“condition has slightly improved” or worse) represented poorer satisfaction. A good functional outcome was determined as > 30% relative improvement compared to the presurgery score in the Oswestry Disability Index (ODI).
Results:
The predictors for good satisfaction were age < 75 years at operation (OR 4.03; 95% CI 1.35–12.02; p = 0.012) and no previous lumbar operation (OR 3.65; 95% CI 1.13–11.79; p = 0.031). Predictors for a good improvement in the ODI score were regular preoperative analgesic use < 12 months (OR 3.40; 95% CI 1.21–9.53; p = 0.020), non-smoking (OR 3.47; 95% CI 1.09–11.03; p = 0.035) and good (above average) self-rated health (OR 3.27; 95% CI 1.06–10.12; p = 0.039).
Conclusions:
In LSS, regular analgesic treatment preoperatively for 12 months or less, self-rated health above average and non-smoking predicted a good postoperative functional improvement. An age under 75 years and no previous lumbar operation predicted good postoperative satisfaction with the surgery.
INTRODUCTION
Lumbar spinal stenosis (LSS) is the most frequent indication for spinal surgery in the elderly (1), but one-third of operated patients have less than good/excellent results from the operation (2–6). The critical decision on whether and when to consider decompressive surgery requires an understanding of the expected surgical outcome, this being based extensively on radiological stenotic findings accompanied by coherent clinical symptoms. In addition, other preoperative factors also predict the postoperative outcome of spinal surgery (5, 7–10). Awareness of the predictors and their predictive values may help clinicians in their assessment of prognosis of patients when considering surgical treatment. In this study we examined the predictive value of eighteen preoperative factors in LSS with respect to good patient satisfaction with surgery and a good improvement of functional ability two years postoperatively.
MATERIAL AND METHODS
The prospective study included 102 patients with clinically and radiologically defined LSS (9–10). Briefly, selection for surgery was made by the orthopaedist or neurosurgeon at Kuopio University Hospital between October 2001 and October 2004. The inclusion criteria were: 1) presence of back, buttock, and/or lower extremity pain, with radiographic evidence (computed tomography, magnetic resonance imaging (MRI), or rhizography) of compression of the cauda equina and/or exiting nerve roots due to degenerative changes (ligamentum flavum, facet joints, osteophytes and/or disc material) (11–13) and 2) the surgeon's judgement that the patient had clinically significant degenerative LSS as the main diagnosis indicative for operative treatment (11). In addition, all the patients had a history of ineffective responses to conservative treatment. A previous spine operation or co-existing disc herniation was permitted; however, LSS still had to be the main diagnosis for the operation. The exclusion criteria included emergency or urgent spinal operation precluding recruitment and protocol investigations; cognitive impairment prohibiting completion of the questionnaires or other failures in co-operation; and the presence of metallic particles in the body preventing the MRI investigation. The surgeons sent the information about patients eligible for the operation to the Department of Physical and Rehabilitation Medicine (DPRM), which organised the study. The patients received an account of the study during their outpatient visit to the Department of Physical and Rehabilitation Medicine and provided informed consent. The study design was approved by the Ethics Committee of the University of Kuopio and Kuopio University Hospital.
PREDICTORS
Predictors were gathered from responses in the prospectively collected preoperative questionnaire unless otherwise stated. The patient-related predictors were age (years at operation), gender, body mass index (kg/m2), smoking (0 = never, 1 = I have stopped smoking, 2 = yes, occasionally and 3 = yes, regularly); marital status (1 = married, 2 = cohabiting, 3 = single, 4 = widowed and 5 = divorced) and education (1 = secondary or higher degree examination, 0 = lower grade schooling). The self-rated health of the patients was assessed with the question “How would you rate your health at present”? (0 = good, 1 = quite good, 2 = average, 3 = quite poor and 4 = poor), modified from Katz et al. (14). Comorbidity affecting walking ability was assessed using preoperative medical charts of study visits, medical charts of surgeons and the Work Ability Index (WAI; patients reporting musculoskeletal diseases) (15) as a means to detect clear objective disability affecting walking performance, in addition to LSS. Five patients had symptomatic knee arthrosis, two had symptomatic hip arthrosis, one had both knee and hip-arthrosis and two had rheumatoid arthritis. The self-reported number of current or recurring diseases diagnosed by a physician, i.e. number of comorbidities, was assessed using the WAI (15). Diabetes (y/n; type 2) was classified separately from the WAI score.
With respect to preoperative treatment, the question “Have you performed self-acting back exercises?” (yes/no) was included. The frequency of analgesic use was assessed with the question “Have you used analgesics during the last month? (0 = no, 1 = occasionally, 2 = about once a week, 3 = a few times a week, 4 = daily or almost daily and 5 = I use analgesics continually at the maximum doses). The duration of preoperative analgesic use was assessed with the question “How long have you regularly used analgesics for your back problem or radiating pain to the lower extremities?” (0 = no use of analgesics or under one month, 1 = 1–3 months, 2 = 3–6 months, 3 = 6–12 months and 4 = over one year).
In-patient rehabilitation due to back problems and the preoperative use of a supportive belt during the previous year (0 = no, 1 = occasionally, 2 = about once a week, 3 = a few times a week, 4 = daily or almost daily) were evaluated. Previous lumbar operations were recorded retrospectively using medical charts.
The predictors were dichotomised in order to use clinically oriented cut-off limits (Table 1A and 2A). With respect to age, 75 years was chosen as a cut-off (16). In order to calculate the body mass index (BMI), the height and weight were measured preoperatively. A BMI of 30 kg/m2 is considered as the border between slight and moderate obesity (17). With respect to comorbidities, the mean split of the data was used. Concerning the duration of regular preoperative use of analgesics for back and/or leg pain (paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), codeine, tramadol, and/or anticonvulsants), all cut-offs (3, 6 and 12 months) were examined.
Univariate analysis for satisfaction and appearance of preoperative predictors in the postoperative study groups according to the outcome.
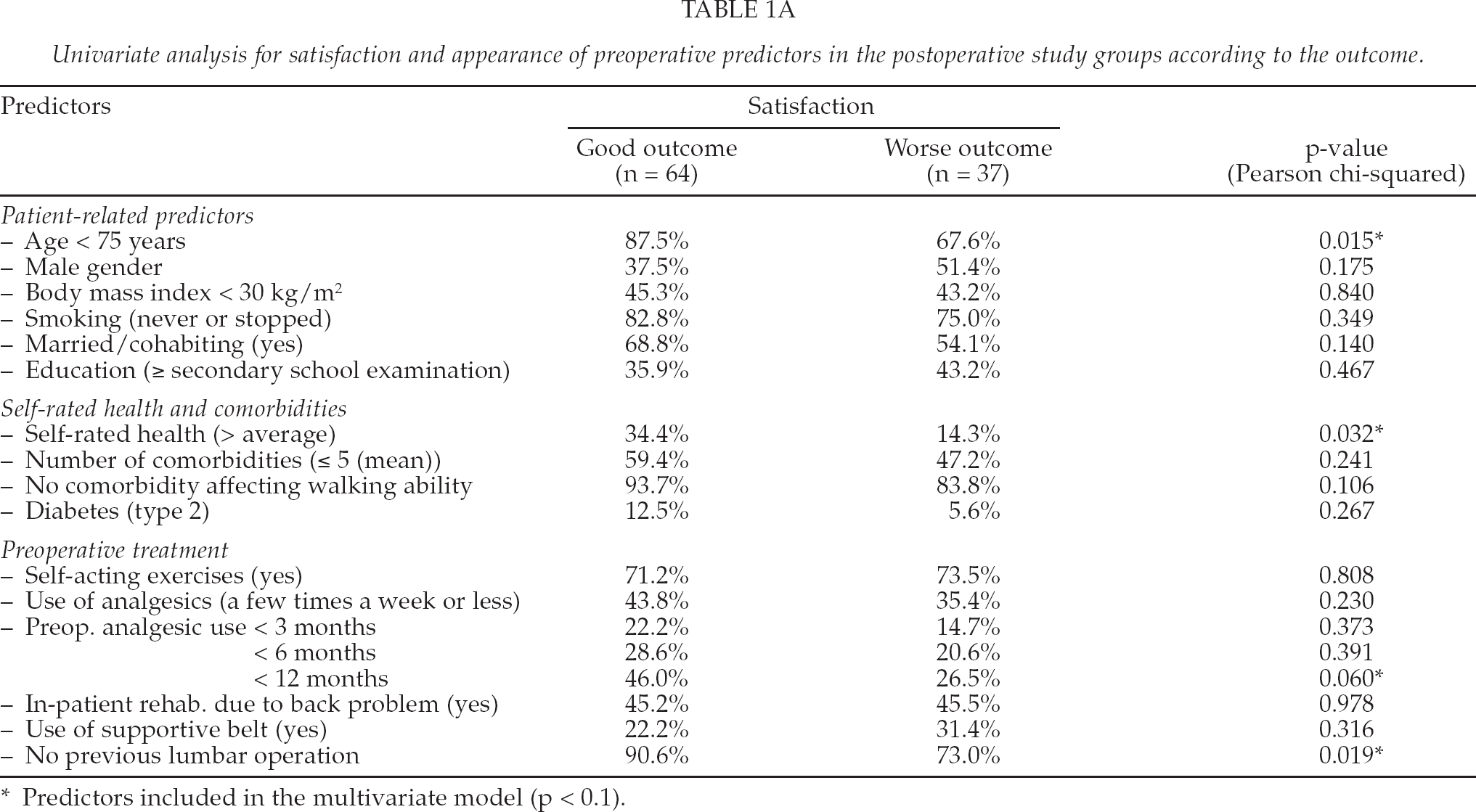
Predictors included in the multivariate model (p < 0.1).
Univariate analysis for the Oswestry Disability Index and appearance of predictors in the postoperative study groups according to the outcome.
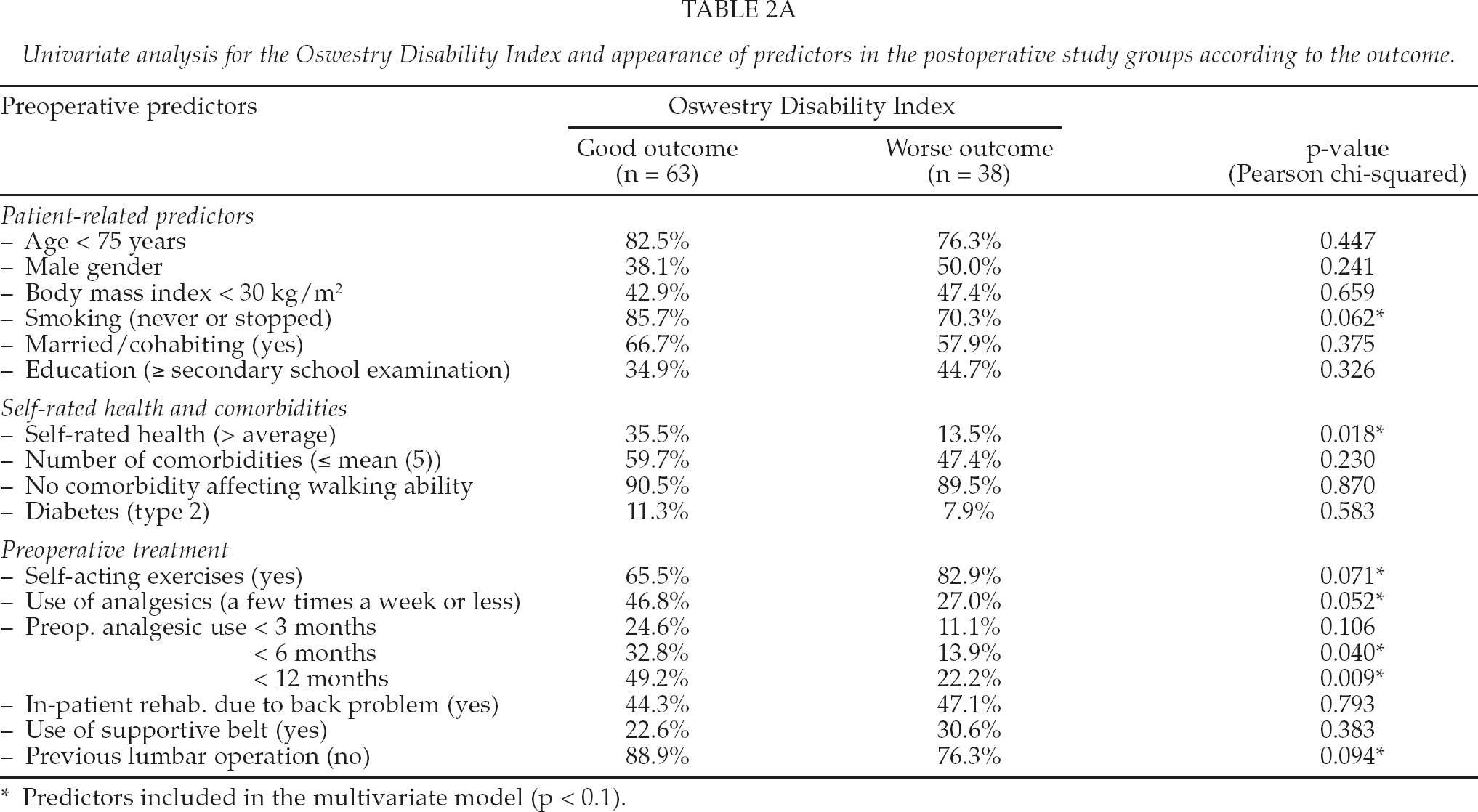
Predictors included in the multivariate model (p < 0.1).
OUTCOME MEASURES AND THE DEFINITION OF A GOOD OUTCOME ON TWO-YEAR FOLLOW-UP
Satisfaction with the surgical outcome was assessed using a seven-category scale as follows: −3 = surgery was a total failure, −2 = condition is now considerably worse, −1 = condition is now slightly worse, 0 = no change, 1 = condition has slightly improved, 2 = condition has considerably improved and 3 = totally cured. With respect to satisfaction, a “good outcome” consisted of those patients who were either “totally cured” or reported “condition considerably improved”, whereas a “worse outcome” consisted of the other responses (10).
A good outcome in the Oswestry Disability Index (ODI, 0–100%) (18–19) was considered as a >30% improvement over the pre-surgery score ((postsurgery score — presurgery score)/presurgery score) × 100%; modified from Mannion et al. (20)).
TREATMENT BEFORE SURGERY
Sixty-eight patients had been provided with self-acting back exercises (any source). For back and/or leg pain, 88 patients had used NSAIDs or paracetamol, 47 tramadol or codeine and 10 patients were prescribed anticonvulsants. Thirty-seven patients used analgesics daily or almost daily, and 24 patients reported continuous use at maximum doses. No strong opioids were used. Sixty patients had used analgesics regularly during the previous 12 months. Forty-four patients had undergone in-patient rehabilitation due to their back problem. A supportive belt had been used by 25 patients during the previous 12 months, and 16 patients had undergone a prior lumbar operation.
SURGICAL TREATMENT
The patients had (on average) severe symptoms due to LSS: preoperatively, the mean ODI was 43.9%, and leg pain on walking and back pain at rest (median; numeric rating scale 0–10; mean during previous week) were rated as 7 and 4, respectively.
All the patients had open or microscopic decompressive surgery of the affected level(s), i.e. laminotomy, hemilaminectomy or laminectomy, with undercutting facetectomy due to lateral (n = 18) or both central and lateral (n = 84) LSS, with a mean dural sac area of 68.6 mm2 at the most stenotic level. In addition to laminar decompression, disc excision was also performed in seven cases (one at level 2–3; one at level 3–4; four at level L4–5 and one at level L5–S1); LSS due other degenerative stenotic changes was also the main diagnosis in these patients. Lumbar fusion, two with instrumentation, was included in the decompression procedure in 19 cases. The indication for additional lumbar fusion was concomitant spondylolisthesis.
STATISTICAL ANALYSIS
Univariate analysis (Pearson chi-squared) was applied to investigate the significance level for each predictor. Following univariate analysis, predictors with a significance level p < 0.1 were included in a binary logistic multivariate model to adjust for intervariable associations. Statistical significance was accepted at the p < 0.05 level, and significant predictors in the multivariate models were considered as the main results. All the patients (n = 102) were evaluated preoperatively. Drop-outs were excluded from the analysis (1 patient). To ensure maximum statistical power, the data from the latest follow-up of four patients who had died before the two-year follow-up were included in the analysis (representing 6–12-month postoperative follow-up data on these patients; data not shown). Thus, the data of 101 patients were finally analysed.
RESULTS
Of the 102 patients, eighty-two (80%) were operated under the age of 75 years. There were 59 females and 43 males. BMI was under 30 in 46 (45%) patients. Twenty patients (20%) smoked either occasionally or regularly. Sixty-five patients (64%) were married or living with a partner. At least secondary-level education was reported in 39 (38%) patients. Self-rated health was good or quite good in 27 (26%) of the 102 patients before the operation. More than five comorbidities were reported by 55 patients (54%). Ten patients (10%) had a comorbidity affecting their walking ability, and eleven patients (11%) had type 2 diabetes.
In 101 patients with follow-up data, good satisfaction with the surgical outcome was reported by 63.4% of the patients (Table 1A). The mean ODI improved from the preoperative level (43.9%) by 17.4 percentage points at the two-year follow-up (p < 0.0001, t-test), and 62.4% achieved a good outcome in the improvement (> 30%) of disability (Table 2A). This corresponded to an 8–56 percentage point improvement in ODI scores in this study population. The distribution of the predictors (data not imputed) in the “good” and “worse” outcome study groups, and univariate analysis are presented in Table 1A (Satisfaction) and Table 2A (ODI).
MULTIVARIATE MODELS (TABLES 1B AND 2B)
Multivariate model: Predictors for good satisfaction with surgery (“total cure” or “condition has considerably improved”).
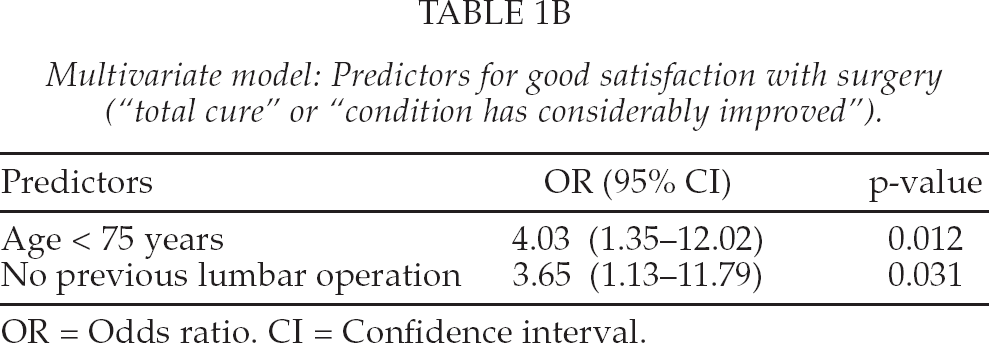
OR = Odds ratio. CI = Confidence interval.
Multivariate model: Predictors for good (> 30%) improvement of ODI.
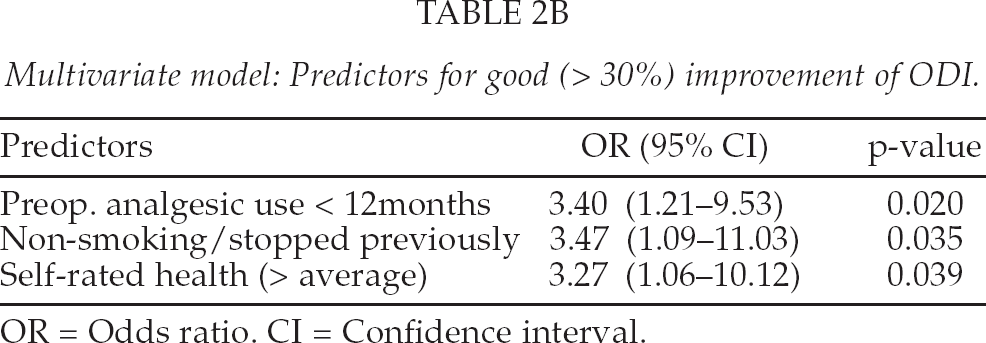
OR = Odds ratio. CI = Confidence interval.
Predictors for good satisfaction were “age < 75 years at operation” (OR 4.03; 95% CI 1.35–12.02; p = 0.012) and “no previous lumbar operation” (OR 3.65; 95% CI 1.13–11.79; p = 0.031). Predictors for good improvement in the ODI were “regular preoperative analgesic use < 12 months” (OR 3.40; 95% CI 1.21–9.53; p = 0.020), “non-smoking” (OR 3.47; 95% CI 1.09–11.03; p = 0.035) and “self-rated health above average” (OR 3.27; 95% CI 1.06–10.12; p = 0.039).
The percentage of “highly satisfied patients” was 69.1% among the patient group < 75 years and 40.0% among the patient group ≥ 75 years. The respective percentages for a good improvement in the ODI were 55.0% and 64.2% (p = ns). The percentage of “highly satisfied patients” was 68.2% among patients without a previous lumbar operation and 37.5% among patients with a previous lumbar operation. The respective percentages for a good improvement in the ODI were 65.9% and 43.8% (p = ns). The percentage of patients reporting a good improvement in the ODI was 78.9% among the patient group “regular preoperative analgesic use < 12 months” and 52.5% for the group “regular preoperative analgesic use ≥ 12 months”. The respective percentages of “highly satisfied patients” were 76.3% and 57.6% (p = ns). The percentage of patients reporting a good improvement in the ODI was 67.5% among non-smokers and 45.0% among smokers. The respective percentages for “highly satisfied patients” were 66.3% and 55.0% (p = ns). The percentage of patients reporting a good improvement in the ODI was 81.5% in the patient group SRH > average and 55.6% in the patient group SRH ≤ average. The respective percentages of “highly satisfied patients” were 81.5% and 58.3% (p = ns).
DISCUSSION
In this prospective, observational study with a two-year follow-up, the outcome was evaluated with two specific outcome measures in LSS surgery, i.e. patient satisfaction and the validated ODI score. The definition of a good outcome included at least a 30% relative improvement in the ODI, or patient satisfaction indicated by the reporting of “totally cured” or “condition has considerably improved”. We used rigorous categorisation of “satisfaction with surgery” in order to identify the patients who were truly satisfied with the results of the surgery. In addition, the predictors had clear cut-off values.
As far as we know, this is the first time that a previous lumbar operation (PLO) has been demonstrated to have significant predictive value for worse satisfaction in a prospective study consisting of only LSS patients (5, 7). Of those 16 patients who had undergone a previous operation, 6 patients were truly satisfied (“condition has considerably improved” or “totally cured”), and of the 10 less satisfied patients, 9 reported “condition has slightly improved” and only one patient reported “no change”. Nevertheless, 15/16 patients had at least “slight improvement”, and thus patients with a prior operation still have a fair possibility of benefiting from an operation. An age of 75 years or over predicted worse patient satisfaction. However, increased age did not predict a worse outcome in the ODI.
To optimise postoperative satisfaction in LSS, these results highlight the need for careful preoperative discussion concerning realistic expectations and the goal of the operation, particularly among elderly patients, and also with patients who have previously undergone a lumbar operation. These results are in line with the study of Jakola et al., in which a decompressive LSS operation was determined to be safe for patients aged over 70 years, and a clinically meaningful improvement in functional status and also the quality of life can be expected (21). Ishii et al (22) reported inferior results after cervical laminoplasty among patients 75 years or above, compared to younger age groups. We tested also other cut-offs (60, 65 and 70 years) which indicated however no predictive value. We thus recommend that the cut-off age of 75 years should be interpreted with caution and confirmed in further LSS studies.
Smoking has been found to be a negative predictor for the outcome following lumbar disc herniation surgery (7), lumbar fusion (23–24), and also in the latest large register study (n = 4555) in LSS including the ODI and overall satisfaction as outcome measures, in which smokers also tended to use more analgesics before the operation and two years postoperatively (25). Our finding was that non-smoking individuals, including patients who have stopped smoking before surgery, have an odds ratio of over three for having a good functional improvement (ODI) following surgery. Our multivariate model also included the preoperative use of analgesics. As only three of the fused patients were smokers, the effect of nicotine on the revascularisation of the bone grafts (26) did not explain the poorer results for smokers in our population. Despite the ultimate mechanism of effect of tobacco, this study strengthens the belief that smoking also has a harmful effect among surgically treated LSS patients.
Self-rated health (SRH) predicted a good improvement in the ODI score. In LSS surgery, better (excellent/good) SRH has been reported as a predictor of a better outcome (satisfaction, symptoms and walking ability) by Katz et al. (14). Instead of a four-item scale (excellent/good/fair/poor), we used a modified five-scale instrument, comparing patients with “good” or “quite good” SRH to the “average/quite poor/poor” SRH group. In the univariate analysis, an association with satisfaction was also noted (Table 1A). It has been suggested that the independent effect of self-assessed health might result from the respondents' personal knowledge of current morbidity, incipient health problems, or other factors that influence the outcomes (27).
For the first time in LSS, a clear cut-off value was found in the preoperative duration of regular analgesic use, i.e. analgesic use for 12 months or less predicted a good improvement in disability compared to patients with regular analgesic use of over 12 months. Our result is supported by the findings of Lawrence et al., according to which preoperative narcotic use for over six months on a daily basis predicted a worse outcome after cervical decompression and arthrodesis for radicular pain, with a minimum two-year follow-up (28). This finding may be useful when considering the timing of the operation. Longer preoperative symptoms have been reported to predict a worse outcome in lateral stenosis, but with no threshold value (29). We did not enquire about the duration of preoperative symptoms, but this duration of preoperative symptoms is likely to be longer than the duration of regular consumption of analgesics. Thus, regular consumption of analgesics may possibly be a better potential predictor, since it may reflect the presence of persistent and severe symptoms warranting operative decompression within a reasonable time window in order to prevent irreversible neural damage. However, before stronger recommendations for LSS treatment guidelines can be made, further studies are needed to confirm this 12-month time period.
The regular preoperative consumption of analgesics in central stenosis has been reported to be associated with greater postoperative pain (29). The frequency of use of analgesics in our study remained at the non-significant level.
LIMITATIONS
Our study population was relatively small. We defined this study to present preoperative patient characteristics, preoperative treatment, self-rated health and comorbidities, excluding peroperative factors. Some predictors had a low prevalence in this population (diabetes, comorbidity affecting walking ability), diminishing the statistical power when comparing these subgroups to the other subjects. It is therefore possible that some predictors in this study with non-significant results (predictive value) could have achieved a significant predictive value with a larger study population. With respect to the outcome measures, we only examined the predictors for good satisfaction with surgery and a good improvement in disability. These shortcomings, however, do not diminish the predictive value of the identified significant predictors in LSS. The present study may help clinicians in their assessment of the prognosis of patients when considering surgical treatment. However, prognostic studies are not designed to answer the question of what is the indication for surgery.
CONCLUSION
Regular analgesic use for 12 months or less preoperatively, better self-rated health (above average) and non-smoking predicted a good postoperative functional improvement. Age < 75 years and no previous lumbar operation both predicted good postoperative satisfaction with surgery.
Footnotes
ACKNOWLEDGEMENTS
We thank Vesa Kiviniemi for the statistical advice.
This study was supported by a Kuopio University Hospital EVO grant and a research grant from the Finnish Cultural Foundation (Hulda Tossavainen Foundation 2003; Aili and Leo Davidsson Foundation 2009, St. Michel Central Hospital 200-year Fund 2010, and the Kaisu and Urho Kiukas Foundation 2011).