
Abstract
This paper provides a summary of up-to-date information and experience with the combined treatment of patients suffering from peripheral arterial disease (PAD) with endovascular and open surgery, performed simultaneously and in a single operating room. Hybrid intervention is reported to have good results in well-indicated groups of patients with acute and chronic limb ischemia, even with older, high-risk patients. The indications for the use of this technique remain unclear with inconsistent opinions among vascular surgeons. The indications for treatment were divided into three main groups: 1) Patients with chronic limb ischemia, 2) acute limb ischemia, and 3) occlusion of a previous vascular reconstruction. The operating techniques for the most commonly used combinations are described.
In conclusion, hybrid operating techniques are often useful when treating complex problems and multilevel disease in patients with chronic or acute lower limb ischemia. Modern vascular surgeons need to master both open and endovascular techniques, and to combine them in a creative fashion to the benefit of our patients.
Keywords
INTRODUCTION
The development of endovascular techniques dates back to the 1970s, when Dotter modified Gruntzig's technique of percutaneous artery dilation and introduced percutaneous intervention to routine clinical practice (1). During recent decades, endovascular procedures have partly replaced open surgery for many indications in the treatment of peripheral arterial disease (PAD). Although the number of patients treated purely with the endovascular procedure has grown, there is a significant number of patients that require a combined (hybrid) approach using both techniques, preferably in one session. This hybrid procedure allows complete revascularization of peripheral arteries in patients with significant co-morbidities and complex multilevel arterial repair (2). The first reported hybrid procedure in the literature dates back to 1973, when dilation of pelvic arteries was performed along with femoro-femoral bypass (3). Currently, hybrid procedures are reported to consist of 5 to 21% of the total number of vascular reconstructions (4). The aim of this paper is to define the indications, technique and benefits for one-session hybrid intervention, based on a literature review of recently published studies.
INDICATIONS FOR HYBRID INTERVENTION
CHRONIC LIMB ISCHEMIA
Chronic limb ischemia presents as critical limb ischemia (CLI) or intermittent claudication. Critical limb ischemia is a manifestation of peripheral arterial disease that describes patients with chronic ischemic rest pain, foot and leg ulcers or gangrene and is associated with multilevel lesions, affecting the inflow and outflow tracts (5). Relief from rest pain and the healing of the ulcers or gangrene often requires complete revascularization of all affected levels by either open surgery, an endovascular procedure or their combination, resulting in renewed blood flow to the pedal circulation (5). The revascularization of one level alone is often insufficient and seldom leads to the healing of ischemic ulcers (6). Endovascular interventions should be preferred for the elderly, high risk patients with life expectancy of less than two years (7). In addition to patients who could benefit from either type of intervention as part of CLI therapy, there is a significant group of patients for whom sole endovascular or open surgery is technically unfeasible or for no benefit is predicted from either technique. In practice we often encounter situations where it is difficult to proceed with angioplasty only due to simultaneous calcifications and stenosis of the inflow arteries (usually the CFA and/or iliac arteries), even when a cross-over strategy is applied. This makes it difficult to safely access the artery with endovascular instruments and increases the risk of re-occlusion. The incidence of re-stenosis after iliac angioplasty combined with infrainguinal reconstruction has also been reported by several authors as being lower (8,9). The hybrid procedures offer a solution for vascular lesions, where endovascular treatment may be used for in-flow or out-flow lesions, in combination with open surgery during a single session.
The most common combinations are iliac artery angioplasty with infrainguinal reconstruction (endarterectomy of the common femoral artery (CFA) or infrainguinal bypass), infrainguinal reconstruction (above-knee bypass) with infrapopliteal angioplasty or a combination of superficial femoral artery (SFA) angioplasty with popliteo-crural/pedal bypass (2). The treatment of chronic limb ischemia with hybrid procedures is associated with high technical success, good primary, primary-assisted and secondary patency, limb salvage and cost effectiveness, thus combining the advantages of both techniques. The largest study was published by Madera in 1997, and included balloon angioplasties performed on 336 vascular segments as a part of 239 lower extremity revascularization procedures in 200 patients (10).
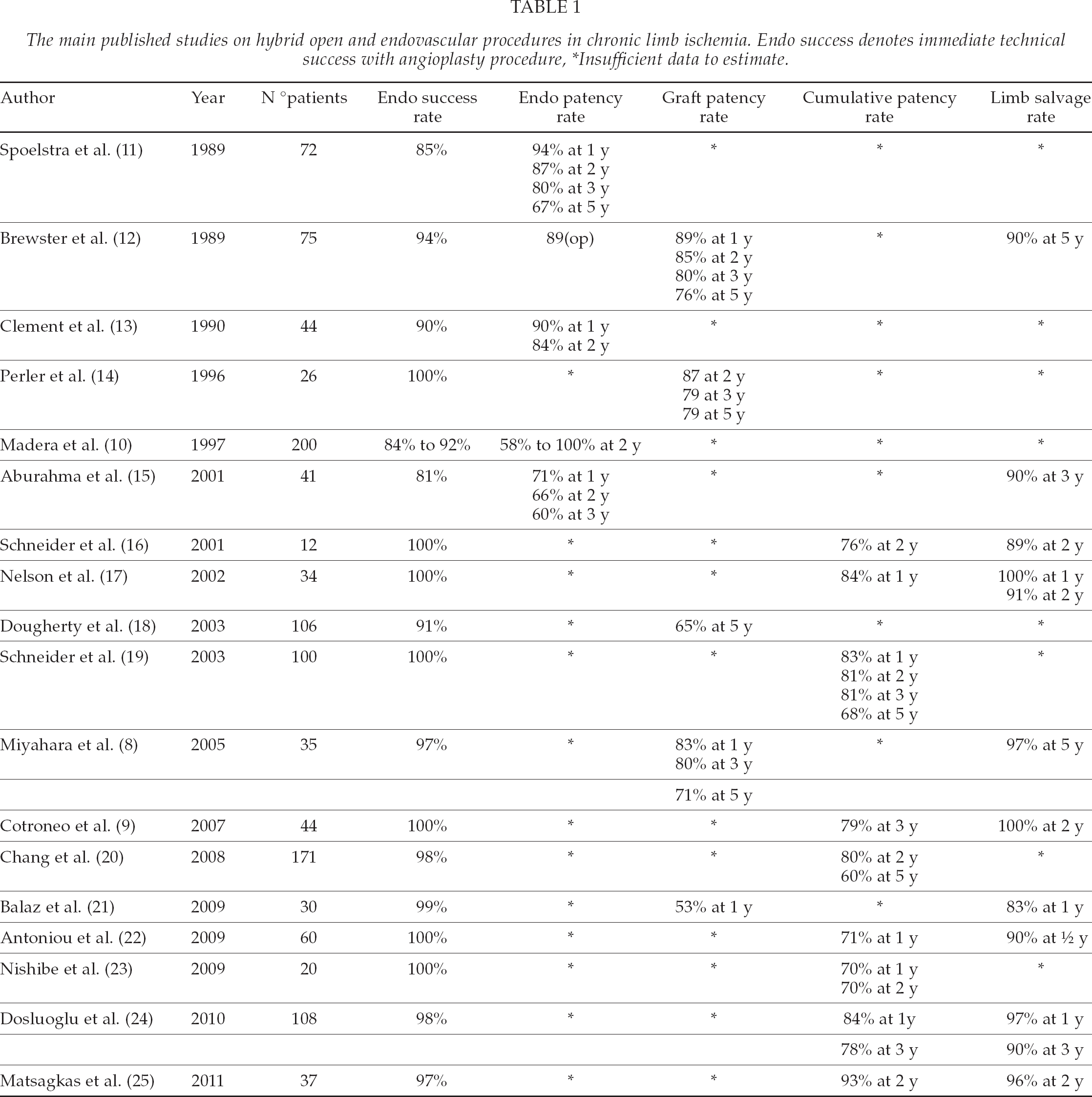
Largest published reports including hybrid open and endovascular procedures are listed in Table 1.
The main published studies on hybrid open and endovascular procedures in chronic limb ischemia. Endo success denotes immediate technical success with angioplasty procedure, *Insufficient data to estimate.
ACUTE LIMB ISCHEMIA (ALI)
ALI is a limb-threatening condition caused by embolization, in situ arterial thrombosis, or acute graft occlusion. The acute risk of limb loss ranges from 5–30%, and mortality from 11–18% (26). The main therapeutic options are: Endovascular (thrombolysis/aspiration), surgical revascularization (thromboembolectomy) or conservative treatment (heparinization, vasodilatators). The choice of therapy depends on the duration and degree of ischemia and the overall condition of the patient, as suggested by the Rutherford classification (27). Hybrid interventions can be offered to patients in whom angiography after surgical thromboembolectomy unmasks lesions in inflow or outflow tracts. Angiographic findings can reveal stenosis, occlusion, dissection, aneurysm of the inflow/outflow tracts or residual thrombus which can be treated with concomitant endovascular procedure, including balloon angioplasty, stenting and thromboaspiration (type I of hybrid procedure in ALI) (28). Zaraca et al. (29) recently reported their experience with intraoperative angiography in 380 thromboembolectomies for ALI over a 12-year period. In this group of patients angioplasty was performed in 24.4% of patients. They noted that the routine use of intraoperative angiography resulted in a higher rate of reintervention due to residual lesions resulting in lower re-occlusion rates at 24 months. Antoniou et al. (22) analyzed retrospectively data in 60 patients who underwent 61 single-step hybrid procedures. In six patients (10%) the indication for arterial reconstruction was acute limb ischemia. In this subgroup, technical success was achieved in all patients (100%) and only one amputation was performed on the seventh postoperative day due to progression of ischemia after unsuccessful revascularization.
When surgical thromboembolectomy is insufficient and the thrombus persists, the combination of surgical techniques with thrombolysis prior to or after surgery (type II of hybrid procedure in ALI), or the combination of endovascular techniques local thrombolysis (type III of hybrid procedure in ALI) can be used (28). Intraoperative fibrinolytic therapy has recently been recommended as an important alternative to mechanical thromboembolectomy to remove residual thrombus. In the prospective study by Fajardo et al. (30), the aim was to determine the value of intra-arterial thrombolysis in 66 patients with ALI as an adjunct to mechanical thromboembolectomy. Two groups of patients were compared: one (n = 35) in which mechanical thromboembolectomy was applied as the single technique and another (n = 31) in which urokinase was instilled at the end of the thromboembolectomy. Intraoperative arteriography showed residual thrombus in 30.3% of the patients and unsuspected arterial lesions in 34.8%. Recurrence of thrombosis was significantly associated with the presence of a residual thrombus followed by amputation and the use of thrombolysis showed to be statistically significant in reducing thrombotic recurrence in patient with ALI.
In the study by Beard et al. intraoperative thrombolysis was attempted in 31 acutely ischemic legs after operative arteriography. Complete lysis was achieved in 11 cases (35%) and partial lysis in 12 (39%) (31). The aim of the study by Witz et al. (32) was to evaluate the use of intraoperative intra-arterial urokinase infusion after thromboembolectomy in 21 patients with acute lower limb ischemia. Angiography demonstrated complete and partial lysis in 14 and three patients respectively and limb salvage was sustained in 17 patients with successful angiographic lysis. The importance and safety of intraoperative intra-arterial thrombolysis after mechanical thromboembolectomy in the treatment of ALI has already been confirmed with good short- and long-term results (33).
OCCLUSION OF THE VASCULAR RECONSTRUCTION
Graft occlusion within one month of surgery (early occlusion) is most commonly due to technical error, and an early surgical revision is recommended (34). Occlusion between 30 days-18 months postoperatively is usually caused by neo-intimal hyperplasia (NIH) in the distal anastomosis. Graft closure after 18 months (late) is mainly due to the progression of atherosclerosis affecting the inflow or outflow tracts (34). In the mid- and late type of occlusion, we have two options for intervention that are dictated by the patient's condition and symptoms: surgical thrombectomy or direct catheter thrombolysis (CT). The results of both methods with occluded venous grafts are not satisfactory. Only 19–28% of occluded venous grafts that underwent thrombectomy were patent after five-years (35, 36). In a study by Nackam et al. (37) the rate of primary patency after thrombolysis of venous bypass at 12 and 24 months was 25% and 19%, respectively. Given the negative results of both methods in the case of venous graft occlusion, a new vascular reconstruction is recommended by some authors (34).
The recanalization of an occluded prosthetic bypass can be achieved by surgical thrombectomy with or without revision of the anastomosis, percutaneous thrombolysis with or without angioplasty, or by a new bypass. A simple surgical thrombectomy can rapidly clear the graft, but without solving the underlying cause of the occlusion, only a temporary effect is achieved (38,39). Surgical thrombectomy of prosthetic bypass with intraoperative angioplasty is an alternative method to surgical and endovascular treatments alone. In this method, which is minimally invasive and can be performed under local anesthesia, the risks of thrombolytic therapy are thus eliminated we can achieve rapid clot removal from the prosthesis, treat the possible stenosis by angioplasty and finally correct the in-and outflow of the involved vascular network, if necessary. In the study by Costanza (40), patients with occlusion of the prosthetic femoropopliteal above-knee bypass were treated with surgical thrombectomy and balloon angioplasty. Patients were categorized into two groups on the basis of time elapsed from initial bypass graft construction to graft failure. Group 1 (n = 21) consisted of patients with femoropopliteal graft failure < 2 years after revascularization and group 2 (n = 9) consisted of patients with femoropopliteal graft failure > 2 years after revascularization. Significant differences in 6- and 12-month patencies between the two groups were reported. In group 1, the patencies at 6 and 12 months were 15.3% and 5.1%; respectively. In group 2, the corresponding patencies were 58.3% and 38.8%. Treatment with surgical thrombectomy and balloon angioplasty achieves significantly greater short-term patency among patients with late (> 2 years) bypass graft failure and may be an alternative for patients who cannot tolerate a complete reoperation, or who lack autogenous conduit. These results are consistent with the work of Nackmana (37) and Hye (41), who reported that early infrainguinal bypass graft failures (< 1 year) had a significantly shorter patency after graft salvage than grafts that had been functional for more than one year. The cause of the failure can be explained by the high resistance of peri-anastomotic stenosis of the distal anastomosis to balloon dilation (42). The combination of surgical thrombectomy with intraoperative angioplasty could be the method of choice for patients who cannot tolerate reoperation, lack suitable autologous material for a new revascularization and need urgent revascularization for limb salvage due to ALI.
The investigation of Aburahma et al. report that, thrombectomy/open surgical repair was superior to lysis/PTA (or thrombectomy/balloon angioplasty) for the treatment of failed above-knee PTFE femoropopliteal grafts with anastomotic stenosis (43). Similar results were published in a not randomized study by Bull et al. (39). Authors compared the effect of percutaneous angioplasty with open bypass (an annual patency of 31% vs. 60%). One of the advantages of the hybrid techniques is that the underlying cause can be dealt with at the time of primary revascularization. Despite excellent immediate results, thrombolysis alone results in limited long-term patency of the occluded graft. Several studies have confirmed that no more than 50% of these grafts are viable at one year (39, 44, 45).
THE ONE-TIME HYBRID INTERVENTION TECHNIQUE
The hybrid procedure can be performed in three different types of operating theaters or environments. The first is the interventional radiology suite, which is fully equipped for endovascular procedures, including excellent imaging tools and a broad portfolio of materials. However, it is not ideal for open surgery.
The second option, an operating room (OR), is ideal for open revascularization but is usually equipped with only a mobile × ray C-arm and a basic CAT laboratory. These shortcomings can be reduced due to recent technological developments. The modern C-arm already possesses the capability for digital subtract angiography with high resolution, which allows for road mapping, data backup, etc. The sterility, illumination and handling of the operating table are the advantages of an OR. It may be equipped with an X-ray-transparent operating table and an automatic injector for contrast agents. Although the image quality will never be the same as it is in the intervention suite, it is still preferable to perform hybrid surgery in an operating room in most cases.
The third and ideal solution is a special hybrid operating theater that combines the advantages of the two previous options, but at a greater cost.
The actual procedure almost always requires access to one or both of the femoral bifurcations. The femoral bifurcation is also the most common site for the proximal/distal bypass anastomosis and the place where thromboembolectomy is usually begun. An exception is the SFA angioplasty or the popliteal artery (PA), which is utilized during popliteo-crural bypass. The access point for retrograde angioplasty is part of the PA, where the proximal anastomosis is placed afterwards (46). Most centers perform angioplasty first, and the site of puncture is used for bypass anastomosis or endarterectomy (2, 19, 47). The opposite approach, also respected (48) and used in our clinics, is to start with open surgery. The guide-wire is then inserted to the proximal anastomosis of the graft, and the procedure is completed by angioplasty (21). The advantage of this procedure is that it allows verification of the patency of the reconstruction without further puncture. The disadvantage is that when angioplasty is performed, the inflow to the reconstruction is temporarily occluded and at risk of thrombosis. We can decrease this risk with adequate and monitored heparinization throughout the procedure. The 7Fr sheath is most often used for aortic and pelvic angioplasty, which allows for the introduction of a wide-range of balloons and stents. Suture of the puncture hole after its extraction does not usually cause problems. After diagnostic angiography, balloon dilation is performed when indicated. The indications for stent implantation depend on the anatomical location and technical issues, such as recoiling (Fig. 1). It should be emphasized that there are no randomized or other robust data to answer the important question which strategy is best, first open or first endovascular.
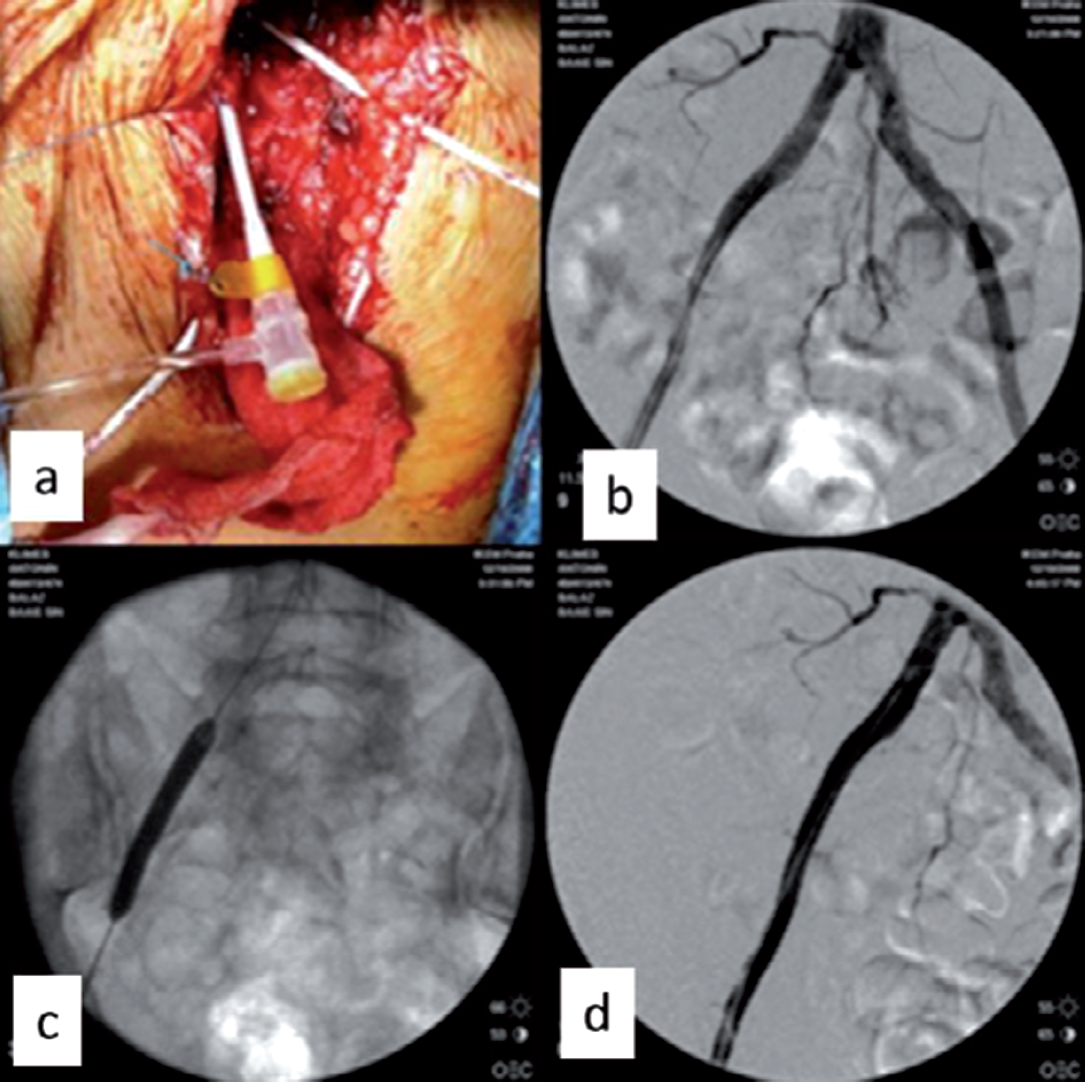
a) 7Fr sheath in the CFA after endarterectomy, b) stenosis of the external iliac artery, c) balloon dilation of the external iliac artery, d) state after angioplasty without stenting.
Last but not least, is important to note that the performance of hybrid procedures on the same day, if possible, significantly decreases the length of hospital stay and reduce the costs, in comparison with the two-staged hybrid approach (4). Besides, the increasing understanding and experience of vascular surgeons with endovascular techniques and equipment has allowed them to incorporate these into endovascular surgery more frequently (2).
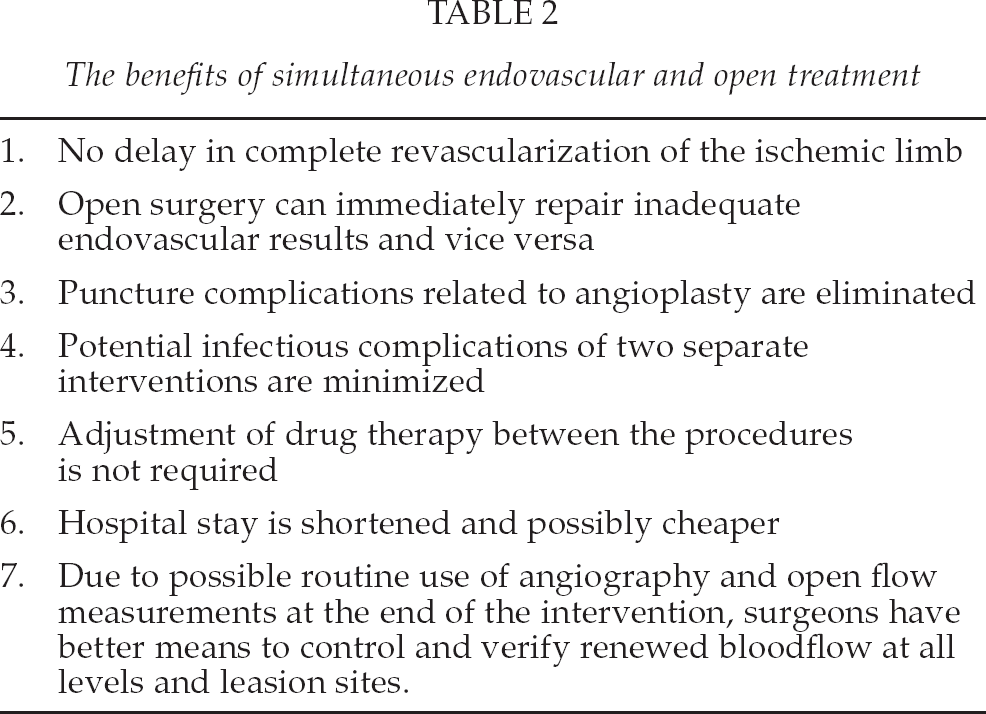
The benefits of simultaneous endovascular and open treatment are summarized in Table 2.
The benefits of simultaneous endovascular and open treatment
CONCLUSION
In conclusion, hybrid operating techniques are often useful when treating complex problems and multilevel disease in patients with chronic or acute lower limb ischemia. Modern vascular surgeons need to master both open and endovascular techniques, and combine them in a creative fashion, to the benefit of our patients.