
Abstract
In hybrid reconstructions, patients are treated using both endovascular and open revascularization techniques simultaneously. In recent years, these multilevel reconstructions have been increasingly used especially by vascular surgeons as they have adopted new knowledge and endovascular skills and the endovascular techniques have evolved. The first reports of combined endovascular and open surgical procedures are from the 1970s. Since then, most reports have dealt with femoral endarterectomy or femoro-femoral bypass combined with inflow iliac percutaneous transluminal angioplasty (PTA) and stenting. Primary success rates have been high: 93%–100%. In our institution 213 hybrid procedures were performed during 2003–2011 with 98.6% technical success rate. The annual number of hybrid procedures ranged from 4 in 2004 to 73 in 2011. Inflow endovascular procedure was performed in 60% and outflow in 40 % of the cases. The proportion of the endovascular component performed by vascular surgeons increased from 0% in 2004 to 86.3% in 2011.
In the current report we review the results published in the literature, report our own experience and present some technical notes and cases.
Keywords
INTRODUCTION
In hybrid reconstructions, patients are treated using both endovascular and open revascularization techniques simultaneously, most often at different levels. In recent years, these multilevel reconstructions have been used increasingly often, especially by vascular surgeons as they master both endovascular and open surgical skills, and as the endovascular techniques as such have evolved. Hybrid procedures offer a less invasive approach for patients with multiple co-morbidities and have recently been preferred whenever possible. Lower morbidity and mortality, as well as reduced stay in both hospital and intensive care are advantages with these minimally invasive techniques (1, 2).
In the current review, we analyse the reports published on hybrid procedures in the literature, in addition to providing a retrospective analysis of the treatment methods used on chronic limb ischaemia patients during 2003–2011 at Helsinki University Central Hospital (HUCH), a tertiary referral centre in southern Finland. Furthermore, treatment modality trends, procedure details, the roles of the interventional radiologist and the vascular surgeon, as well as the short-term results of hybrid procedures are further analysed.
REVIEW OF THE LITERATURE
The first reports of combined endovascular and open surgical procedures are from the 1970s (3). Since then, most reports have dealt with femoral endarterectomy or femoro-femoral bypass combined with inflow iliac PTA and stenting. Primary success rates have been high: 93%–100% (2, 4 –6). The long-term results in such inflow endovascular procedures have been shown to be comparable to those of open surgical procedures, with lower or equal morbidity and mortality rates and with primary patency rates of 60%–91% (1, 2, 4, 5, 7). Piazza et al. also discovered that major tissue loss was a negative predictor for patency (1). In some reports morbidity has been higher in hybrid procedures as compared to sole endovascular procedures, possibly due to the patient having a more generalized atherosclerosis (2). Yet there are no randomised studies involving comparisons between hybrid and open procedures. Such studies may be very difficult to conduct due to the complexity of and variations in the outflow and inflow anatomy of these patients with multilevel disease and various clinical presentations. Reports of combined procedures with the endovascular outflow component have been especially scarce.
The proportion of hybrid procedures among all revascularizations has increased steadily during the last decade and is estimated to constitute some 5%–20% of all reconstructions (2, 8).
Technical aspects regarding target vessel recanalization, wire and catheter placement, stent placement and the timing or order of an endovascular and open procedure usually involve femoral endarterectomy and patching with iliac stenting. Most reports favour pre-arteriotomy guidewire placement, followed by femoral endarterectomy and iliac balloon angioplasty and stenting (2, 4, 5). The stent materials and brands used vary in all of the reports and reflect the complex and versatile nature of vascular disease. Chang et al. found that in iliac disease the use of covered stents yielded better results than bare stents when combined with common femoral endarterectomy (primary patency 87% versus 53%; (4).
OUR OWN EXPERIENCE
All hybrid procedures performed at our institution due to chronic lower limb ischaemia during the review period were searched using the vascular surgical registry and cross-checking against a registry containing all angioradiologic procedures in HUCH. In total, 9800 procedures were performed during this period: 4000 open repairs, including 213 hybrid procedures and 5800 endovascular procedures. The annual number of hybrid procedures ranged from 4 in 2004 to 73 in 2011 and the proportion of hybrid procedures among all open revascularizations for chronic limb ischemia increased from 3% to 22% (Fig. 1). The technical success rate was 98.6%. Out of all these procedures, 70.4% (n = 150) were performed due to critical limb ischaemia (31.3% due to rest pain and 39.1% due to tissue loss), 28.2% (n = 60) due to claudication and 1.9% (n = 4) for other indications. Almost 40% of the cases were emergencies (32.1%) or urgent (5.0%), 62.9% being elective procedures.
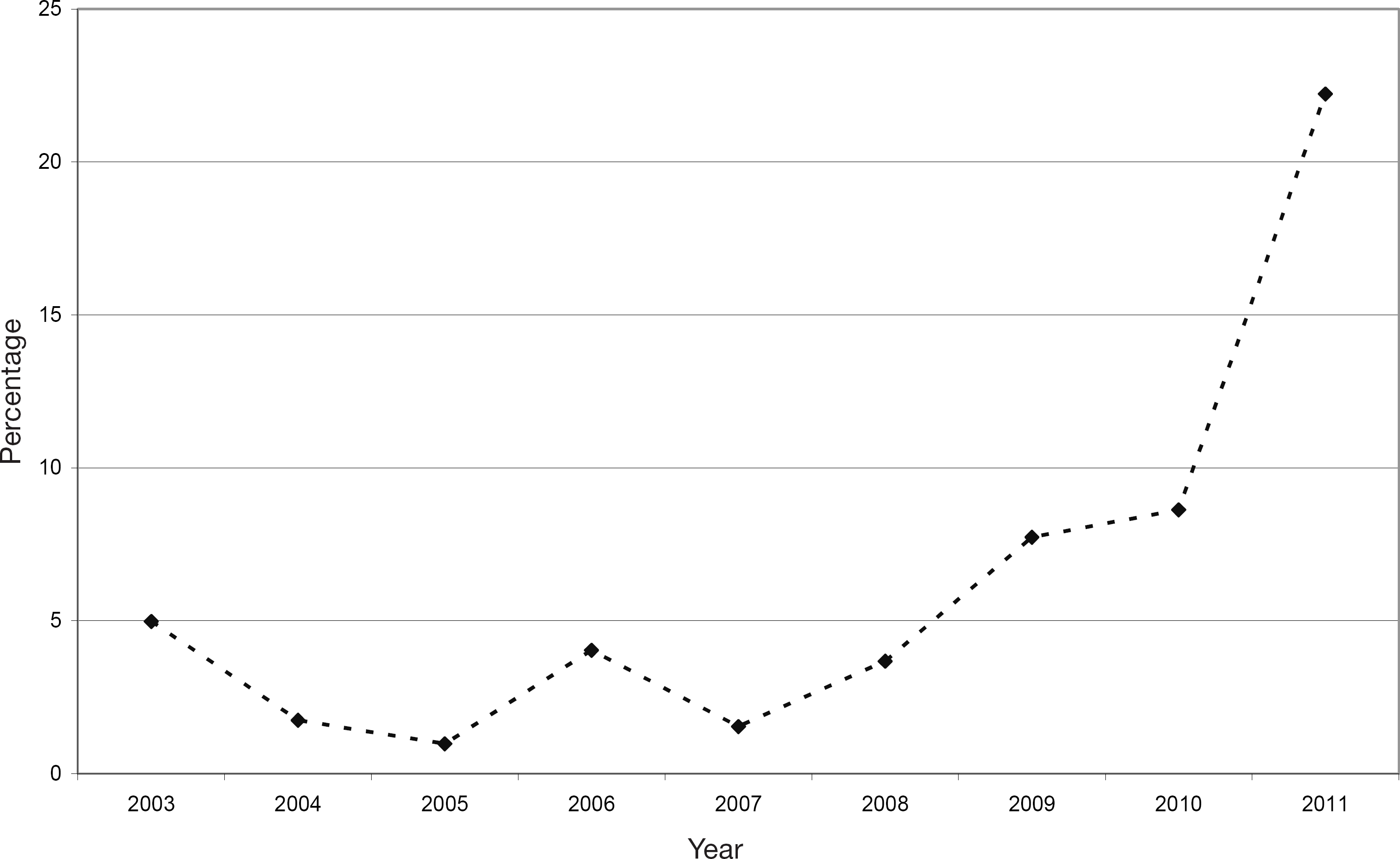
The proportion of hybrid procedures from all open procedures for chronic limb ischaemia during 2003–2011.
In three patients the endovascular procedure was unsuccessful. These patients were treated in 2003, 2008 and 2011. They were excluded from further analysis.
In most of the hybrid procedures (n = 127, 60.5%), inflow was treated with an endovascular procedure, which was combined with a femoral procedure in the groin only (38.6%) or with a bypass (61.4%). In 73 cases (34.8%), outflow PTA was performed, 78.1% of which constituted an outflow PTA distal to a femoral procedure in the groin and 21.9% an outflow PTA of the vessels distal to the bypass. For ten patients (4.8%), both inflow and outflow PTA was performed together with an open surgical revascularization.
The mean duration of the operation for all hybrid procedures was 211 minutes (SD 82 minutes, range 67–540 minutes). It was longest in procedures where an inflow PTA (+/– stenting) and distal bypass were combined (279 minutes, SD 88 minutes, range 115–540 minutes) and shortest in those where a femoral procedure in the groin was combined with an outflow PTA (+/– stenting). The mean blood loss was 832 ml (SD 744 ml, range 50–3,800 ml), being highest where inflow PTA (+/– stenting) was combined with bypass and lowest in femoral procedures combined with outflow PTA (+/– stenting) (686 ml, SD 601 ml, range 100–3.300 ml).
The number of hybrid procedures increased steadily during the 9-year period, but the proportion of inflow and outflow endovascular procedures did not change significantly (Fig. 2). The role of the vascular surgeon in the endovascular procedure increased significantly from 0% in 2004 to 86.3% in 2011 (Fig. 3). Three patients died and one underwent major amputation within 30 days of the procedure (1.9%).
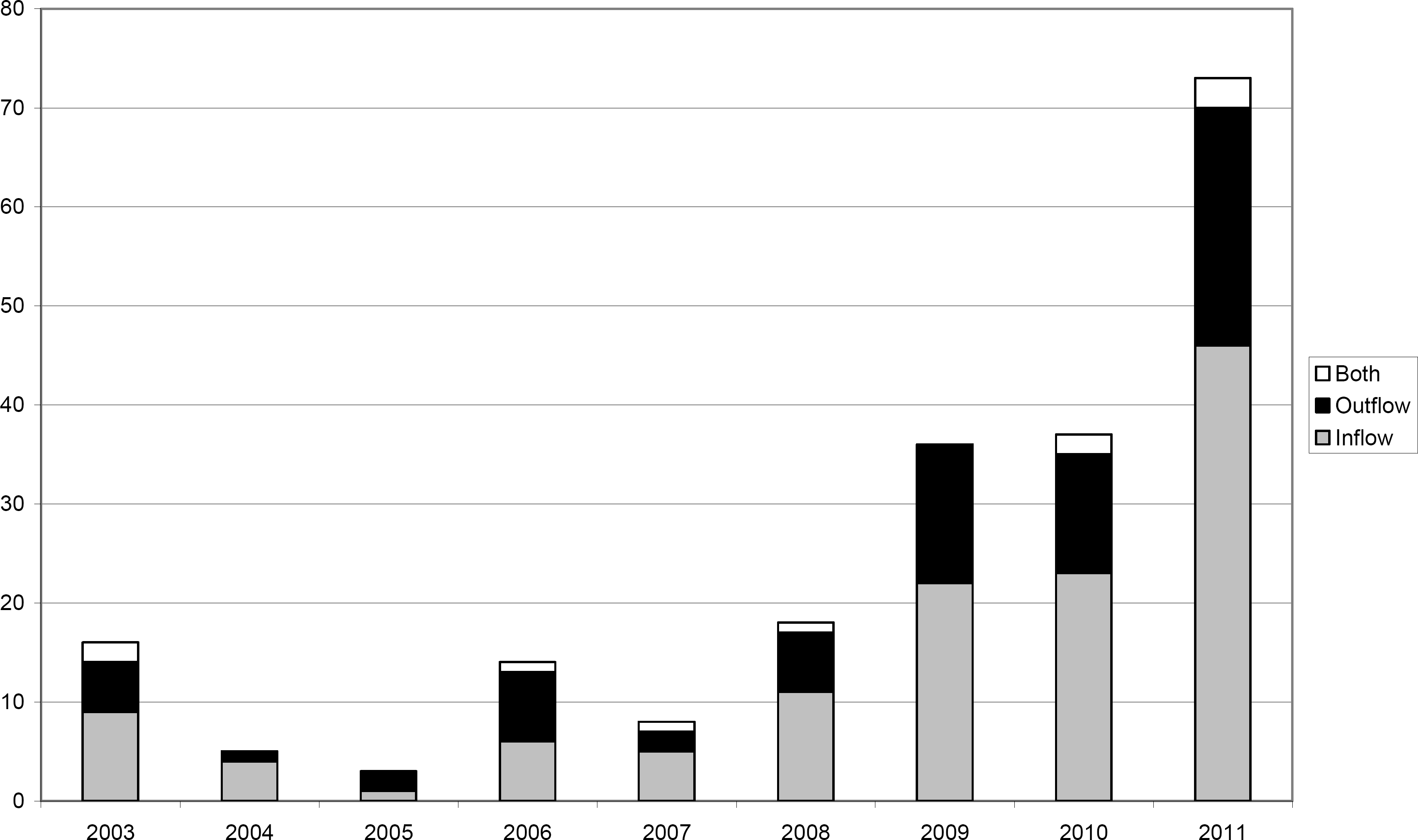
The number of hybrid procedures in 2003–2011 divided into three categories: open surgical revascularization combined with endovascular inflow procedure (grey), outflow procedure (black) and both inflow and outflow procedure (white).
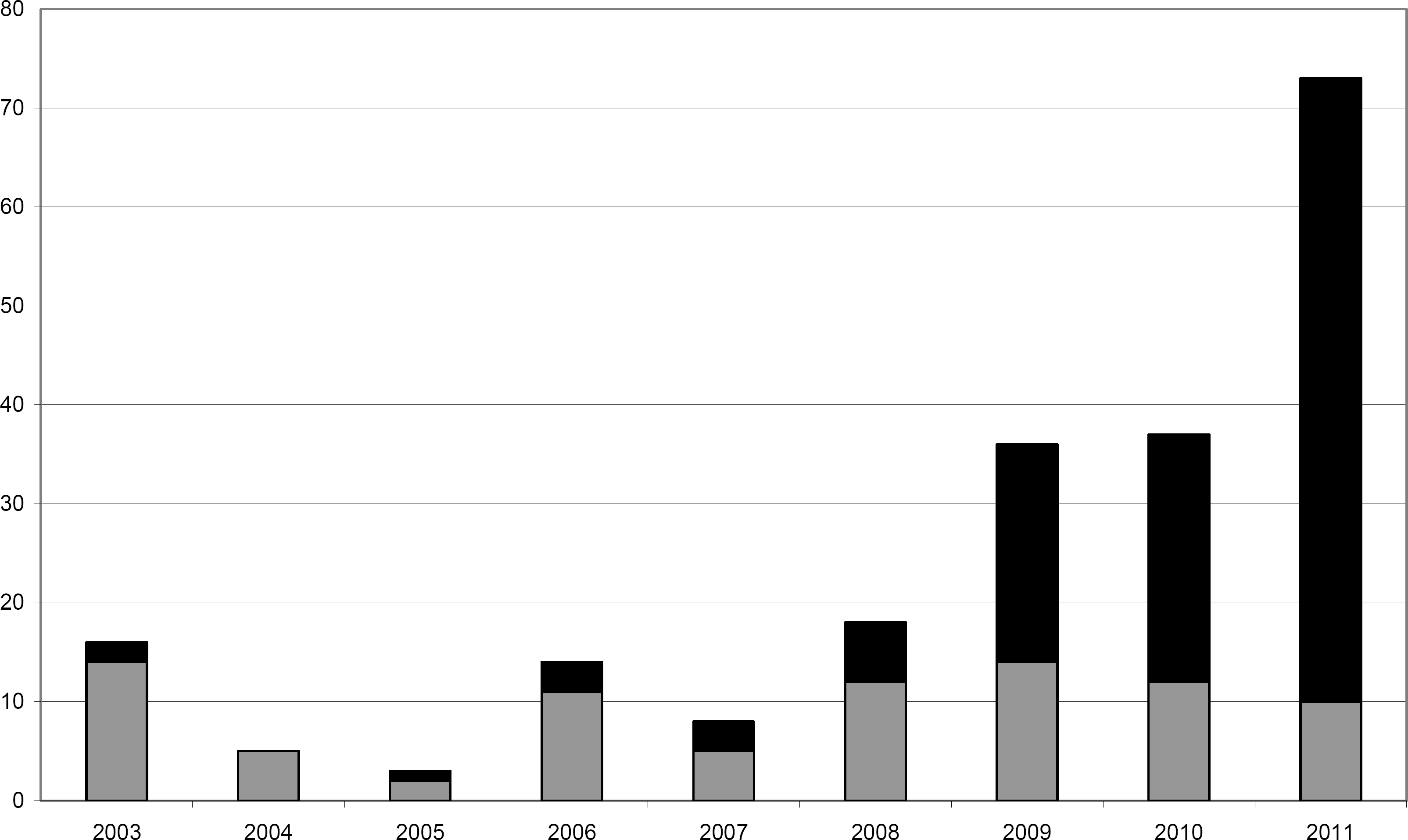
The number of hybrid procedures in 2003–2011 divided into two categories: procedures performed together with interventional radiologists (grey) and solely by vascular surgeons (black).
TECHNICAL PERFORMANCE
All procedures were performed in an operating room (OR) – either in a hybrid OR or using a mobile C-arm in a standard OR. In the early years, the operative techniques varied, but during the last two years, the combination of a surgical and endovascular procedure has become more or less standardized. In the case of femoral endarterectomy, we perform the endarterectomy at the groin and close the artery using a venous patch if necessary. Femoral endarterectomy is carried out as proximally as possible, and the goal is to achieve endarterectomy at least 2 cm above the proximal edge of the arteriotomy, usually reaching the external iliac artery above the inguinal ligament (Fig. 4). The purpose of this maneuvre is to enable the iliac stent to reach the proximal end of the endarterectomy to avoid stenosis in the artery between the distal end of the stent and the proximal end of the endarterectomy. After the closure of the arteriotomy, a standard 5–6 French sheet is inserted by puncture to the distal part of the patch, or the common femoral artery if a patch is not used. The sheet is introduced only a short distance inside the artery to avoid subintimal placement. A terumo guidewire and a catheter is then directed to the intraluminal space of the external iliac artery and the iliac artery is treated endovascularly (Fig. 5). In the case of an iliac occlusion, the retrograde approach was the first choice, and the antegrade approach was adopted only if the retrograde approach failed.
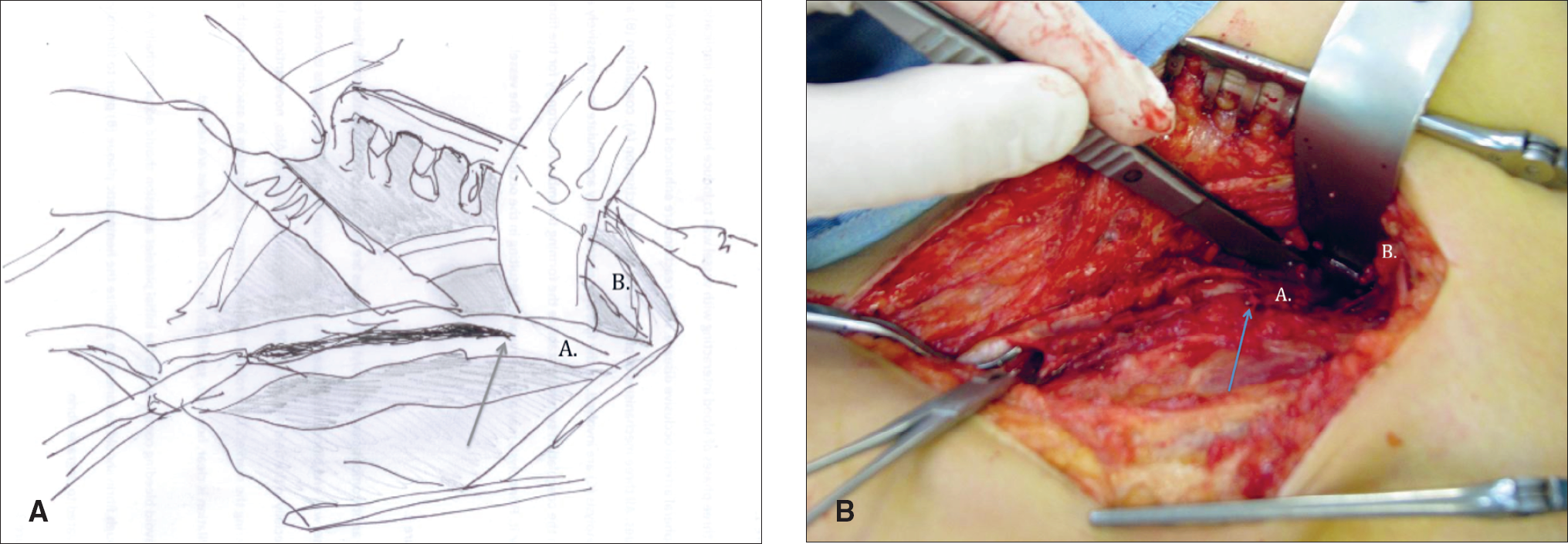
Endarterectomy of the common femoral artery (A.) before proximal endovascular inflow procedure. The endarterectomy is extended 3–4 cm above the proximal end of arteriotomy (arrow) and inguinal ligament (B.) is retracted to achieve the proximal control of external iliac artery.
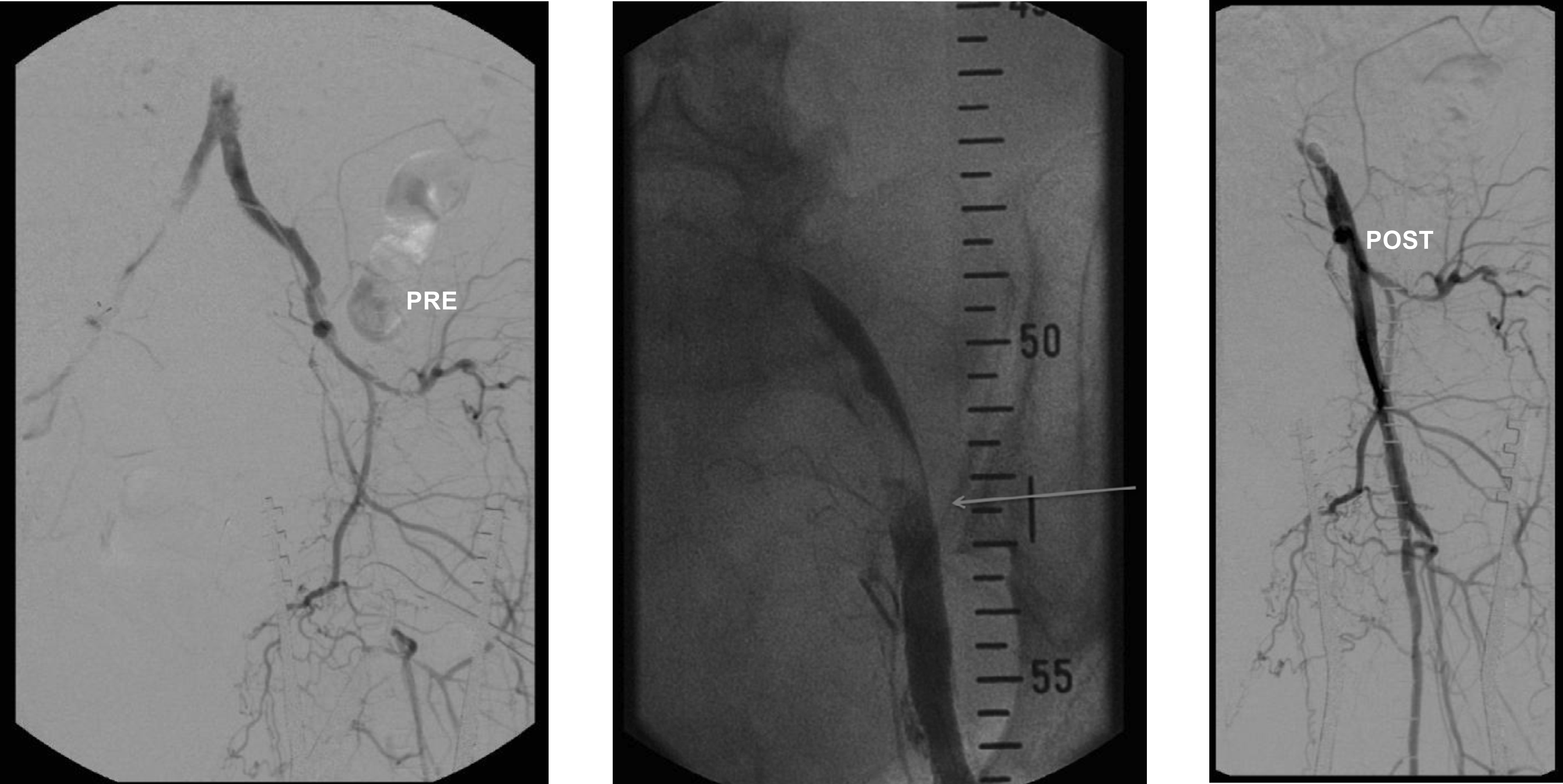
Angiographic images of a patient who underwent endarterectomy of the left femoral bifurcation and inflow PTA. Endarterectomy is performed as proximally as possible (arrow), at least 2 cm above the arteriotomy and the stent is inserted to cover the proximal edge of the endarterectomy site.
CASE
Our case is a 81 years old woman with a history of smoking, type II diabetes, hypothyreosis, hypertension and alcohol abuse. She had undergone endarterectomy of the right common femoral artery in 2002 and PTA and stenting of the left common iliac artery in 2004. She has ASA medication. Her left ankle had been operated due to fracture in 2006 and the osteosynthesis material had not been removed.
Recently, she fell and got a wound to the left ankle. When she arrived to HUCH, she had an infected wound in the left ankle and the osteosynthesis material was visible. Toe pressure in the left first toe was zero and ankle pressure 22 mmHg.
Next day, the osteosynthesis material was removed and the infected wound cleaned and postoperatively treated with vacuum assisted wound therapy (VAC).
On MRI, she had significant stenosis in the left external iliac artery, short occlusions at the orifice of superficial and deep femoral arteries and stenosis of the left superficial femoral artery. The peroneal artery was stenotic and in the proximal part of anterior tibial artery there was an eight cm long occlusion (Fig. 6).
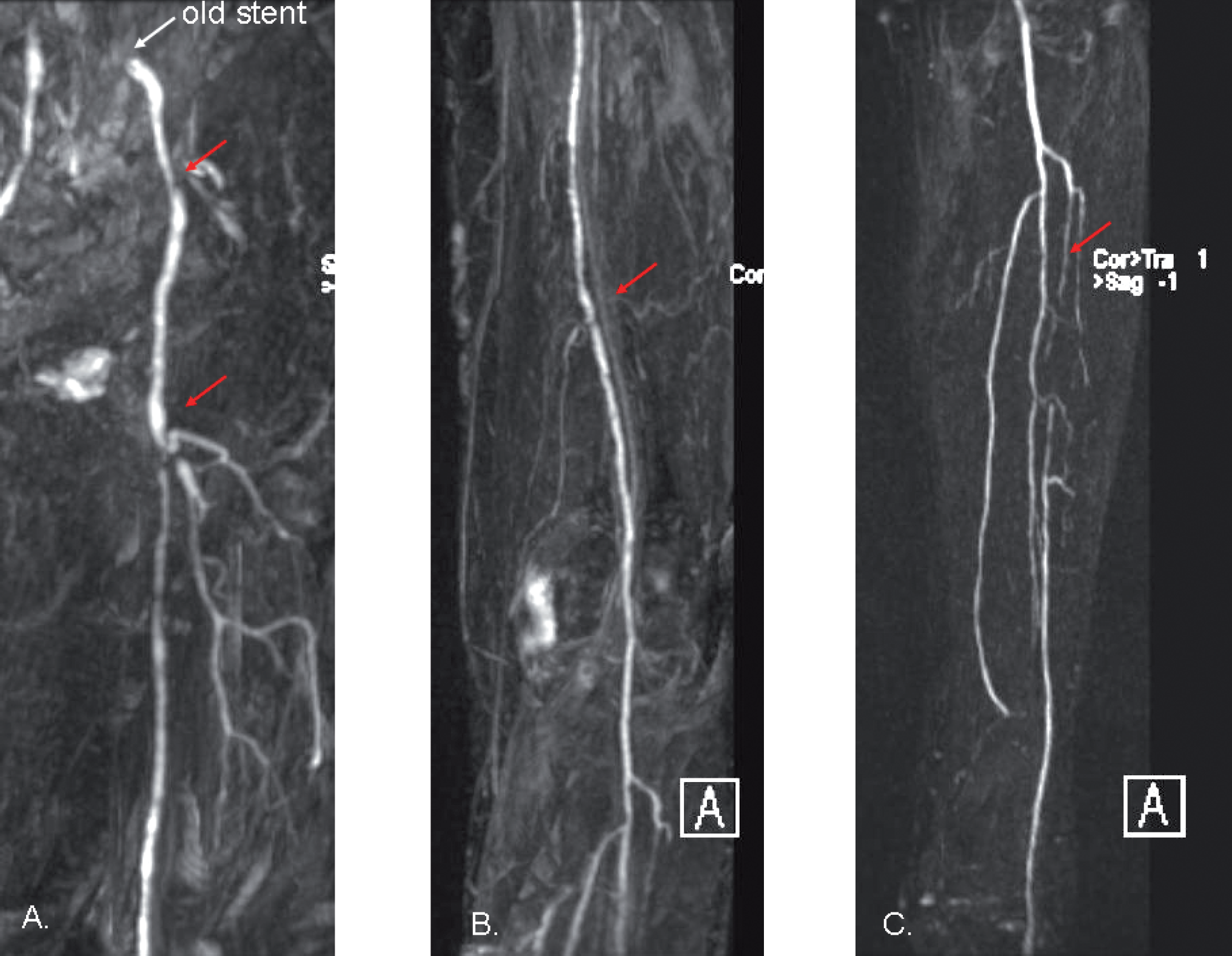
Preoperative magnetic resonance angiography of a patient with infected wound in the left ankle and critical limb ischemia. Atherosclerosis can be seen in the iliac arteries (A.), femoral arteries (B.) and tibial arteries (C.).
Two days later she underwent a hybrid procedure: Endarterectomy of the left common femoral artery, proximal superficial and deep femoral artery was followed by PTA of the external iliac, superficial femoral and peroneal arteries. The occlusion of anterior tibial artery was recanalized and dilatated with a 3 mm balloon (Fig. 7).
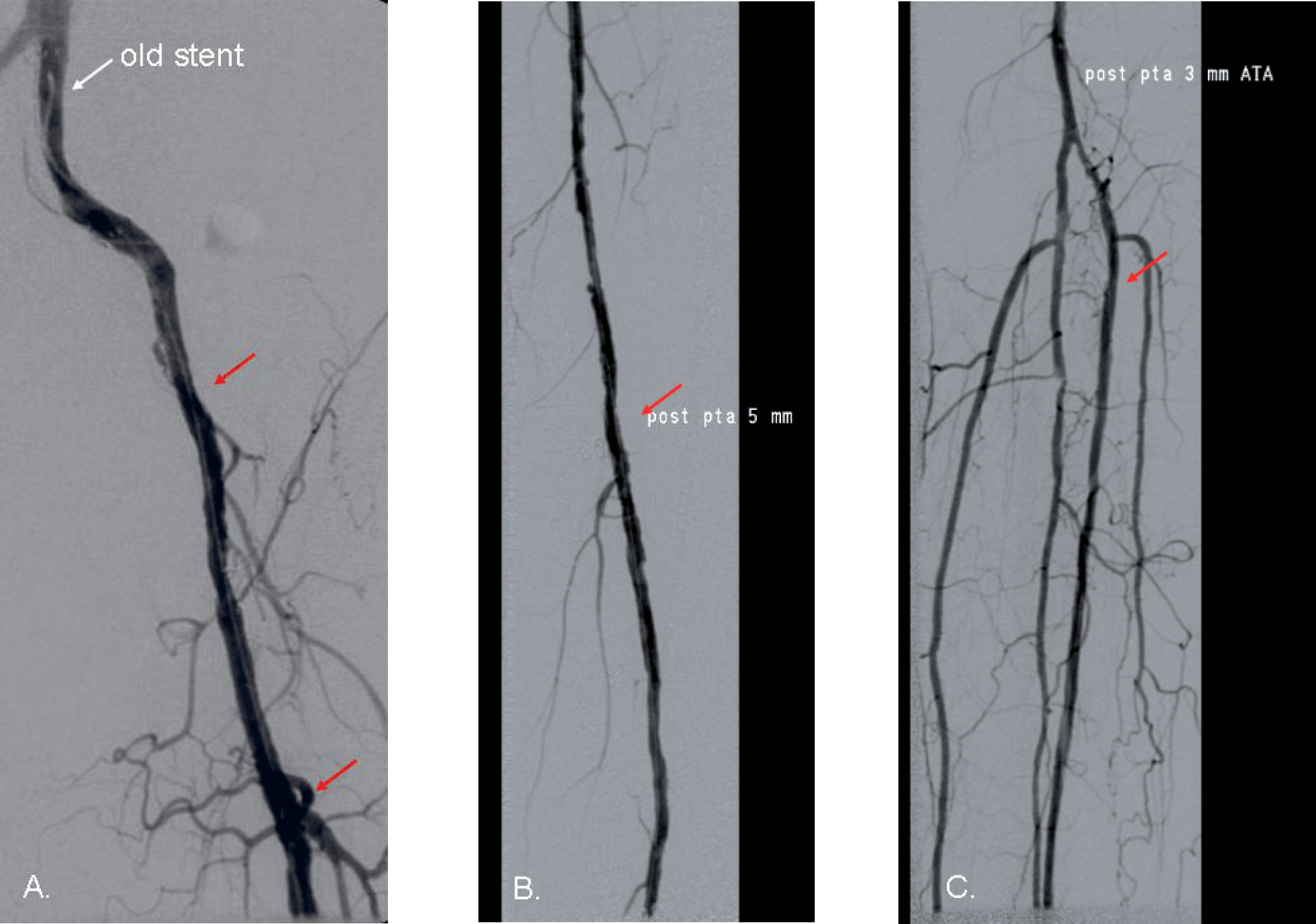
The patient underwent a hybrid procedure: Endarterectomy of the common femoral, superficial femoral (SFA) and deep femoral artery (A.), PTA and stenting of the external iliac artery (A.), PTA of the SFA (B.), PTA of the peroneal artery and recanalization and PTA of the anterior tibial artery (C.).
After the procedure, the toe pressure increased from 0 to 34 and the ankle pressure from 22 to 90 mmHg. An additional wound revision and skin grafting was performed ten days later.
All wounds in the left leg had healed and the patient was ambulatory with a warm foot at follow-up three months after the procedure.
DISCUSSION
Endovascular treatment has gained popularity in the treatment of chronic limb ischaemia. Because of multilevel disease especially in patients with critical limb ischaemia, revascularization is often required at the level of the iliac as well as the femoral arteries, and frequently even at the infrapopliteal segment. Furthermore, the treatment of choice may be endovascular at some levels and surgical in others. As portable C-arms have been available in operating theatres, and even dedicated endovascular suites have been built, endovascular and surgical revascularization has been possible during the same procedure and anaesthesia. In our hospital, the number of hybrid procedures increased during the last 9 years and especially during the last three. One of the most important reasons behind this increase is the adoption of endovascular skills among the vascular surgeons. Although the cooperation between vascular surgeons and interventional radiologists has traditionally been very close in our hospital, the threshold for a vascular surgeon to perform hybrid procedures has, for some reason, been relatively high. When the same surgeon who performs the open surgical revascularization is also able to continue with the endovascular part of the operation, this threshold disappears. This is a way how new approaches and innovative techniques develop.
One of the typical places for atherosclerotic lesions is a bifurcation of the common femoral artery. While the common iliac artery is usually suitable for endovascular treatment with a high technical success rate, a low complication rate and good long-term results, the common femoral artery has many challenges concerning endovascular treatment. Firstly, atherosclerotic lesions often compromise the origin of both the superficial and the deep femoral arteries, and balloon angioplasty of the common femoral artery may occlude the deep femoral artery if the guidewire is in the superficial femoral artery. Secondly, the common femoral artery in the groin is under continuous movement, which may result in stent fractures. Furthermore, after stenting, surgical access to the vessel would be difficult. The common femoral artery is relatively easy to access with open surgery, and so far the first choice of treatment has been surgical endarterectomy (9). Previously, stepwise procedures were common, in which inflow stenosis PTA was performed in an angiolaboratory, followed by femoral endarterectomy or bypass during another operation. Usually, patients went home in the meantime for a week or two and returned to hospital for the open surgery. Today, as we perform more than 70 hybrid procedures per year, a significant amount of angiolaboratory capacity is spared for other patients. With the ageing population suffering from multiple co-morbidities and multi-level disease, all means of making our practices more effective are warranted. In some cases, hybrid procedures may increase procedural costs, but this is compensated by shorter intensive care and hospital stays. On the other hand, as inflow stenosis PTA is performed to allow a more distal inflow segment to distal bypass or distal PTA to achieve more proximal landing zone, the greatest benefit is achieved for the patient who may undergo a minimally invasive procedure with less vein graft required. In some cases, the use of a prosthetic graft can be avoided when a shorter bypass with vein is sufficient.
The technical success of the hybrid procedures in our material is high and comparable with other series. It has not decreased although vascular surgeons have assumed the responsibility for the entire procedures. Due to close cooperation, interventional radiologists are available if consultation or technical advice is needed during the procedure. At the same time, as the number of hybrid procedures has increased and the procedures are performed mainly by vascular surgeons, the endovascular equipments have developed, allowing more challenging anatomies to be treated successfully. Guidewires and catheters have been developed to solve various technical problems – for example, re-entry catheters allow the crossing of the lesion even from a subintimal space.
One of the most common and challenging situations in a hybrid theatre is the iliac recanalization with femoral endarterectomy. Some authors suggest that a guide wire should be placed through the stenotic or occluded iliac segments prior to arteriotomy and endarterectomy. In our technique the arteriotomy is significantly shorter than the blind endarterectomy continuing in a proximal direction, which allows us to shift the distal part of the stenting to the region above the inguinal ligament, still fixing the end of the endarterectomy. With this technique it might be challenging to reach the lumen with the wire and stay away from the subintimal space, but we have succeeded in almost all the cases by carefully directing the guide-wire with the help of a road map. In only few cases has an antegrade stenting been necessary, usually cross-over from the contralateral side.
Despite the clear benefits achieved with the hybrid technique, there are also some limitations. The total time needed for the operation increases by at least 30 minutes, sometimes by hours. If the procedure was performed in two steps, the patient would need shorter general anaesthesia as the endovascular procedure could be performed under local anaesthesia. Because the operating time is longer, the wound in the groin is also exposed for a longer period than during open surgical revascularization only. This may increase the risk of infection. This is a true concern if prosthetic material is used in the groin, and we suggest that it should be avoided if possible.
As the hybrid theatre has made endovascular procedures routine practice for vascular surgeons, education and training should follow the development. So far, there are no systematic or official national endovascular training programmes for vascular surgeons in training in Finland despite the European requirements. The procedures can be learned in daily practice together with senior vascular surgeons with endovascular skills and also under the supervision of radiologists. However, just as important as the skills of using guidewires and balloons is the skill of avoiding excess radiation. This includes theoretical education on radiation and its physical and biological impact including legislation and practical hygiene issues. This is a challenge for vascular surgeons all over the world to improve themselves professionally.
CONCLUSIONS
Hybrid procedures have been used increasingly often for the treatment of multilevel vascular disease in the fragile vascular patient population. The results of the treatment seem to be as good as with open revascularisation, but with less morbidity and shorter intensive care and hospital stay. In our unit, as in many other centres, vascular surgeons have adopted this new technique with good primary success. The long term results are to be analysed in the future. There is a substantial need for endovascular training during vascular surgical education programmes, with a special emphasis on radiation hygiene and novel endovascular techniques.