
Abstract
Background and Aims:
Early results of fluted and tapered distal fixation stems used in reconstruction of deficient femora in femoral revision arthroplasty have been successful in small series. We evaluated the survival of the LINK MP Reconstruction Hip Stem and factors associated with survival using data from a nation-wide arthroplasty register.
Materials and Methods:
408 femoral revisions using LINK MPReconstruction Hip Stem were performed during 1994 to 207. The mean age of the patients was 72.5 (range: 36–93) years and 63% were performed in women. Kaplan-Meier analysis and the Cox regression model were used for the survival analysis. The effects of age, sex and diagnoses were also studied.
Results:
The 9-year overall survivorship for the LINK MPReconstruction Hip Stem was 75% (95% CI 70–80). Aseptic loosening was rare; the 9-year revision rate for aseptic loosening was only 3%, which coincides with earlier reports with shorter folllow-up. The most common reason for re-revision was dislocation of the prosthesis with or without malposition of the socket (67%). Indication for revision strongly affected the survival rate with revisions for dislocation having an over 3-fold and revisions for infection a 3-fold relative risk for re-revision compared to revisions for aseptic loosening. Increasing age slightly decreased the risk of re-revision but sex did not affect the survival.
Discussion:
Based on our findings, we conclude LINK MP Reconstruction Hip Stem, as an example of a fluted and tapered distal fixation stem, appears to solve many problems with implant fixation in femoral revisions. High number of dislocations suggests that special attention should be paid to correct center of rotation, to correct implant positioning and to need of constrained implants in case of deficient abductor mechanism.
Keywords
INTRODUCTION
Modular femoral components with grit-blasted fluted and tapered distal fixation appear suitable tools in femoral reconstruction in revision total hip arthroplasty with femoral bone loss and in treatment of periprosthetic fractures (1 –11). There have been some reports with significant postoperative stem migration (4, 5, 9) but otherwise the published series have been very promising. As with other hip revision arthroplasty, the risk of dislocation may be over 10%. Rate of stem re-revision aseptic loosening has varied between 1.4% to 7.3% at < 5 years (1 –11). Majority of the previous studies report results after short to mid-term follow-up, with number of patients varying between (n = 62 to 129) and/or are from specialized centers.
LINK MP Reconstruction Hip Stem is a modular femoral stem with grit-blasted fluted and tapered distal fixation. Purpose of this study was to analyze its survival rate in femoral revision and factors affecting the survival rate.
PATIENTS AND METHODS
Our study was based on information recorded in the Finnish Arthroplasty Register (12) relating to patients who underwent femoral component revision using the LINK MP Reconstruction Hip Stem (Waldemar Link, Hamburg, Germany) between 1994 and 207. The coverage of the Finnish Arthroplasty Register was analyzed in 1994–1995 by comparing its data with those of the discharge registers of the participating hospitals; it was found to cover 90% of implantations and implant removals. Since 1995, the data of the register have been compared with those of the hospital discharge registers every few years. Currently, over 95% of implantations are recorded. Revisions were linked to the primary operation, using the unique personal identification number assigned to each resident of Finland.
The register contains data on 429 LINK MP Reconstruction Hip Stems, each of which have been recorded individually for every operation since the beginning of the Register. Among these operations 408 (95%) were revision THAs and 21 (5%) were primary THAs. The revision cases were selected for further analysis.
In Finland, the majority of the 408 femoral revisions with LINK MP Reconstruction Hip Stems were due to aseptic loosening of the femoral or both prosthesis components (n = 157; 39%). In 86 hips there was a periprosthetic femoral fracture (21%). Periprosthetic joint infection (PJI) accounted for 21 (5%) of the revisions. Other indications included dislocation of the prosthesis with or without stem malposition (n = 66; 16%), femoral revision in conjunction with revision of aseptic loosening of the socket (n = 25; 6%) fracture of the prosthesis (n = 10; 2%), and other indications including conversion of a hemiarthoplasty with acetabular degeneration into a THA (n = 41; 10%). In 27 hips (7%), the indication was incompletely recorded. In 18 of the 21 revisions for PJI, the exchange was performed as a II-stage revision.
Using revision for any reason as the end point, we compared the survival of femoral revisions with LINK MP Reconstruction Hip Stems performed due to 1) aseptic loosening of one or both prosthesis components or prosthesis fracture or other indication including liner exchange, 2) dislocation, 3) periprosthetic joint infection, and 4) periprosthetic fracture in order to assess the impact of underlying disease.
The endpoint for survival was defined as revision with either one component or the whole implant removed or exchanged. Kaplan-Meier survival data were used to construct the survival probabilities of implants at 1, 5 and 9 years. The Cox multiple-regression model was used to study differences between revision indications and to adjust for potential confounding factors. Other indications for revision were compared with periprosthetic fracture (reference indication). In all models, the confounding factors were age, gender and indication for revision THA. The model included adjustment for differences in age and gender.
The Cox regression analyses provided estimates of survival probabilities and revision risk ratios (RR) for different factors. Estimates from the Cox analyses were used to construct adjusted survival curves at mean values of the risk factors. The Wald test was applied to calculate p-values for data obtained from the Cox multiple regression analysis. Differences between groups were considered statistically significant if the p-values were less than 0.05 in a two-tailed test.
We used SPSS 17.0 statistical software (SPSS Inc, Chicago, Illinois, U.S.A.) for the statistical analysis.
RESULTS
Of the 408 femoral component revisions using the LINK MP Reconstruction Hip Stem, 258 (63%) were performed in women and 224 (55%) on the right hip. At the time of the operation, the mean age of the patients was 72.5 (range: 36–93) years. The annual use of the LINK MP Reconstruction Hip Stem is shown in Figure 1.
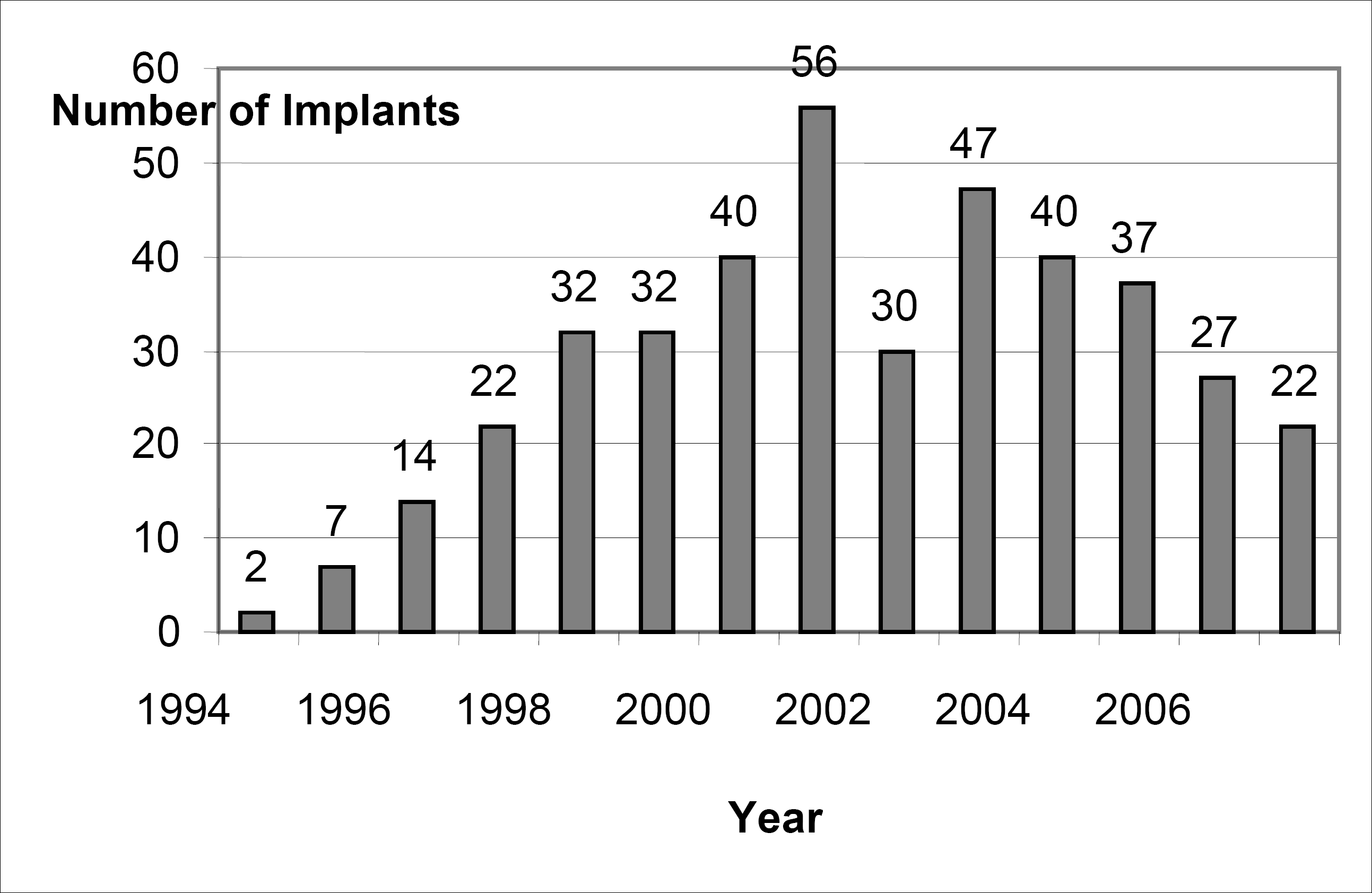
Number of LINK MP Reconstruction Hip Stems implanted in Finland per year during 1994–2007.
The 1-, 5- and 9-year survivorships for the whole LINK MP Reconstruction Hip Stem cohort were 87% (95% CI 84–90), 78% (95% CI 73–83) and 75% (95% CI 70–80) using re-revision for any reason as end point, and 98% (95% CI 97–100), 97% (95% CI 95–99) and 97% (95% CI 95–99) using re-revision for aseptic loosening of the stem as end point (Figure 2).
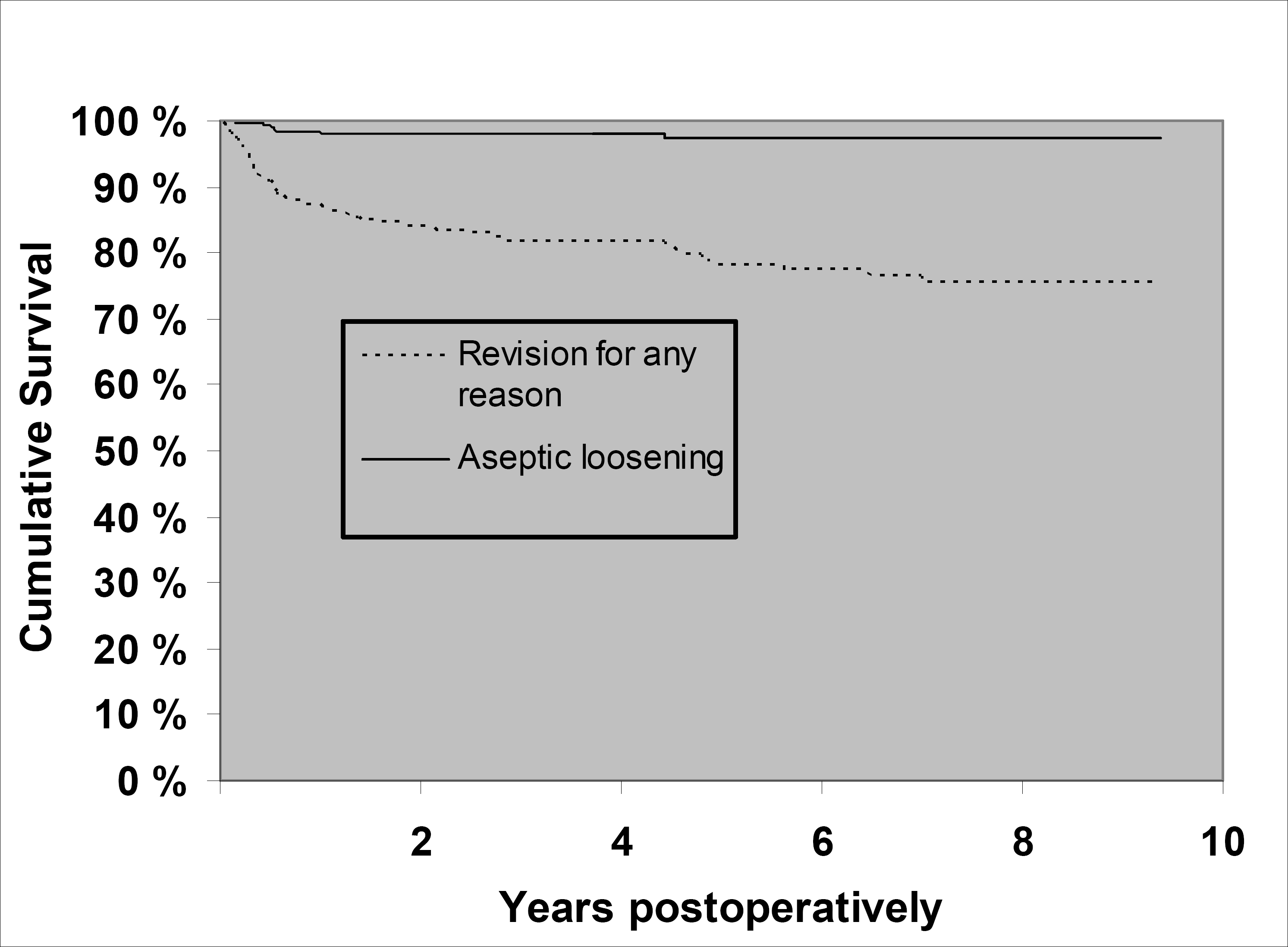
Kaplan-Meier survival curves for 408 femoral revisions with LINK MP Reconstruction Hip Stems (mean follow-up 3.8 years). The end-point was defined as revision for any reason, or for aseptic loosening of the LINK MP Reconstruction Hip Stem.
Sex did not have any statistically significant effect on survivorship in the Cox multiple regression models. Age, on the other hand, was found to significantly affect stem survivorship: each additional year in age decreased the risk of re-revision by 3.1% (95 % CI 1.2–5.0, p = 0.001).
The Cox regression model (adjusted for age and sex) showed an increased risk of re-revision in femoral revisions due to aseptic loosening, dislocation and infection compared to revisions due to periprosthetic fracture (Table 1).
Overall and indication-based survival and Cox-adjusted risk ratio for revision of LINK MP Reconstruction Hip Stems over 1994–2007 in Finland. The end-point was defined as revision for any reason of one or both of the prosthesis components.
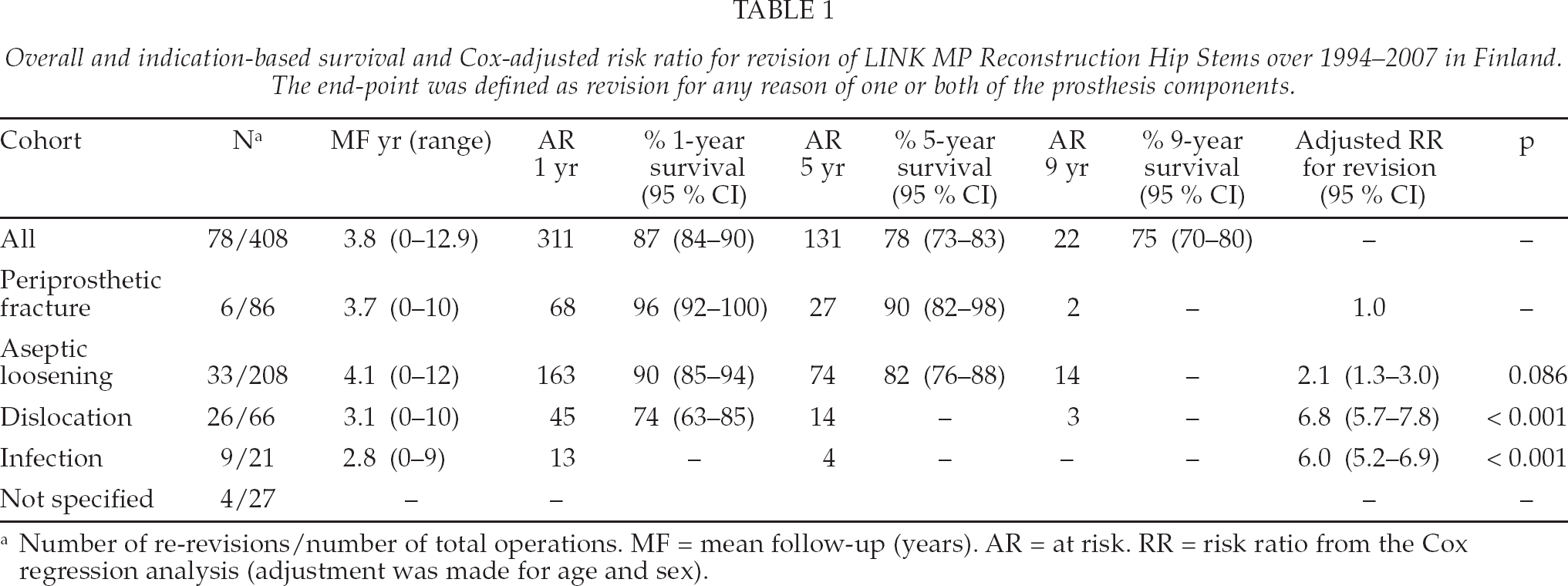
Number of re-revisions/number of total operations. MF = mean follow-up (years). AR = at risk. RR = risk ratio from the Cox regression analysis (adjustment was made for age and sex).
During the 1994–2007 period, 78 revisions were reported. Thus, the 9-year survivorship for the whole LINK MP Reconstruction Hip Stem cohort was 75% (95% CI 70–80). The most common reason for revision was dislocation of the prosthesis with or without malposition of the stem (n = 52, 67%). This was followed by aseptic loosening of the stem with or without aseptic loosening of the cup 10% (n = 8), PJI 4% (n = 3) and periprosthetic fracture 3% (n = 2), of operations. One stem fracture also occurred (1%) at 4.5 years after revision. Other reasons (including liner exchange) accounted for 15% (n = 12) of the revisions. 59% (n = 30) of dislocations requiring re-revision occurred within 6 months after revision, and in 18/52 of the dislocations the indication for revision had been dislocation.
DISCUSSION
We found that the LINK MP Reconstruction Hip Stem showed acceptable short- and mid-term survivorship in femoral revisions at a nation-wide level. Aseptic loosening of this stem was rare; the 9-year survival rate was 97% (95% CI 95–99) using revision for aseptic loosening of the stem as the end-point. Increased age had a positive effect on stem survival. Indication for revision strongly affected the survival rate with revisions for dislocation and infection having an over 3-fold relative risk for re-revision compared to revisions for aseptic loosening. Majority of the re-revisions (67%) were performed due to prosthesis dislocations.
We acknowledge that the register-based studies have certain limitations. For example, we were not able to report any subjective outcome measurements, e.g. hip performance scores or disease-specific quality of life measurements. Moreover, it is not possible to conduct radiographic analyses in register-based analyses on the large number of register-based patients.
A previous study using the ZMR Revision implant (Zimmer, Warzaw, In) with a proximal spout body and a tapered distal stem from the Danish Arthroplasty Registry (DAR), found a 5-year survival of 97% and 94% using aseptic loosening and any revision as the end-point, respectively (9). Another study from Swedish Hip Register (SHR) reported corresponding 5-year survivals of 98 % and 90% for the LINK MP Reconstruction Hip Stem (8). These results and our survival rate using aseptic loosening as the end-point (97%) confirm the reliable osseointegration achievable with the grit-blasted fluted and tapered distal stem. The lower survival rate free of any revision (78%) in the present study, is probably due to the higher number of revisions performed for dislocations (16%) compared to DAR (4.8%) and SHR (< 8%), since this indication was associated with an over 3-fold risk of re-revision compared to aseptic loosening.
In other studies from single arthroplasty units and including other grit-blasted fluted and tapered distal stems, the proportion of re-revision free stems has varied between 80% to 99% and the mean follow-up time between 8 to 50 months. However, these studies did not use a formal survival analysis and the end-points were not well defined. Murphy and Rodrigues revised 1/35 Link MP stem due to deficient osseointegration and 6 more hips due to dislocation (3). Park et al. had 1/62 Lima-L to stems (Lima-Lto, Udine, Italy) re-revised due to infection and one more revision due to dislocation (4). McInnis et al. had 2 periprosthetic fractures and 3 dislocations among 70 PFM stems (Sulzer Orthopedics, Baar, Swizerland) (5). In their study on Vancouver type B2 and B3 femoral periprosthetic fractures, Mulay et al. found 2 non-unions and 2 dislocations among 24 femora treated with Link MP stem (6). Wirtz et al. had 2/142 and 5/142 MRP-Titan stems (Corin, Cirencester, UK) re-revised due to aseptic loosening and dislocation, respectively (10). Lakstein et al. had 2 aseptic loosenings and one PJI requiring re-revision among 84 femoral revisions with the ZMR stem, reporting a 92.7% survival at mean follow-up of 46 months (11). In our study, there were 52 re-revisions due to dislocation. Majority of these dislocations occurred within the first 6 month after revision. Stem migration may have a role in the risk of dislocation but without radiographic analysis it remains only speculation.
Other distally fixed reconstruction options for proximally deficient femora include modular implants with uncemented extensively porous coated stems or interlocking stems, and impaction bone grafting with a polished tapered cemented stem. 10-year survival rates of up to 96% have been reported with cylindrical, porous coated stems (13) but there are also reports with 11% stem subsidence rates, some leading to femoral re-revision (14). Philippot et al. used the hydroxyapatite-coated REEF Distally Interlocked Modular Femoral Reconstruction Prosthesis (DePuy International, Leeds, England) in 43 hips with 5-year survival of 97.7% and 2% dislocation rate (14). However, the use of interlocking screws creates a stress riser in femoral diaphysis, possibly predisposing to periprosthetic fracture. Impaction bone grafting with a polished tapered cemented stem resulted in 38% (13/34) subsidence rate among hips revised for aseptic loosening (15). Unfortunately direct comparison of these results with tapered distal stems is not possible. As subsidence occurs with both tapered and cylindrical porous-coated stems, we aim to achieve substantial proximal support with some calcar-replacing prosthesis design with trochanteric fixation when needed. Distal fixation with interlocking screws provides further support in situations where rotatory stability is difficult to achieve. We believe that use of impaction grafting and cemented stem is seldom indicated.
Based on our findings, we conclude that the LINK MP Reconstruction Hip Stem appears to solve many problems with implant fixation in femoral revisions with deficient bone. Reported subsidence rates indicate that in addition to distal fixation some proximal support is often needed. High number of dislocations suggests that special attention should be paid to correct center of rotation, to correct implant positioning and to need of constrained implants in case of deficient abductor mechanism, especially when the revision is due to dislocation.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by the Sigrid Juselius foundation.