
Abstract
Background and Aims:
We have previously shown that nutritional guidelines decreased the incidence of pressure ulcers in hip fracture patients. In the present study, we evaluate whether the nutritional biochemical markers S-IGF-1 (Insulin-like Growth Factor 1), S-Transthyretin and S-Albumin are affected by patients' energy intake, and whether the markers are useful as predictors of postoperative complications.
Material and Methods:
Quasi-experimental design, with one intervention and one control group, as well as pre- and post-study measurements. Eighty-eight hip fracture patients were included: 42 in the control group and 46 in the intervention group. The control group received regular nutritional support pre- and postoperatively, while the intervention group received nutritional support that followed new, improved clinical guidelines from admission to five days postoperatively. S-Albumin, S-Transthyretin, C-Reactive Protein (S-CRP) and S-IGF-1 were analysed at admission and five days postoperatively as well as complications like pressure ulcer and infection.
Results:
The intervention group had a significantly higher energy intake; for example, 1636 kcal versus 852 kcal postoperative day 1. S-IGF-1 levels decreased significantly in the control group, while no decrease in the intervention group. S-Albumin and S-Transthyretin decreased and S-CRP increased significantly in both groups, indicating that those markers were not affected short-term by a high-energy intake. There was no correlation between short-term postoperative complications and S-IGF-1, S-Transthyretin or S-Albumin at admission.
Conclusion:
The results of our study showed that S-IGF-1 can be used as a short-term nutritional biochemical marker, as it was affected by a five-day high-energy regimen. However, neither S-IGF-1, S-Transthyretin or S-Albumin were useful in predicting postoperative complications within five days postoperatively.
Keywords
INTRODUCTION
Patients with a hip fracture are often malnourished at the time of hospital admission (1, 2), and malnutrition is associated with increased risk of developing postoperative complications (2 –6). Consequently, it is important to identify malnourished patients at admission in order to prevent postoperative complications. Many postoperative complications occur already 2–4 days after surgery, for example pressure ulcer (5) and urinary tract infection (7). Several risk assessment tools may be used to assess nutritional status. The assessment tool must be practical, rapid, simple, valid and meaningful in order to be used by health professionals. Nutritional Risk Screening (NRS-2002), Mini-Nutritional Assessment (MNA) and Short Form Mini-Nutritional Assessment (MNA-SF) are among the different tools commonly used to asses nutritional status, often employed in clinical practice as well as in research with orthopaedic patients (8). The tools include questions about body mass index, weight loss, current nutritional intake, illness, physical and mental factors (8, 9).
Some authors prefer to use biochemical nutritional markers such as albumin and transthyretin (prealbumin) levels to assess nutritional status (10), although albumin is known to be affected by both infection and the normal inflammatory response following trauma (11, 12). Another biochemical marker, Insulin-Like Growth Factor −1 (S-IGF-1), has also been suggested as a marker of nutritional status (10), and is reported not to be as affected by inflammation and trauma as albumin (10,–12). In addition, S-IGF-1 has higher diagnostic sensitivity and specificity if the nutritional status improves compared with albumin (11, 12).
In our previous study at Uppsala University Hospital, Sweden, we performed a study on 100 patients with hip fracture in order to investigate whether nutritional supplements administered in accordance with nutritional guidelines aimed at a high energy intake administered before and for five days after surgery would decrease postoperative complications. The results showed a significant decrease in the prevalence of pressure ulcers (36% compared to 18%), and a decreased occurrence of hospital-acquired infections (18% to 8.7%), as well as a shortened median length of hospital stay (9 days compared with 7 days) (13). In the current study, we perform an extended analysis to investigate whether S-IGF-1, S-Transthyretin and S-Albumin were affected by high-energy intake.
Another study, performed in Switzerland, with hip fracture patients who received protein supplements for six months, a long-term nutritional intervention, showed increased levels of IGF-1 compared to those who did not receive any supplements (14). Our hypothesis is that a short-term intervention, up to five days postoperatively, will affect IGF-1 but is too short term to affect Albumin and Transthyretin.
AIM
The primary aim of the present study was to investigate whether the biochemical markers S-IGF-1, S-Transthyretin and S-Albumin are affected by patients' energy intake. The secondary aim was to investigate whether the biochemical markers are useful in predicting postoperative complications.
MATERIAL AND METHODS
STUDY DESIGN
The design was quasi-experimental, with one intervention and one control group, as well as pre- and post-study measurements. The population included in the present study was previously studied to address other aspects of the importance of nutrition following hip fracture surgery (13).
SUBJECTS
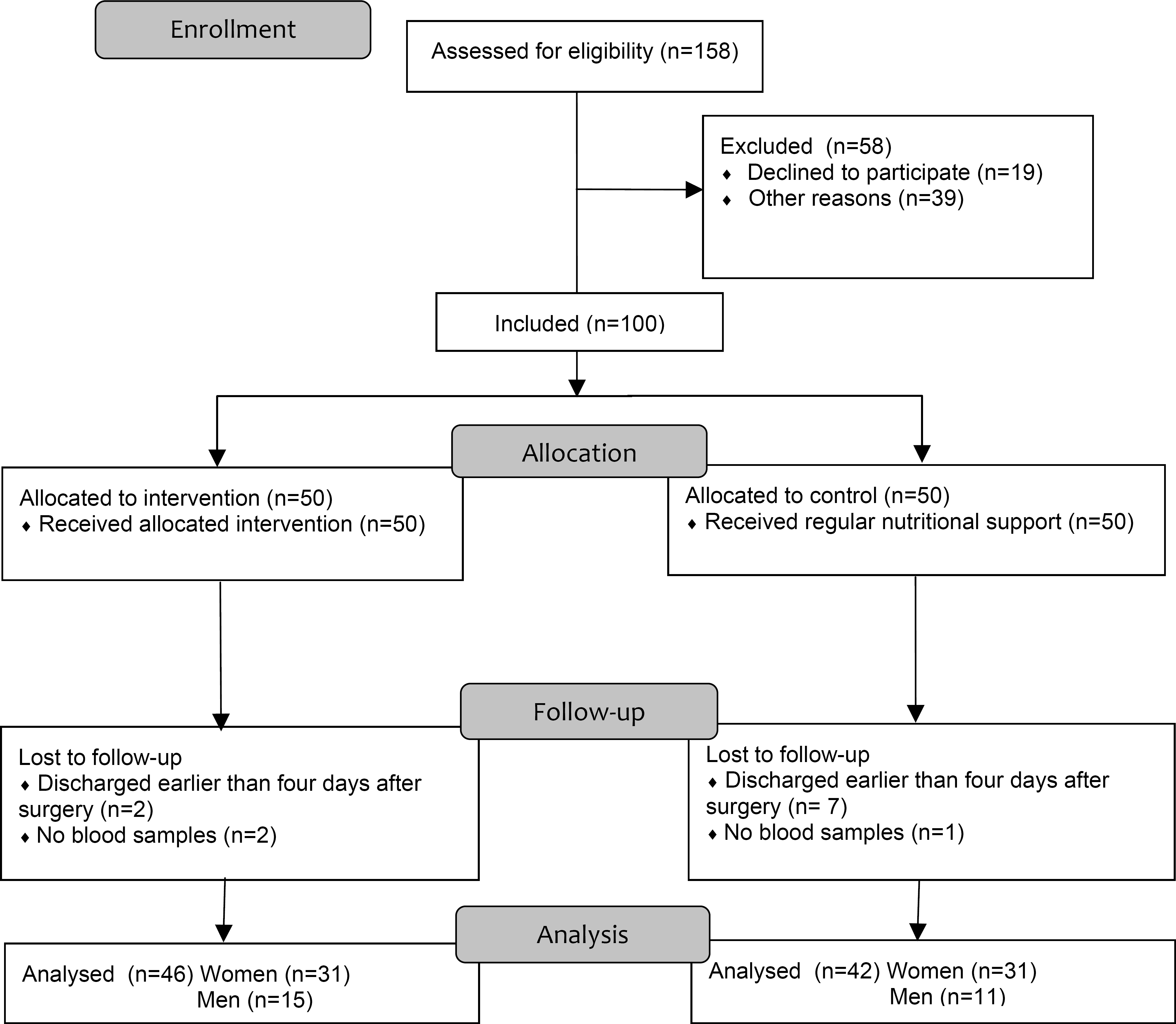
One hundred consecutively admitted patients with hip fracture were included in the study, 50 in each group. The first 50 patients formed the control group, while the next 50 made up the intervention group. Nine patients were lost to follow-up, seven in the control group and two in the intervention group, shown in the flow diagram (Fig. 1). Three patients, one in the control group and two in the intervention group, had no blood samples and were excluded. The mean age for both groups was 81 years (women 83 years, SD 7,6; men 78 years, SD 9,7), and 70 % of the patients were women. There were no significant differences between the groups at admission to the ward related to age, gender, body weight, fracture, type of surgery or time to surgery (Table 1).
Subjects
Baseline data
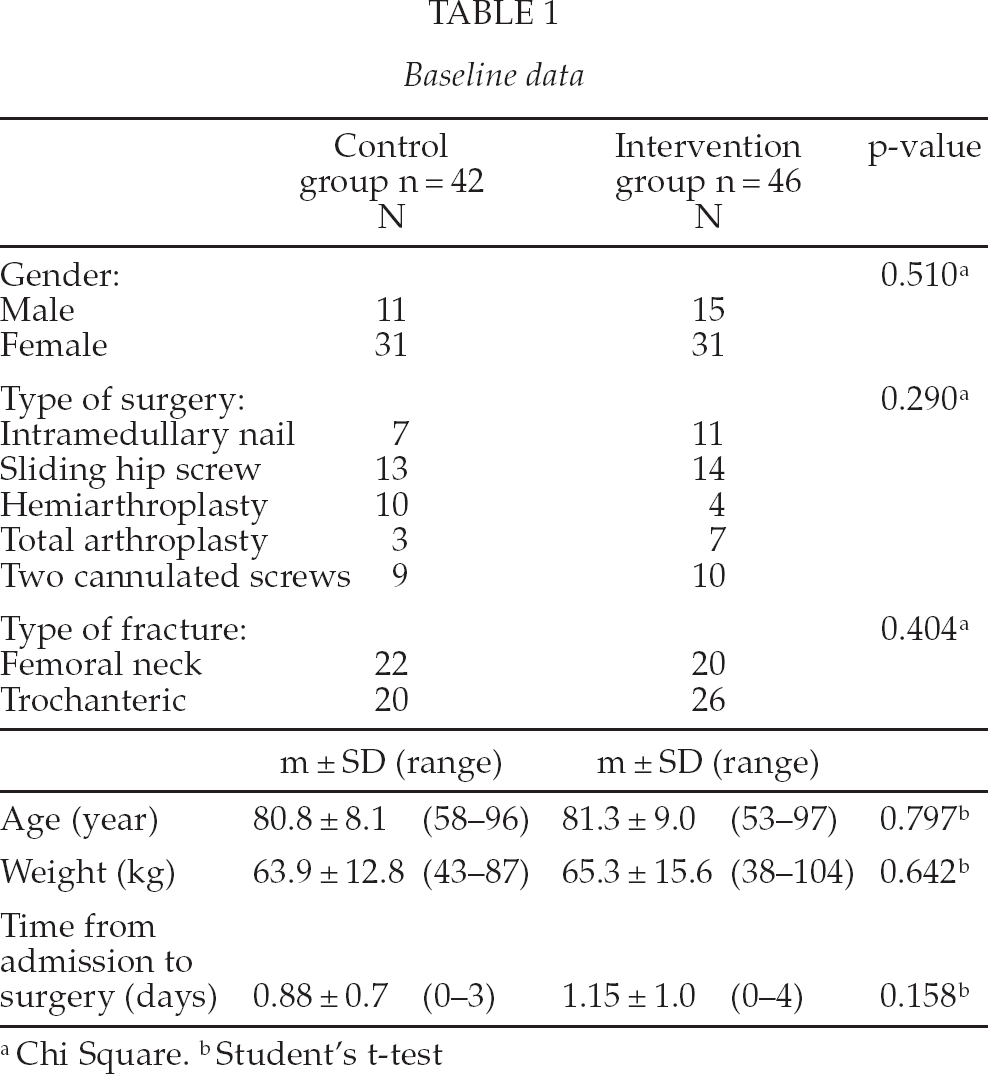
Chi Square.
Student's t-test
Exclusion criteria included patients in need of dialysis, patients with kidney disease requiring protein-reduced food or liquid restrictions, and patients with severe liver disease.
Fifty-eight (36.7%) possible hip fracture patients were not included, 23 during the period when controls were enrolled and 35 during the intervention period. No significant differences were found between patients who did or did not participate in terms of gender (χ2 = 2.6, p = 0.107, df = 1) or age (t = 1.064, p = 0.289, df = 152).
ENERGY INTAKE IN CONTROL AND INTERVENTION GROUPS
Intervention group
The intervention group received nutritional supplements according to nutritional guidelines developed by a multidisciplinary team; a dietician, orthopaedic surgeon and registered nurse. The guidelines included two preoperative carbohydrate drinks (100 kcal/200 mL), an intravenous glucose infusion (50 mg/mL) preoperatively, and nutritional drinking supplements (300 kcal/200 mL), three times a day for five postoperative days. The energy requirement (30 kcal/kg) (15) was calculated for each patient. The first day after surgery, the calculated energy requirement represented at least one-third of the energy needed, the second day represented half of the energy needed, and from day three, 75 % of the energy needed. If the nutritional goal was not reached, additional interventions were performed according to the guidelines, including intravenous fluids and tube feeding.
Control group
The control group received standard nutritional support pre- and post-operatively at the ward.
DATA COLLECTION
At both admission and five days postoperatively, assessments of nutritional status and complications were made. Nutritional and liquid intake were assessed daily from admission until five days postoperatively. When the patient was discharged from the ward, length of stay was calculated. Data was collected on specific Clinical Report Forms by one of the authors (A-K G) and by the nurses at the ward.
Assessment of nutritional status
Biochemical markers
Venous blood samples were taken to measure the levels of S-Albumin, S-Transthyretin and S-IGF-1. S-CRP was also analysed to elucidate how inflammation affects the nutritional biochemical markers. Biochemical analyses were performed at the Department of Clinical Chemistry at Uppsala University hospital. The samples were kept frozen at −70 °C until analysis by established routine methods at the laboratory. Serum measurement of CRP and Albumin were performed on an Architect Ci8200® analyser (Abbott Labs). The highly sensitive S-CRP assay had a total analytical CV of 0.8% at 8 mg/L, and a 0.2 mg/L detection limit. S-Albumin had a CV of 0.3% at 32 g/L. S-Transthyretin was analysed on an automatic immunoassay (BN ProSpec, Siemens Healthcare Diagnostics GmbH) with a total analytical CV of 3.0% at 150 mg/L. S-IGF-1 was analysed on an automated immunoassay (IMMULITE® 2000; Siemens Healthcare Diagnostics GmbH) with a total analytical CV of 3.7 % at 55 μg/L.
S-Albumin below lower reference value (2 standard deviations below the mean of the age group), i.e. < 35 g/L was interpreted as moderate malnutrition and S-Albumin < 30 g/L was interpreted as severe malnutrition (16). S-IGF-1 < 55 μg/L (2 standard deviations below the mean of the age group), was interpreted as moderate malnutrition (17). S-Transthyretin < 170 mg/L was interpreted as moderate malnutrition (18). S-CRP was used to evaluate the acute-phase response following the fracture event and the surgical procedure.
Postoperative complications
Hospital-acquired pressure ulcers
Patients' skin was examined for pressure ulcers, and any ulcers were classified according to the European Pressure Ulcer Advisory Panel guidelines. Category I: non-blanching erythema of intact skin. Category II: partial-thickness skin loss involving epidermis, dermis or both. Category III: full-thickness skin loss involving damage to or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia. Category IV: full-thickness skin loss with extensive destruction, tissue necrosis or damage to muscle, bone or supporting structures (19).
Hospital-acquired infection
The medical record was audited for hospital acquired infection, i.e., a physician's diagnosis of wound infection, urinary tract infection, pneumonia or sepsis at admission and five days postoperatively.
DATA ANALYSIS
The data analysis was performed using SPSS 17.0. For descriptive purposes, means, standard deviations and percentages were used. For comparison between groups, a Student's t-test was used for continuous variables (e.g., age, energy intake and preoperative days). For dichotomous variables (e.g., gender, fracture type, type of surgery and postoperative complications), a Chi-square test was used. For comparison within the groups, a paired sample t-test was used for parametric data (e.g., g/l, mg/l and μg/L). The Mann-Whitney U-test and Wilcoxon Signed Rank Test were used for non-parametric analysis (e.g., μg/L, mg/L, g/L). Data was analysed both by group and gender. For gender, only the significant results are presented. Significance level p < 0.05 was used.
ETHICAL CONSIDERATIONS
The regional Ethical Review Board in Uppsala (Date 2005-06-15 Reg No 2005:150) approved the study. The study conformed to the Helsinki Declaration. Each patient signed an informed consent at the time of study inclusion. If the patients were unable to fully understand the information, a relative was given the information and as a proxy asked about the patient's participation.
RESULTS
The postoperative energy intake in the intervention group was significantly higher than that in the control group (Table 2); for example 1636 kcal versus 852 kcal postoperative day 1. S-IGF-1 decreased significantly between admission and five days postoperatively in the control group, while there were no significant differences in the intervention group. Within both groups, S-Albumin and S-Transthyretin decreased significantly and S-CRP increased significantly. At five days postoperatively the women in the intervention group had a significantly higher S-IGF-1 (mean 80.4, SD 33.4) compared to the women in the control group (mean 62.5, SD 23.6) (p = 0.018). In the control group the women had a significantly lower S-Albumin (mean 29.4, SD 4.2) than the men (mean 33, SD 4.6) (p = 0.025). There were no difference in the energy intake between women and men.
Energy intake the first three days after surgery
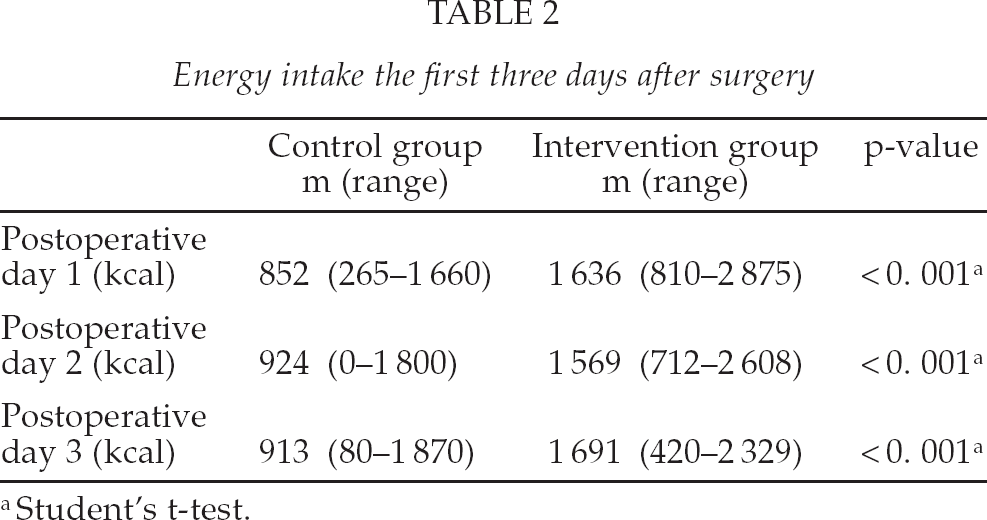
Student's t-test.
Upon arrival to the ward, five patients in the control group and 15 in the intervention group were identified to be malnourished (moderate and severe) according to their concentration of S-Albumin (Table 3). According to S-IGF-1 levels, seven were malnourished (moderate) in the control group and 10 in the intervention group. The levels of S-Transthyretin showed that 14 of the patients in the control group and 14 in the intervention group were identified as malnourished (moderate). No significant differences between men and women were found.
Comparison of biochemical markers preoperatively and five days postoperatively
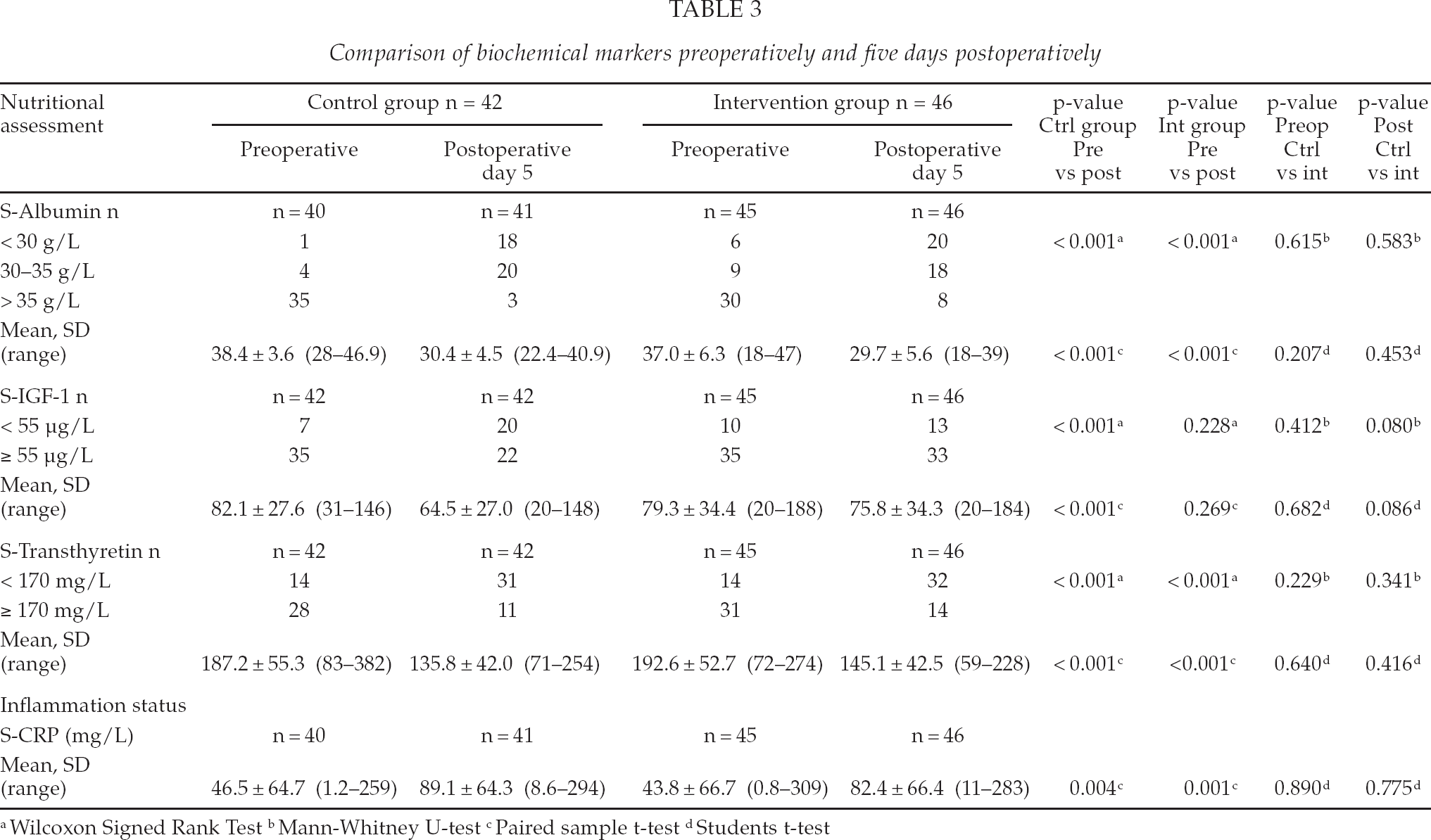
Wilcoxon Signed Rank Test
Mann-Whitney U-test
Paired sample t-test
Students t-test
Five days postoperatively, 38 of the patients in the control group and 38 in the intervention group were malnourished (moderate and severe) according to S-Albumin. According to S-IGF-1, 20 were malnourished (moderate) in the control group and 13 in the intervention group. The levels of S-Transthyretin showed that 31 of the patients in the control group and 32 in the intervention group were identified as malnourished (moderate). No significant differences between men and women were found.
Postoperative complications were found in 21 patients in the control group. There were 16 patients with pressure ulcers (category 1: n = 4 and category 2: n = 12) and seven patients with hospital-acquired infections, two patients with both. In the intervention group, postoperative complications were found in 13 patients, nine patients with pressure ulcers (category 1: n = 3 and category 2: n = 6) and four patients with hospital-acquired infections. The women in the control group had significantly more postoperative complications (n = 18) than the women in the intervention group (n = 10) (p = 0.041).
At admission to the ward there were no significant differences between the group of patients who developed a postoperative complication and the ones who did not in terms of the three nutritional biochemical markers S-Albumin, S-Transthyretin and S-IGF-1. The mean postoperative length of stay was 10.6 days (SD 5.3) in the control group and 7.9 days (SD 4.3) in the intervention group, p = 0.012.
DISCUSSION
The result showed that S-IGF-1 was constant by increased energy intake within five days, while S-Albumin and S-Transthyretin decreased. Therefore, our findings confirms those of Lumbers et al. and Thissen et al., who stated that nutritional intake is important for the levels of circulating S-IGF-1 (1, 20) and that low protein and energy intake result in low S-IGF-1 levels (21, 22).
We used a short-term intervention and found that if patients stay only a few days at the ward, it was possible to follow their energy intake with S-IGF-1. Chevalley et al. found significantly higher levels of IGF-1 after one week of protein supplementation in female hip fracture patients, although the study was not performed directly postoperatively (23). Our study confirms these results. Tidermark et al. who used a long-term, six-month intervention with protein-rich supplements in hip fracture patients, reported significantly increased S-Albumin levels but no increase in the levels of S-IGF-1 at follow-up (24). This could be compared with the results from Schurch et al., which reported that the S-Albumin levels remained stable when the patients were given nutritional supplements for six months (14). The results from the present study indicate that Albumin may not be a useful biochemical marker for evaluating a five-day nutritional intervention. Mears used transthyretin as a biochemical marker at admission to hospital and once to twice a week to follow the patients' nutritional status when the patients were given nutritional supplements (25). However in our study we found that transthyretin was not affected within five days and might not be useful as a short-tem nutritional biochemical marker.
Because S-IGF-1 decreased significantly in the control group and did not change significantly in the intervention group, S-IGF-1 does not seem to be affected by inflammation status and the fracture event, as S-CRP increased significantly in both groups. However, S-Albumin and S-Transthyretin decreased significantly in both groups, a finding that indicates that S-Albumin and S-Transthyretin might be affected by the inflammatory response caused by the injury and the subsequent surgery. Thus, the present study indicates that S-IGF-1 was not affected by the fracture and the normal inflammatory response following trauma, per se, as previously shown for S-Albumin (11, 12).
The results showed that it was not possible to predict short-term postoperative complications within five days after surgery by assessing the nutritional biochemical markers S-IGF-1, S-Albumin or S-Transthyretin in hip fracture patients. However, a study by Gunningberg et al. found S-Albumin levels, but not S-IGF1, to be predictive for surgical wound infection 30 days postoperative in elective patients with hip- or knee-replacement or coronary bypass graft surgery (1717). They concluded that S-Albumin was not a biochemical marker specific for nutritional status, but could be influenced by illness and inflammation. In our study, the detailed analysis with only women showed that the control group had more complications than the intervention group.
Today IGF-1 is not used as an analytic tool clinically, mainly because it is considered to be too expensive (17 € in our laboratory), while Albumin is low price analytical tool (2 €) and Transthyretin is moderate-price one (11 €). IGF-1 could be useful to identify patients who did not fulfil their energy requirement during the hospital stay, thus needing additional nutritional attention after discharge or during rehabilitation, but more research is warranted.
METHODOLOGICAL CONSIDERATIONS
In this study, we registered each patient's nutrient and liquid intake daily, from admission until five days postoperatively. All nurses at the ward received education in nutrient and liquid registration, and the hospital kitchen provided guidelines for the energy content of each meal. We also had biochemical assessments from the day of admission and postoperative day five. S-Albumin, P-Transthyretin and S-IGF-1 are known nutritional biochemical markers often used both in clinical practice and for research purposes, and the levels in the blood samples of those markers are clearly objective. The biochemical analyses are standardised and reliable and performed at a certified laboratory. However, the cut-off value for every biochemical marker is a compromise between specificity and sensitivity, and there are no universally accepted cut-off levels for IGF-1, Transthyretin or Albumin in regard to malnutrition assessment. This is, nonetheless, not of major concern when evaluating concentration changes during a dietary intervention as we did in our study.
Fifty-eight potential patients (36.7%) were not included in the study. A retrospective evaluation of the demographic data for those patients, and the causes for exclusion, did not reveal any systematic cause for those patients' not being included. The nutritional intervention increased the patients' energy intake significantly, showing very good compliance with the intervention.
The best study design would have been a randomised-controlled trial. However, according to our assessment when designing the study, we foresaw that such a study design would have caused ethical problems at the ward, as some patients then would have been given nutritional supplements while other patients would have been kept on a regular diet and one from each group might share room. The design used in the present study was therefore chosen as it was considered to be the next-best alternative.
CONCLUSION
The results of our study showed that S-IGF-1 could be used as a short-term nutritional biochemical marker in patients with hip fracture, as it was affected by a five day high-energy intake, while S-Albumin and S-Transthyretin was not affected. S-IGF-1 is less affected by the acute trauma and the associated inflammation than S-Albumin and S-Transthyretin. S-IGF-1 could be a valuable complement to record patient's nutritional intake. S-IGF-1, S-Albumin and S-Transthyretin were not useful in predicting postoperative complications within five days postoperatively in hip fracture patients. However they all indicate the preoperative nutritional status of the patient.
Footnotes
ACKNOWLEDGEMENTS
Financial support from Uppsala University Hospital and Department of Orthopaedics at Uppsala University Hospital. Thanks to all nurses at the ward for collecting the data and especially to the head nurse Susanna Ingendoh-Husevik.