
Abstract
Background and Aims:
Obesity has been linked to the development of osteoarthritis of the knee and since the incidence of obesity is increasing, the need for total knee arthroplasty (TKA) is likely to increase. Conflicting findings have been reported concerning the relationship between obesity and TKA. It has been shown in several studies, that obese patients have poorer clinical results after operation. On the other hand it has also been reported similar results for obese and non-obese patients. The purpose of this study was to analyze clinically and radiologically the results of total knee artrhoplasty in obese patients.
Material and Methods:
The study consisted of 48 patients who had a TKA. The patients were divided in two groups according their body mass index. Patients of BMI over 30 were regarded as obese.
Results:
The obese patients had poorer clinical success at the final follow-up, their WOMAC scores were significantly higher compared to non-obese (pain 20.7 vs. 11.6; p = 0.021, stiffness 26.9 vs. 13.4; p = 0.006, physical function 26.5 vs. 14.4; p = 0.003). Differences were also found in the Knee (KS) and Function (FS) scores and a long-term postoperative ROM and (KS: 83.6 vs. 88.9; p = 0.01, FS: 63.6/76.3; p = 0.051, ROM: 104.6 vs. 109.6; p = 0.016). Non-obese patients reached better percentage improvement in the KSS compared to obese patients (KS change + 194.5% vs. + 59.5%, p = 0.03; FS change + 51.5% vs. + 14.9%, p = 0.19).
Conclusions:
Obesity has a negative impact on the outcome of TKA, assessed by patients' clinical function and satisfaction level.
INTRODUCTION
Osteoarthritis is a common joint disorder in the elderly and total knee arthroplasty (TKA) is generally considered to be a cost-effective and reliable method for the treatment of knee osteoarthritis (1,2) Obesity has been linked to the development of osteoarthritis of the knee and since the incidence of obesity is increasing, the need for TKA is likely to increase (3,–5). It seems that the role of obesity in this process is mechanical rather than systematic (6)
Conflicting findings have been reported concerning the relationship between obesity and TKA. It has been reported that obese patients have poorer functional outcome and a higher revision rate after total knee arthroplasty (7,8) found that patients' comorbidities such as obesity significantly affected postoperative infection risk. On the other hand, some studies have reported similar results for obese and non-obese patients (9,–11) showed in their study that obese patients indeed had lower function and knee scores, but at the same time a high percentage of these patients were satisfied with their knees after operation. The purpose of this study was to analyze clinically and radiologically the results of total knee arthroplasty in obese patients.
PATIENTS AND METHODS
Between May 1997 and May 2000, 95 total knee arthroplasties were performed, for randomly selected 85 patients who qualified inclusion criteria: no previous knee or hip operations, no medication or diseases known to influence bone mineral metabolism, in the department of the Orthopaedics and Traumatology, Kuopio University Hospital. Two other TKA studies were conveyed at the same time and those patients were not accepted. After obtaining the approval of the ethics committee of the University of the Kuopio, the current study continued March 2009 by inviting the all living patients to follow-up examination. 18 patients had died (1997–2009) during the follow-up, in addition 27 patients were not able to participate because of different reasons (unfit n = 8, change of residence n = 2, cancelled without stating reason n = 17). 16 of these 23 patients were women and 7 were men, and the mean BMI of this drop out group was 30.3 kg/m2 (Women: 32.0 kg/m2, Men 26.5 kg/m2). The final follow-up cohort consisted of 48 TKA patients and 52 knees. A minimum of follow-up period was nine years (mean 10.8 years, range 9–12 years).
Four knee implant designs from four manufacturers had been used: AMK (n = 8) (DePuy, Warsaw, IN, USA), AGC (n = 2) (Biomet Merck, Limited, Bridgend, South Wales, UK), Duracon (n = 25) (Stryker, Howmedica, NJ, USA) and Nexgen (n =
The clinical and radiological evaluations were performed preoperatively, and at the follow-up visits (1-year postoperatively and April 2009). The clinical evaluations included The Knee Society clinical rating system (KSS) which contains two components of assessments (Knee score (KS) for assessing knee and prostheses and Function score (FS) for patient's function) with a maximum of 100 score for each (12). The knee score evaluates pain, range of motion (ROM) and knee stability, the function score evaluates walking distance, ability to climb stairs and the need for the ambulatory supports. The clinical evaluation also included Western Ontario and McMaster Universities Osteoarthritis index (WOMAC) (13), and the Timed- Up-and Go-test (14). Detailed medical examination and interview were also performed. The WOMAC included 24 questions in three classes (Pain, Stiffness and Physical function). The patients were given a VAS (visual analogue scale)-version of the WOMAC on scale from 0 mm (no pain, stiffness or disability in physical function) to 100 mm (severe pain, stiffness or disability on physical function), and sum of scores were calculated within all classes. The aggregate scores for each dimension were calculated as an average within all three classes. In the Timed Up- and Go- test, patient is sitting on a chair at first and gets up after received a sign, walks 3 meters and then turns around, returns to the chair and sits down. The time from leaving the chair to returning back until being seated again was measured. This test assesses the patient's postoperative walking ability and balance. The duration of the operation (min), postoperative bleeding (ml) and hospital stay was also recorded (days).
The long antero-posterior weight-bearing and short lateral radiographs of the lower limb were performed preoperatively and postoperatively (1-year, April 2009). The alignment of the knee was evaluated and the degree of deviation of the mechanical axis was defined as the angle between a line from the femoral head to the centre of the knee joint and the line from the knee joint to the centre of the ankle. A deviation of within ± 3 degrees from neutral was determined to be a good and acceptable outcome (15). Patients' characteristics (both preoperative and postoperative) including age, gender, medication, smoking, chronic diseases and body mass index (BMI) were recorded from the medical case records and during clinical examination. The postoperative complications were recorded.
The patients were divided into two study groups according to body mass index (BMI). BMI was calculated by dividing person's weight in kilograms by their weight in meters squared (kg/m2). BMI was categorized as non-obese (Group 1) and obese (Group 2). The Group 1 consisted of patients whose body mass index was < 30 kg/m2 (non-obese, n = 26 preop/1-year; n = 23 spring 2009) and the patients with BMI ≥ 30 kg/m2 belonged to the Group 2 (obese, n = 22 preop/1-year; n = 25 spring 2009). A total of five patients in the primary group 1 had gained and two patients in the primary group 2 had reduced their weight over the categorize line, during the mean of 10.8 years follow-up.
STATISTICS
Statistical analysis was performed using the SPSS 17.0 software. Standard descriptive statistics were calculated for the study population. Mann-Whitney test was used to evaluate group differences in continuous variables with non-normal distribution and Wilcoxon's signed-rank test was used for the case of repeated measurements. The analysis for categorical parameters was performed with Pearson's chi-square test. Correlation between patients' age and continuous variables in follow-up outcome at April 2009 was considered by using Spearman's non-parametric correlation matrix. P-value of < 0.05 was considered significant.
RESULTS
A total of 85 patients underwent primary TKA during 1997–2000 and at the time of final control examination 48 patients (40 women and 8 men) were able to participate in the study. All the patients had knee osteoarthrosis as an indication for the operation. For three women and one man also contralateral knee arthroplasty operation had been carried out during 1997–2000, thus the total number of knees in this follow-up was 52. There were 43 knees with preoperative varus deformity (mean 10.3°, SD 5.4) and 9 knees with preoperative valgus deformity (mean 7.7°, SD 4.5). The mean age of the patients at the time of follow-up examination (April 2009) was 76.3 years (54–90, SD 6.7).
There was no statistically significant difference between women and men in preoperative or postoperative functional results (Table 1). At the follow-up, age correlated weakly with the Knee Score, Function Score, ROM-value and walking distance (r = −0.28; p = 0.058, r = −0.39; p = 0.007, r = −0.11; p = 0.47, r = −0.34; p = 0.017, respectively). The age had positive correlation with WOMAC pain-, stiffness-, physical function- scores and Up- and Go- test (r = 0.19; p = 0.20, r = 0.30; p = 0.040, r = 0.22; p = 0.14, r = 0.51; p = 0.001).
The preoperative and follow-up characteristics in women and men, expressed as mean (SD).
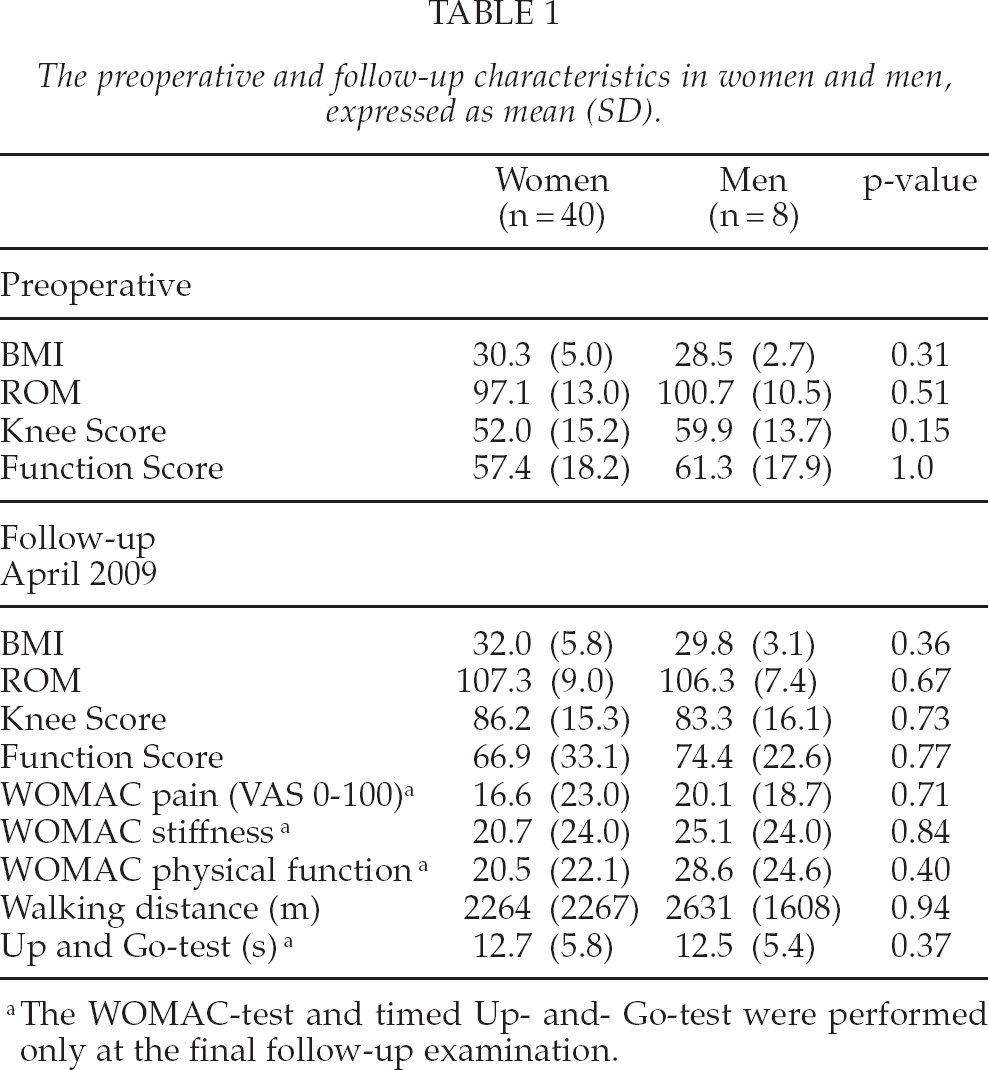
The WOMAC-test and timed Up- and- Go-test were performed only at the final follow-up examination.
The mean BMI was 30.0 kg/m2 (21.2–40.90, SD 4.7) preoperatively, increasing up to 31.6 kg/m2 (21.4–45.0, SD 5.5) in 2009. A total of 21 patients had a chronic disease (one or more of following: hypertension, cardiac illness, non-insulin diabetes) needing medication preoperatively. At the time of final follow-up in spring 2009, a total of 40 patients were suffering by chronic disease.
The prevalence of the preoperative chronic diseases did not differ between the study groups (Group 1, n = 10 vs. Group 2, n = 11; p = 0.42). Statistically significant difference was noticed when comparing the prevalence of chronic diseases between the groups in April 2009 (Group 1, n = 16 vs. Group 2, n = 24; p = 0.014).
The functional and radiological results between the non-obese (Group 1) and obese (Group 2) patients did not differ preoperatively. At 1-year follow-up Function score and ROM were significantly lower in the obese patients (Table 2).
The preoperative and 1-year postoperative functional and radiological results per knee, expressed as mean (SD).
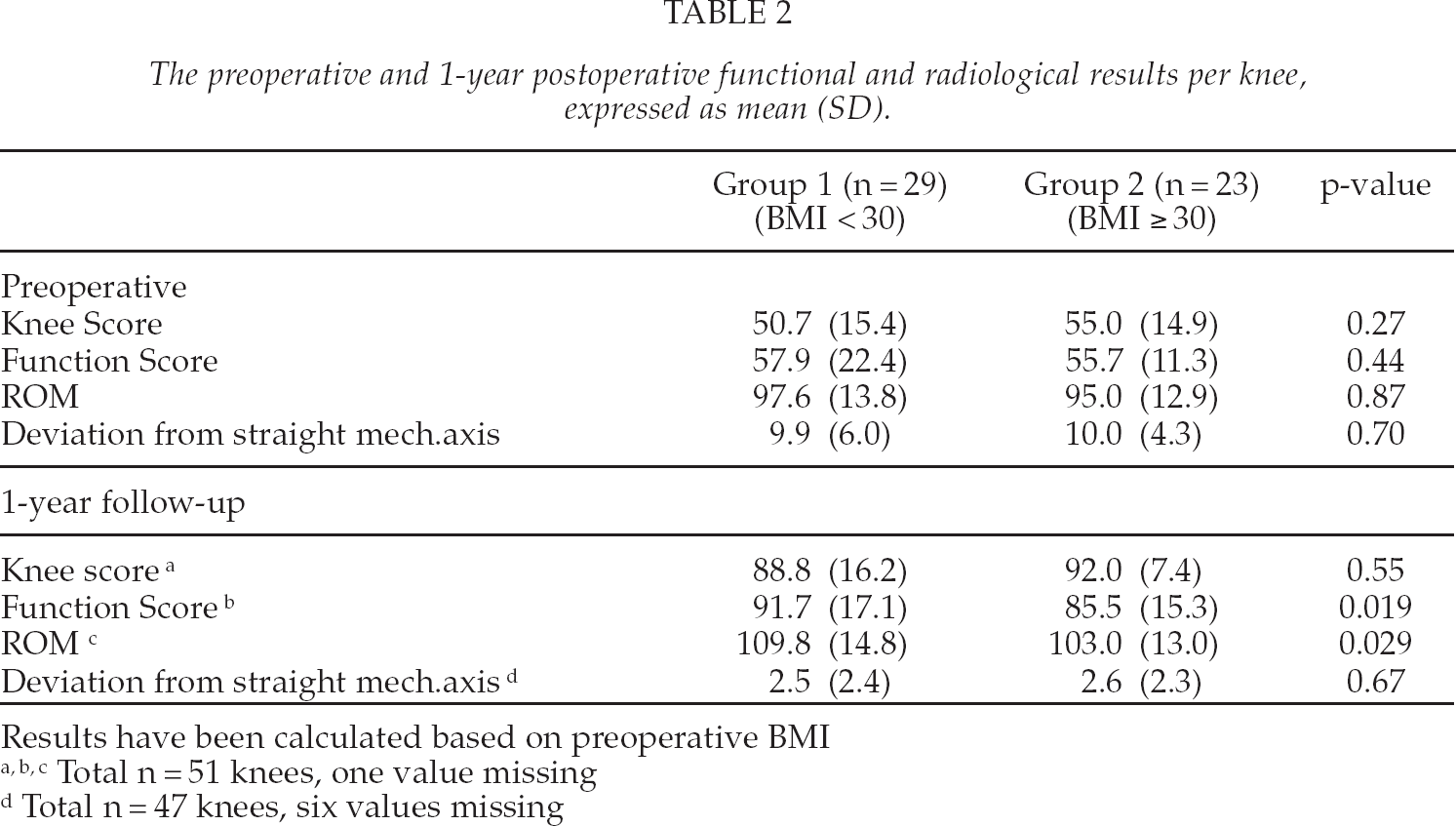
Results have been calculated based on preoperative BMI
Total n = 51 knees, one value missing
Total n = 47 knees, six values missing
At the final follow-up in April 2009, the obese patients had significantly lower Knee and Function scores, ROM-values and WOMAC-scores (Table 3). The deviation from the straight mechanical axis was at least 3 degrees in 11 patients in the Group 1 and in 12 patients in the Group 2, p = 0.42. There was no difference in the use of ambulatory support at the final control examination (Group 1, n = 8/Group 2, n = 8; p = 0.84).
The postoperative functional, radiological and subjective results at the follow-up examination in April 2009 per knee, expressed as mean (SD).
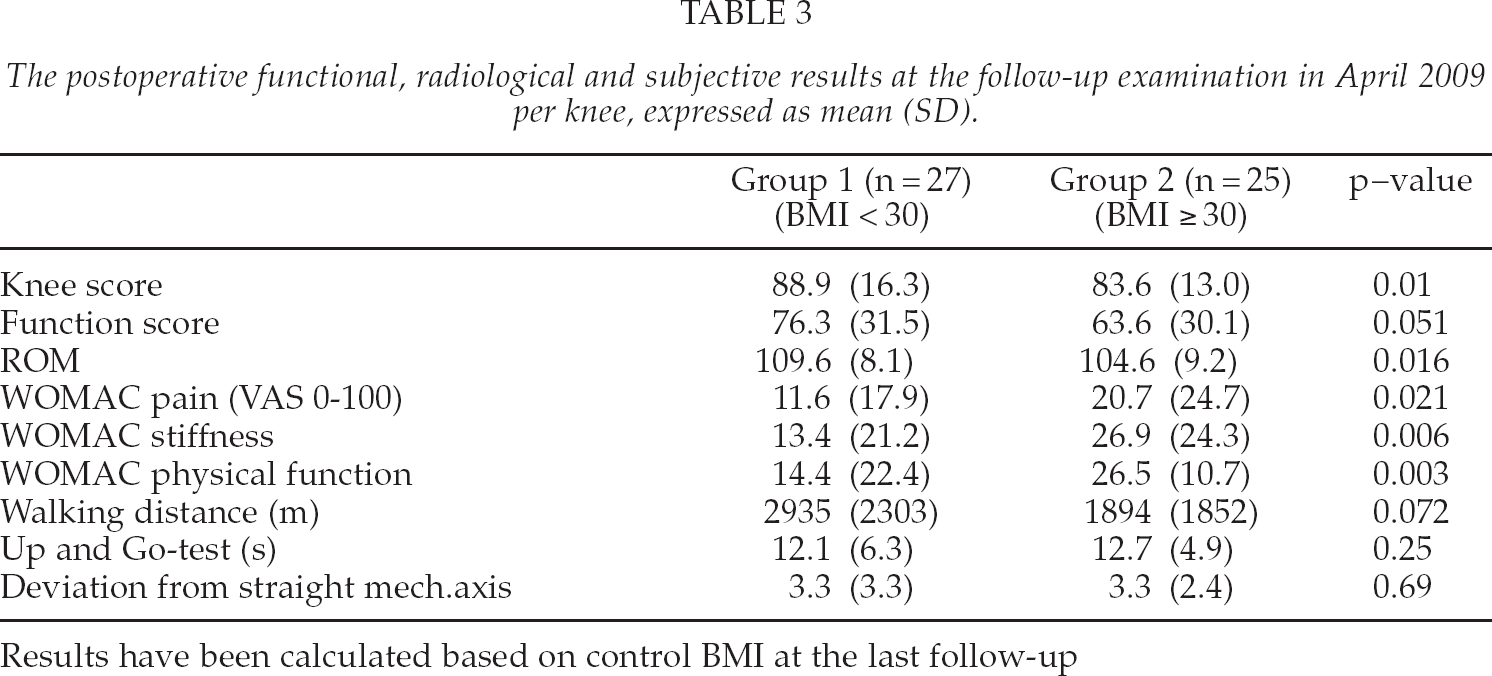
Results have been calculated based on control BMI at the last follow-up
Altogether six (early or late-onset) postoperative complications (three in both study group) [wound infection: Group 1 (BMI < 30), n = 0 vs. Group 2, n = 1, prosthesis infection n = 1 vs. n = 2, respectively, venous thrombosis of the lower limb or cement body in the joint as a technical error (n = 2 vs. n = 0, respectively, p-value of the number of the total of the post. op. complications p = 0.22 were found among whole study cohort, of 48 patients. There were no significant difference in complications or revision rate between the study groups during the follow-up (Group 1, n = 3 vs. Group 2, n = 3; p = 0.83) and there were no significant difference between groups either in operation time (Group 1: 120, Group 2: 112; p 0.13), postoperative bleeding (460/436, p = 0.95) or postoperative hospital stay (6.0/5.8, p = 0.98).
The patients in both study groups reached a clear improvement in the Knee and Functional scores during the first study interval (preoperative −1-year follow-up, Group 1 ΔKS = 38.3, Group 2 ΔKS = 36.1; p = 0.70/ΔFS = 35.6 vs. 30.8, respectively; p = 0.55), but the scores decreased during the second interval (1-year—final control at 2009, Group 1 ΔKS = −0.3, Group 2 ΔKS = −8.5; p = 0.32/ΔFS = −15.8 vs. ΔFS = −24.6; p = 0.36). The decline was more remarkable in Function scores in both groups, and the decline (Knee score and Function score) tended to be higher in the Group 2. The patients in Group 1 achieved higher numerical values in the change of total Knee and Function scores, but difference between study groups was not significant. The mean percentage change of the Knee scores during follow-up in the Group 1 was + 194.5% and + 59.5% in the Group 2 (p = 0.030). The mean percentage change of the Functional scores was + 51.5% and + 14.9% (p = 0.19), respectively. The mean percentage change of the ROM during follow-up was + 16.7 percent in Group 1 and + 8.5 percent in Group 2 (p = 0.13) (Fig. 1). These values are available in 41 patients (and 44 knees) because those patients whose BMI-values had changed over the categorize line (< 30, ≥ 30 kg/m2) were excluded from this analysisa.
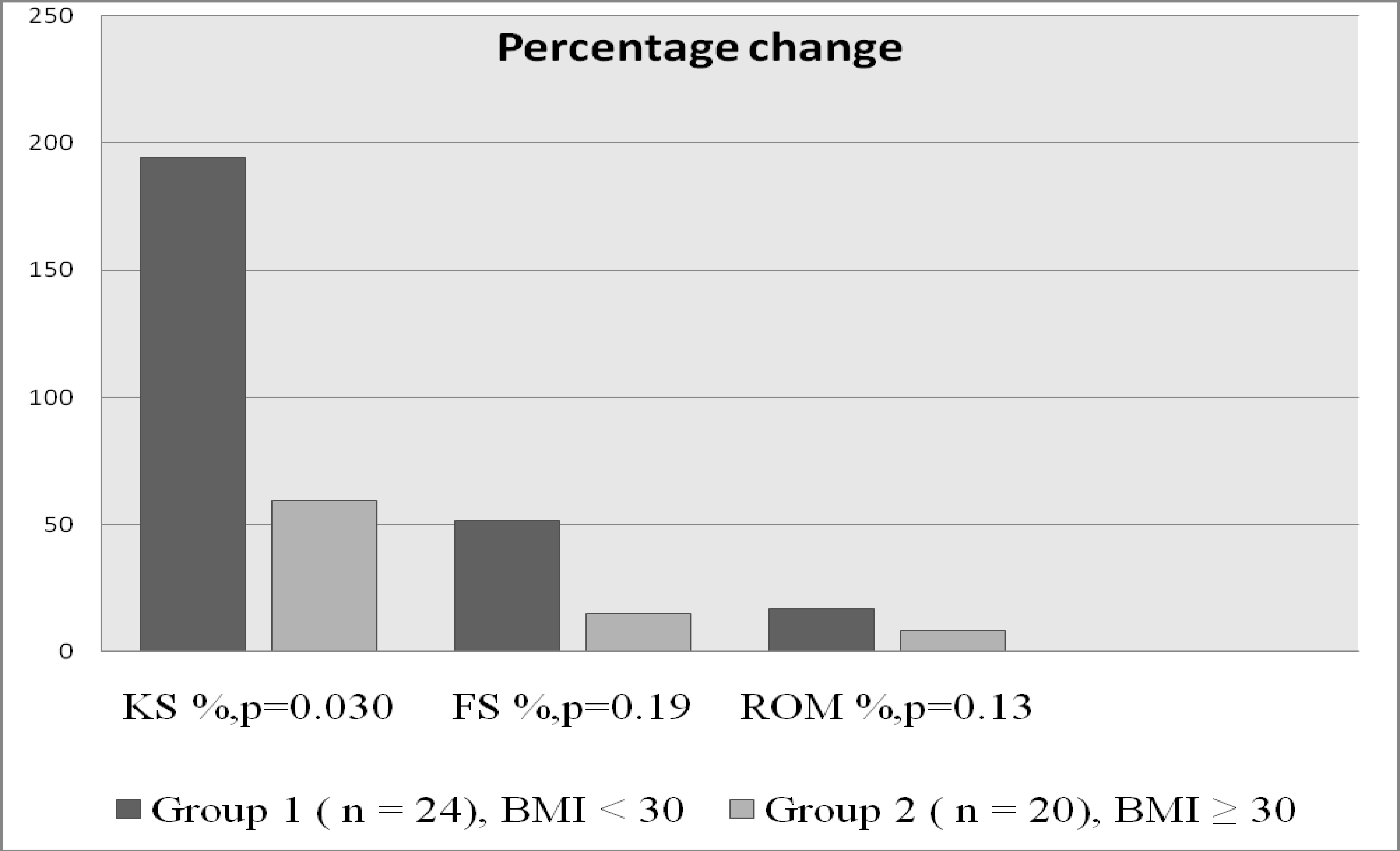
The percentage change of Knee (KS) and Functional scores (FS) and ROM-values between the study groups during follow-up period.
DISCUSSION
Obesity and over-weight have been increasing worldwide during the past twenty year (16,17). It has also been shown that obese persons seem to be over-represented among the patients needing common orthopaedic operations such as total knee arthroplasty (18). The results of our current study suggest that obesity has a negative effect on the functional and subjective outcome of total knee arthroplasty. At baseline the preoperative characteristics were similar for obese and non-obese patients, but at a mean of 10.8 years follow-up, obese patients reached poorer success in the KSS and the ROM values, but the preoperative values between the study groups were convergent. The self-assessed WOMAC scores were also significantly lower in the obese group. Our findings are in agreement with those of several previous studies. Foran et al. (19) concluded in their study with 87 knees that any degree of obesity has a negative impact on the outcome of TKA: they found that there was a significant difference in the postoperative Knee Society scores between non-obese and obese patients. Jackson et al. (20) reported that obese patients had significantly lower mean improvement in clinical scores after TKA measured by using The Hospital for Special Surgery Knee Rating Score system (HSS).
Obesity has also been shown to increase the risk of postoperative complications after knee replacement surgery. Amin et al. (21) concluded in their study of 38 morbidly obese patients that results were inferior in this patient group, as demonstrated by inferior Knee Society scores and higher rate of complications. Winiarsky et al. (22) found that morbid obesity is associated with an increased rate of perioperative complications including problems with wound healing and infections. In this study, we found no difference between obese and non-obese patients in complication rate or revision rate.
Several studies assessing outcome after TKA have reported differing findings. Stickles et al. (23) found no difference between obese and non-obese regarding patients' satisfaction assessed by WOMAC. Spicer et al. (9) found that the revision and survival rates were comparable between non-obese and obese patients over the first follow-up decade.
The current study also found a decline in the Knee Society scores during the follow-up in both groups, and the rate of decline being higher in the Function scores than in the Knee scores. Malkani et al. (24) found in their ten year follow-up study that the Functional scores improved from a mean of 46 points preoperatively to a mean of 79 points at one year, but the scores decreased to a mean of 64 points at the latest evaluation. James et al. (25) also reported that the Knee and Functional scores improved after TKA operation, but at the last follow-up evaluation a statistically significant decline was noticed in the Functional scores. Patients' BMI showed no correlation with the postoperative scores. We found that the obese patients' rate of decline in both Knee scores and Function scores were higher, although not significant, and their percentage improvement in the scores was lower. Overall, this disparity in the Knee and Functional scores is difficult to explain, but it must be noted that obese patients' mean walking distance was also lower and walking distance contributes a half of the total Functional scores (without deductions).
This study has some limitations. Our study cohort was relatively small (48 patients and 52 knees), but the small size of the study population also reflects the age distribution of these patients. Over time, a loss of study population is inevitable. Further, not all clinical measurements were used preoperatively. The strengths of our study are the long follow-up time and comprehensive clinical and radiological measurements.
In conclusion, obese patients had poorer clinical success at final follow-up. Womac scores were significantly higher in obese patients. There were also differences in Knee score, function score and range of motion. The authors conclude that obesity has a negative effect on the outcome of TKA.
Footnotes
ACKNOWLEDGMENTS
We would like to thank statistician Vesa Kiviniemi for his assistance in this study.