
Abstract
Background and Aims
Endoscopic retrograde cholangiopancreatography (ERCP) is a procedure with a risk of serious and life-threatening complications. The most common complications are pancreatitis, haemorrhage, perforation and cholangitis. The aim of this study was to determine indications, success rates and complications in a low-volume ERCP unit in Kanta-Häme Central Hospital (KHCH).
Material and Methods
Data on 1207 consecutive ERCPs performed in KHCH between 2002 and 2009 was collected retrospectively from patient histories. Complications were classified according to need for intervention and length of hospitalisation.
Results
Cannulation of the desired duct was successful in 89.2% of 825 ERCPs with no earlier sphincterotomy. Complete stone removal was achieved in 91.3% of procedures. Standard biliary sphincterotomy was performed in 73.8% and precut sphincterotomy in 12.0 % of cases. Cholangitis developed in 2.1%, bleeding in 1.9%, pancreatitis in 1.9%, perforation in 1.0% and cardio-pulmonary or miscellaneous complications in 4.2% of cases. The majority of complications could be managed conservatively. In procedures with no earlier sphincterotomy ERCP-related 30-day mortality was 0.2% (n = 2) and overall 30-day mortality was 3.3% (n = 27).
Conclusions
ERCP indications and success rates, as well as morbidity and mortality were comparable to those reported earlier. Although the success rate of cannulation and thereby ERCP procedures seem to be somewhat lower than in tertiary referral centres, ERCP procedures can be safely performed in a low-volume ERCP unit by concentrating procedures on a few experienced endoscopists. The success rates may be further improved with the latest cannulation techniques, used selectively in the last years of the study period.
Keywords
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is used in the treatment of benign and malignant pancreatic and biliary diseases. It is a demanding procedure with a long learning curve and a risk of serious and life-threatening complications. The most common indications of ERCP are removal of common bile duct (CBD) stones and relieving bile duct obstruction by stent insertion. Diagnostic procedures should be avoided, because they can be mostly replaced by non-invasive magnetic resonance imaging (MRI) or endoscopic ultrasound. The main complications are pancreatitis, haemorrhage, cholangitis and perforation of the CBD or duodenum (1, 2). Several studies, most from large academic centres have reported a low incidence of complications (3 –17). In Finland ERCPs are also widely performed in low-volume community hospitals. The quality indicators of ERCP practice include adequate indications and low complication figures as well as success rate of cannulation (18). The cannulation of the desired duct should be successful in over 85% of ERCPs (18), but success rates as high as 98% have been reported (19, 20, 21). In this study, our aim was to retrospectively investigate indications, success rates and complications of ERCPs in a low-volume community hospital.
MATERIAL AND METHODS
The hospital database was searched for ERCPs performed between 1 January 2002 and 31 December 2009 in the endoscopy unit of Kanta-Häme Central Hospital (KHCH) in Hämeenlinna. KHCH is a medium-sized community hospital in southern Finland serving a population of 173.000. All procedures were performed by two experienced endoscopists. All complications were managed in our hospital except one patient with cholangitis and suspected duodenal perforation. Thirty-three procedures were excluded because papilla Vateri could not be reached (for reasons related e.g. to duodenal obstruction or inadequate sedation). Retrospective chart review was continued for up to 30 days after the procedure or to the end of longer hospitalisation. Patient status after 30 days could be confirmed in 91.5% of ERCPs. Olympus duodenoscopes were used in all ERCPs. The cannulation techniques evolved during the study period. A primary method of entering the bile duct was to use sphincterotome or to cannulate over guide wire inserted in the CBD. In the early years of the study period, the guide wire cannulation was not routinely used and some cannulations had to be done with a little contrast medium injection to the pancreatic duct as access to CBD was attempted. When necessary, a precut sphincterotomy was performed with a needle knife towards 11–12 o'clock to expose the CBD. Selectively, in the last few years a pancreatic sphincterotomy technique was used in which precut was directed towards pancreatic duct. Some of the CBD cannulations were performed with a double-guide-wire technique (i.e. an another guide wire inside the pancreatic duct). CBD stones were extracted by balloon catheter or basket.
During the last two years of the study period, a routine antibiotic prophylaxis (i.v. cefuroxime 1.5 g) was administered. Before this, antibiotics were given selectively if a stent insertion was planned or if a patient had a bile duct obstruction or an acute infection. The patients were given i.v. sedation (midatsolame or propofol) in the last three years of the study period administered mainly by an anaesthetist. In the earlier years, sedation and monitoring were managed by the endoscopy team and only i.v. midatsolame was used. Duodenal peristalsis was reduced by i.v. hyoscine butylbromide or i.v. glucagon. Procedures were classified as therapeutic when sphincterotomy, stone removal, stent insertion or removal, brush cytology or dilatation was performed. Routine serum blood samples after 6–10 hours included WBC count, haemoglobin, CRP and amylase. Each patient was followed up in our hospital for at least 24 hours after ERCP.
Complications were classified using the standardised criteria proposed by Cotton et al. (22). A complication was defined as any adverse event occurring during the 30-day period after ERCP requiring more than one night of hospitalisation. Severe complications required more than ten days of hospitalisation, necessitated surgical or invasive radiologic intervention, required admission to the intensive care unit (ICU) or caused patient's death. We compared the age, sex, history of diabetes, use of anticoagulation treatment, long-term corticosteroid use and the procedure related factors (e.g. precut) to mortality and morbidity to find significant risk factors. The grade of procedure difficulty and complexity was defined by the criteria published earlier (23).
Statistical analysis was performed using IBM SPSS Statistics 19.0. Categorial variables were compared using Chi-square test and calculating odds ratios and their 95 % confidence intervals. A probability of < 0.05 was regarded as significant. The study protocol was approved by ethics committee of KHCH.
RESULTS
A total of 1207 consecutive ERCPs were performed to 809 patients. Papilla was intact i.e. no earlier sphincterotomy had been performed in 68.4% (n = 825) of procedures. In these procedures 61.1% of patients were females and the median age was 70 years (range 17–101). The cannulation of the desired duct was achieved in 89.2% (n = 736) of the procedures with intact papilla in the first ERCP session of the study period. Complete stone extraction was successful in 91.3% and bile duct obstruction could be relieved completely in 80.1% of procedures with intact papilla. Of all 1207 ERCPs performed, 80.9% were therapeutic, 11.7% diagnostic or without therapeutic interventions and in 7.4% cannulation was unsuccessful.
The most common indications were CBD stones or bile duct obstruction caused by malignancy (Table 1). Of ERCPs with intact papilla, precut was performed in 12%, standard sphincterotomy in 73.8%, CBD stone removal in 33.7%, brush cytology in 11.8% and stricture dilation in 8.1% of procedures. A biliary stent was inserted for malignant stricture in 11.4% and for other reasons in 3.3% of ERCPs. A pancreatic stent was inserted in 0.6% and pancreatic stone was extracted in 0.5% of primary procedures. Pancreatography was performed or contrast medium was observed in the pancreatic duct in 47.8% of ERCPs with intact papilla and in 38.8% of all procedures. Of all 1207 procedures a biliary stent exchange was performed in 7.6% of ERCPs.
Indications or work-up diagnosis of 825 ERCPs with intact papilla
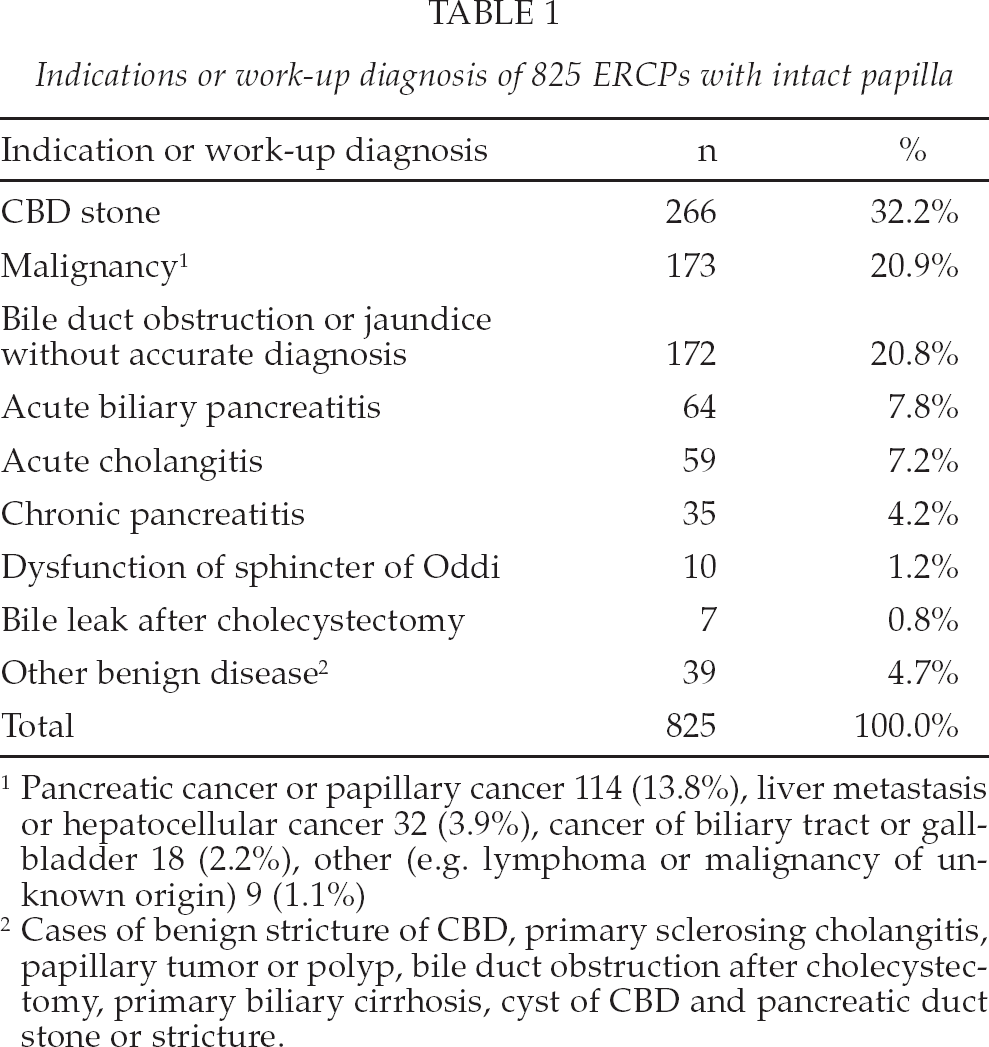
Pancreatic cancer or papillary cancer 114 (13.8%), liver metastasis or hepatocellular cancer 32 (3.9%), cancer of biliary tract or gallbladder 18 (2.2%), other (e.g. lymphoma or malignancy of unknown origin) 9 (1.1%)
Cases of benign stricture of CBD, primary sclerosing cholangitis, papillary tumor or polyp, bile duct obstruction after cholecystectomy, primary biliary cirrhosis, cyst of CBD and pancreatic duct stone or stricture.
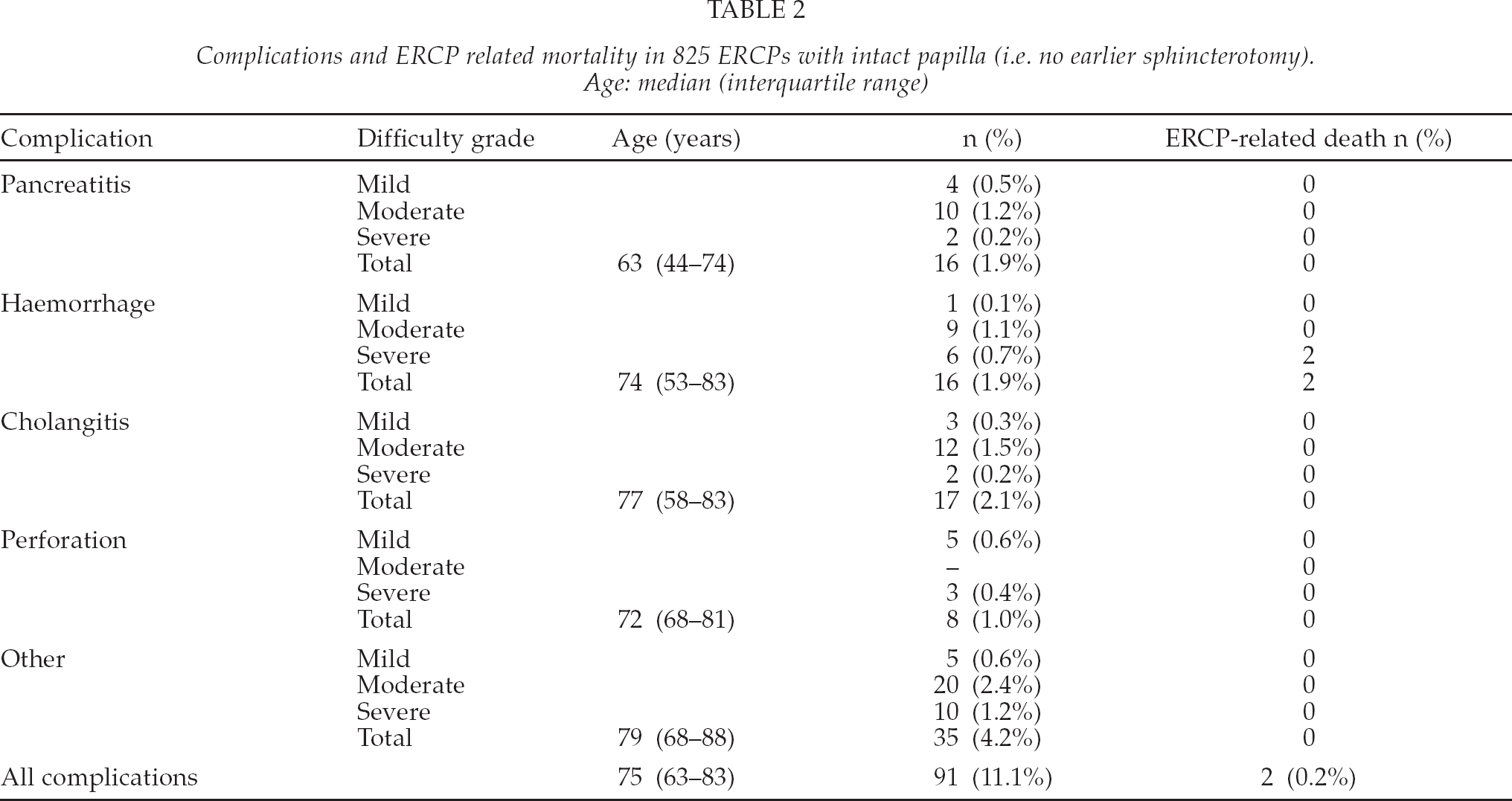
Complications and ERCP related mortality in 825 ERCPs with intact papilla (i.e. no earlier sphincterotomy). Age: median (interquartile range)
The complexity and difficulty level of completed ERCP procedures were graded by a three-step classification. ERCPs with intact papilla fell into categories I, II and III respectively as 79%, 19% and 2%. No connection between the level of difficulty and complications was found.
Of all ERCPs, 8.7% were planned second attempt procedures 2–14 days after an incomplete or failed procedure. These included cases where an earlier attempted ERCP had failed or had been intentionally aborted after performing precut sphincterotomy in a difficult cannulation.
Overall complication rate was 11.1% in procedures with intact papilla (Table 2) and 9.8% in all ERCPs. The majority of the complications (77 %) were mild or moderate i.e. they were managed conservatively and necessitated less than ten days of hospitalisation. No statistically significant risk factors for overall complications were found.
PANCREATITIS
Pancreatitis occurred after 16 (1.9%) of procedures with intact papilla. Two of these were severe and required operation. Both were caused by a therapeutic procedure. None of the patients died of pancreatitis. After precut sphincterotomy, pancreatitis of any degree was noted in six (5.6%) cases and after standard sphincterotomy in 11 (1.8%) cases, but the difference was not statistically significant (NS). Precut was a risk factor of moderate or severe pancreatitis (OR 3.8, 95% CI 1.1–12.8, p 0.022). Patient's sex, diabetes, medication or contrast injection to pancreatic duct during ERCP did not affect the risk of pancreatitis. In patients under 50 years of age pancreatitis developed in five cases (3.4%) and in 11 cases (1.6%) in older patients (NS).
HAEMORRHAGE
Haemorrhage was present after 16 (1.9%) ERCPs with intact papilla. Half of these (50%) were treated with re-duodenoscopy to achieve haemostasis. Two patients died of ERCP-related haemorrhage. Bleeding resulted after four (4.0%) procedures with precut sphincterotomy and after 13 (2.1%) of those with standard sphincterotomy (NS). All ERCPs that caused moderate or severe bleeding were therapeutic. None of the patient or procedure related factors (e.g. age, use of anticoagulation treatment, sphincterotomy, precut) were related to the incidence of hemorrhage.
CHOLANGITIS
Seventeen (2.1%) patients developed cholangitis after ERCPs with intact papilla. One patient was treated surgically for a suspected duodenal perforation. Both cases of severe cholangitis developed after therapeutic procedures. No risk factors for cholangitis were found.
PERFORATION
Perforation was observed in eight (1.0%) patients. Most of the perforations (75%) were retroperitoneal and were noticed during the endoscopy (75%). None of the cases were caused by a duodenoscope. Three patients required surgery. All cases of moderate or severe perforations were preceded by a therapeutic ERCP. Perforation occurred in two (2.0%) procedures with precut sphincterotomy and in four procedures (0.7%) with standard sphincterotomy (NS). Patient or procedure related factors were not related to risk of perforation. Two patients of all of the 1207 ERCPs died after perforation.
OTHER COMPLICATIONS
Other morbidity or complications developed in 35 (4.2%) of ERCPs with intact papilla. These included seven (0.8%) patients with pneumonia, seven (0.8%) infections of unknown origin, six (0.7%) cerebral infarctions, four (0.5%) cardiac events and four (0.5%) cases with urinary retention or urinary tract infection. Two (0.2%) patients with cholecystitis were operated on. In addition, one case (0.1%) of each of the following events occurred: acute colitis, gastroenteritis, deep venous thrombosis, suspected pulmonary embolism, and haemorrhage from oesophageal varices. Age over 60 years was a risk factor of other complications graded moderate or severe (OR 3.6, 95% CI 1.1–12.0, p 0.027).
MORTALITY
The ERCP-related mortality in procedures with intact papilla was 0.2% (n = 2). Both cases resulted from hemorrhage. Overall mortality in 30 days was 3.3% (n = 27). Eighteen (2.2%) of these were caused by cancer and seven (0.8%) by other, non-ERCP-related adverse events. These seven deaths consisted of two cases of pneumonia, three cardiac events, a septic infection after insertion of a percutaneous transhepatic biliary drain and a haemorrhage from esophageal varices in a patient with severe liver cirrhosis. Age over 60 years was a risk factor of overall 30-day mortality (OR 11.8, 95% CI 1.6–87.4, p 0.002).
In all of the 1207 procedures, ERCP-related mortality was 0.4% (n = 5). Two patients died after perforation. In addition, the death of a 68-year old male in the ICU nine days after biliary stent insertion was considered ERCP-related. In autopsy, the cause of death was multi-organ failure of unknown origin.
DISCUSSION
Given that ERCP is a technically demanding invasive procedure with a risk of complications, ERCP practice should be critically evaluated in terms of indications, success rates and complications (18). Most of the earlier studies come from university clinics, whereas there are only few reports of complications in low-volume centres (10). Our objective was to describe ERCP-practice in a community hospital and to report success rates and complication figures that could be compared to earlier studies.
In our material 80.9% of all ERCPs were therapeutic and 11.7% were diagnostic or without need for intervention. In the earlier studies, the proportion of therapeutic ERCPs has ranged from 54.7% to 97.7% (7, 8, 10, 12, 13). Both the indications of ERCPs and the proportions of different biliary procedures were essentially similar to those described in earlier reports (6, 8 –12). The number of pancreatographies seems high, because it was defined as any amount of contrast medium in the pancreatic duct and not only as an intentional diagnostic filling of the duct. In the early years of the study period, as CBD was cannulated without a guide wire, a careful injection of contrast medium to pancreatic duct was sometimes unavoidable. In our study a pancreatic stent was inserted in 1.8% of all procedures and in 0.6% of ERCPs with intact papilla. No complications occurred after pancreatic procedures. In the earlier studies the proportion of pancreatic procedures varied widely, which may indicate differences in patient mix between centres. In the study by Williams et al. (9) pancreatic procedures accounted for 1.6% of ERCPs. In other reports, the proportion of pancreatic stent insertions has ranged from 5.5 to 9.2% of procedures (10, 11).
A three-step classification of procedure complexity has been used in a few earlier studies to control the effect of patient mix to complications (10, 11). More complex and more difficult procedures (grade III) have resulted more often in severe complications or mortality (11). The proportion of the most complex procedures was expectedly slightly lower than in larger centres (10, 11). In a retrospective setting, defining ERCP complexity may be unreliable. In our material, five patients were referred to the endoscopy unit of Helsinki University Hospital (HUS) because demanding pancreatic interventions were needed and in our unit even repeated attempts had not been successful.
We used precut sphincterotomy in 12% of ERCPs with intact papilla. This is slightly more than 8.5–10.0% in earlier studies (5, 6, 19, 21). In our material precut was a significant risk factor for moderate or severe pancreatitis. This concurs with findings showing both difficult cannulation and precut sphincterotomy to be risk factors of ERCP-related complications (5, 7, 8, 9, 12). On the other hand, properly timed precut sphincterotomy performed by an expert endoscopist makes it possible to complete the procedure endoscopically without risk of operative or percutaneous interventions (3, 4, 19, 20, 21). It has been suggested, that precut sphincterotomy should be used early enough in a difficult cannulation to avoid numerous cannulation attempts and unnecessary injury to the papilla or to the pancreatic duct. Early use of precut sphincterotomy may reduce the risk of pancreatitis (24, 25). The second cannulation attempt a few days after precut is usually easier (13, 19, 20).
In the last two years of the study period, we selectively used pancreatic sphincterotomy in difficult bile duct cannulation (21, 26, 27). This technique has been shown to enable bile duct cannulation relatively safely in up to 98.1% of cases (20). We did not use temporary pancreatic stenting to prevent ERCP-related pancreatitis (12, 27, 28, 29).
The success rate of cannulation and complication figures are usually reported from ERCPs with no earlier sphincterotomy. The cannulation of the papilla is easier and less risky if a sphincterotomy has already been done. In the present study the success rate of cannulation was 89.2% of ERCPs in which the papilla was intact and 92.6% of all ERCPs. Studies from academic centres have reported successful bile duct cannulation in 85.6–98.1% of cases (8, 9, 10, 12, 13, 19, 20, 21). However, in our study the proportion of planned second attempt ERCPs 2–14 days after aborted or failed procedure was 8.7% of all procedures. As far as we know, this figure has seldom been reported in other studies; in the study by Palm et al., the proportion of second attempt ERCPs was 3.0% (20). We have tried to avoid complications by converting a difficult cannulation attempt early enough into a precut sphincterotomy, followed by a planned second attempt ERCP a few days later. As our figures are per procedure, the definitive success rate per patient after repeated ERCPs remains unknown. In the other studies, repeat ERCP after precut sphincterotomy has been shown to enable successful cannulation ultimately in up to 96.0–98.2% of cases (19, 20). The success rates for extraction of CBD stone or relieving bile duct obstruction were similar to the results of Colton et al. in a community setting and to the published guideline (10, 18).
In our study the incidence of pancreatitis (1.9%) was lower than 2.6–7.2% reported earlier (3, 4, 6 –12, 21). According to the prospective studies, younger patients and patients under 60 years of age have been in increased risk of pancreatitis (4, 9, 12). In the earlier studies, the incidence of haemorrhage and cholangitis has been 0.3–2.0% and 0.3–1.4%, respectively (3, 4, 6 –12). The highest incidence of cholangitis has reportedly been up to 5% (8). Our results substantiate this. Some cases of haemorrhage could have been avoided, as some of the procedures were performed to extremely high risk patients as a palliative attempt to relieve e.g. malignant biliary obstruction. Perforation has occured in 0.1–1.1% of cases (3, 4, 6 –12). Our incidence was 1.0%. Other, e.g. cardio-pulmonary complications were slightly more frequent than 0.2–1.5% in recent reports (7 –12). On the other hand, in a large prospective Danish study with a thorough follow-up, the incidence of other complications was 5.1% with an overall complication rate of 15.9% (8). As noted in the earlier studies (7 –12), the majority of the complications was mild or moderate and could be managed non-operatively with a short hospitalisation.
The most of the mortality was caused by cancer or non-ERCP-related diseases. ERCP-related mortality in procedures with intact papilla (0.2%) was similar to figures of 0–1.0% of the earlier studies (8, 10, 11). In the reports from Finnish academic centres, ERCP-related mortality has been 0.1–0.3% (13, 14, 20). Overall mortality usually ranges from 1.4% to 5.8% (8, 10, 11), but this figure, as well as rate of overall morbidity, may be influenced to some extent by differences in patient follow-up and study design. Both non-ERCP-related complications and overall mortality were expectedly related to patient's age of over 60 years.
This study describes ERCP practice in a low-volume community hospital. The indications and success rates as well as morbidity and mortality are acceptable compared to those in earlier reports and published guidelines. Although the success rate of cannulation and thereby ERCP procedures seem to be somewhat lower than in tertiary referral centres, our results confirm that ERCP procedures can be safely performed in a low-volume ERCP unit. Adequate indications of ERCP and good procedure routine can be maintained, at least when procedures are concentrated on a few experienced endoscopists. Cannulation success rates reported from academic centers may be achieved using techniques, such as pancreatic sphincterotomy and cannulation with the double guide wire technique, that were used only in the last years of the study period.