
Abstract
Background and Aims
Longterm survival after curative resection for adenocarcinoma at the gastro-esophageal junction (GEJ) range between 18% and 50%. In the pivotal Intergroup-0116 Phase III trial by Macdonald et all, adjuvant chemoradiotherapy improved both disease-free and overall survival in curatively resected patients with mainly gastric adenocarcinoma. We compared survival data for curatively resected patients with adenocarcinoma solely at the gastro-esophageal junction (GEJ), treated with surgery alone or surgery and adjuvant chemoradiotherapy.
Methods
From 2003 to 2009, 211 patients underwent curative resection. Surgery alone was performed in 95 patients and 116 patients received adjuvant therapy after resection.
All patients underwent Lewis-Tanner operation with D1 node resection including coliac nodes (D1+). Informations about recurrence and death were collected from the Danish Cancer Register and the Central Death Register. Patients who died after experiencing severe complications after surgery were excluded from the survival analysis. Patients with T0N0 or T1N0 were also excluded because patients of this category were not given adjuvant therapy according to the Macdonald protocol.
Results
Patients with positive node status in the resected specimen, the 3-year disease-free survival after adjuvant chemoradiotherapy (n = 91) or surgery alone (n = 43) was 24% and 37%, respectively. Median time of survival was prolonged by 10 month in favour of those who received chemoradiotherapy. However, after controlling for the confounding effect of age and node status, only positive node status in the resected specimen had significant partial effect on survival.
Conclusion
Chemoradiotherapy according to the Intergroup-0116 protocol might still be a reasonable option after curative resection in patients with GEJ adenocarcinomas and positive lymph node status, who did not receive neoadjuvant chemotherapy.
INTRODUCTION
Surgical resection is the primary treatment for adenocarcinoma at the gastro-esophageal junction (GEJ). However, long term survival after curative resection range between 18% and 50% and depends on stage and complete tumour resection with negative margins (R0) (1).
At least 50% will experience relapse of their cancer disease arising from unresected microscopic metastases present at the time of surgery (2, 3).
To prevent relapse and improve survival several prospective studies have been conducted, investigating both pre-operative and post-operative therapy strategies.
In the pivotal Intergroup-0116 Phase III trial by Macdonald et all, adjuvant chemoradiotherapy improved both disease-free and overall survival in curatively resected patients with stomach and gastroesophageal adenocarcinoma (4).
However, the majority of the patients in the Intergroup-0116 trial and later studies, where similar adjuvant regime was used, had gastric cancer and only a minor part had cancer at the GEJ.
In the present study we compared the survival of patients curatively resected for adenocarcinoma at the GEJ and postoperatively treated according to the Intergroup-0116 protocol, with the survival of patients, who underwent curative surgery alone.
MATERIALS AND METHODS
PATIENTS AND PREOPERATIVE EVALUATION
From 2003 to 2009, 211 consecutive patients were referred to our department with resectable, biopsy verified adenocarcinoma at the GEJ. According to the national guidelines, resectability was determined through thoracoabdominal computer tomografi, ultrasonography of the neck and esophageal endoscopic ultrasonography (EUS). All 211 patients were classified to performance status 0–2 without major comorbidity that would make them ineligible for surgery (Fig. 1).
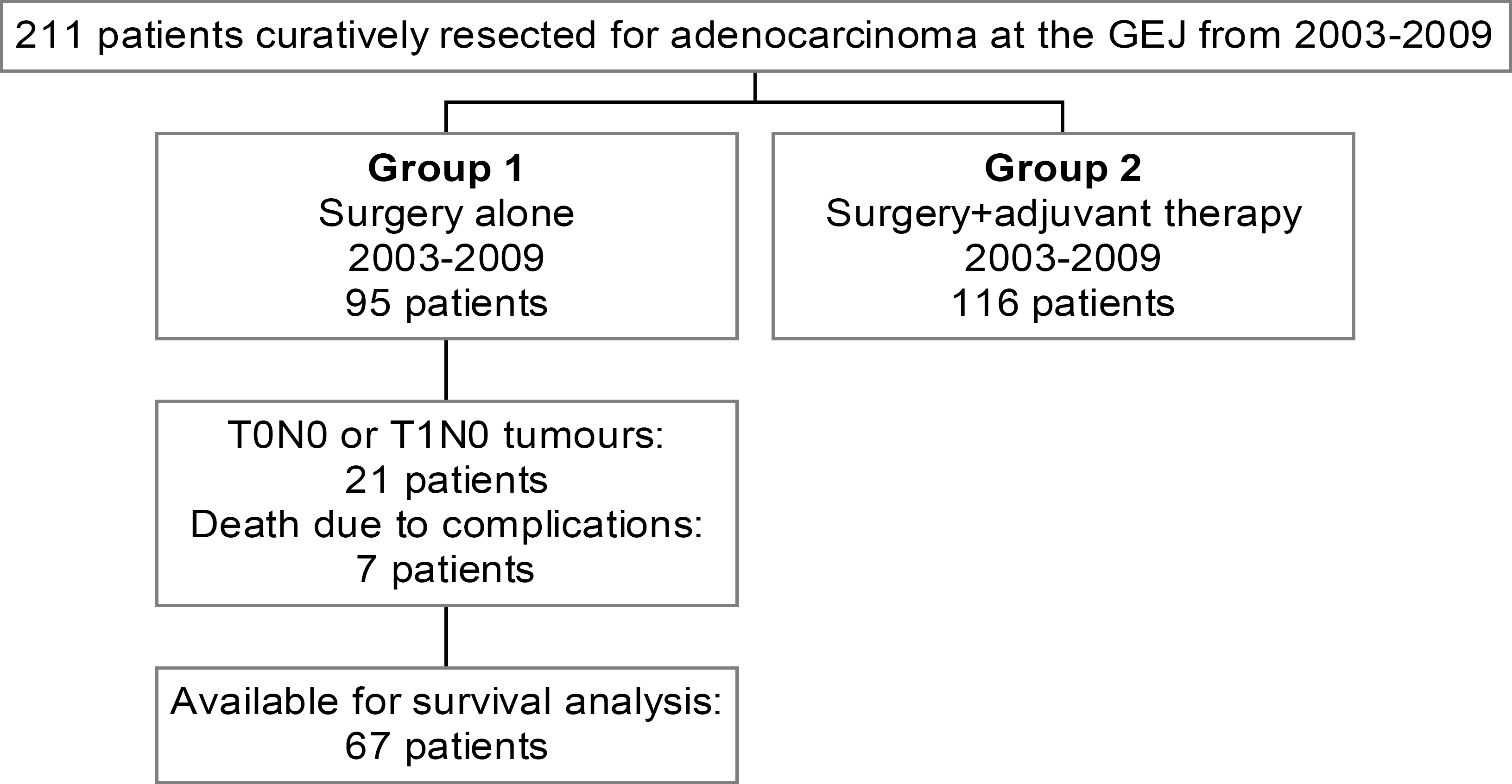
Study design of the 211 patients, curatively resected for adenocarcinoma at the GEJ from 2003–2009.
SURGERY
The operation was carried out as a modified Lewis Tanner procedure and was consistent throughout the whole period: A two-phase abdominal and right chest approach for enbloc subtotal esophagectomy followed by a double-stapled esophagogastric anastomosis. A D1 resection extended with dissection of the celiac nodes was performed. If the majority of tumour was in the stomach (Siewerts type lll), a gastrectomy was performed along with the esophagectomy (5) through an abdominal incision. The proximal jejune intestine was used as conduit and anastomosed side-to-end to the remaining esophagus. The distal anastomosis was done as a Roux-en-y reconstruction.
In both surgical procedures, the lines of resection were placed as far way from the tumour as possible and always at least 6 cm from tumour in the in-vivo specimen.
All operations were conducted by the same 3 surgeons in cooperation with a thoracic surgeon.
POSTOPERATIVE STAGING
The pathological examination of the resected specimen were performed by the same two pathologists. Tumour grade, local lymph node involvement, number of lymph nodes present in the specimen and resection margin status were registered. R0 resection was defined as macro- and microscopic tumour-free resection margins.
65 patients (31%) had between 15 and 25 nodes resected and 57 (27%) patients had 25 or more nodes resected.
The international TNM classification of gastro-esophageal cancer (6th edition) was used for tumour staging.
ADJUVANT THERAPY
In accordance with the MacDonald study, adjuvant chemoradiation was offered to all patients with T-stage higher than T1 with or without lymph node metastases.
The postoperative adjuvant treatment consisted of chemotherapy with fluorouracil plus leucovorin and loco-regional radiotherapy. Chemotherapy (fluorouracil, 425 mg per square meter per day and leucovorin 10 mg per square meter, for 5 days) was initiated on day 1 and was followed by radiotherapy beginning 28 days after the start of the initial cycle of chemotherapy. Concomitant chemotherapy with fluorouracil 400 mg per square meter plus leucovorin 10 mg per square meter was given on the first four days and the last three days of radiotherapy. One month after the completion of radiotherapy, two five-day cycles of fluorouracil were given one month apart.
All patients received daily treatment 5 days a week for 5 weeks using 1,8 Gy fractions, 45 Gy in total, administered using beams ranging in energy from 6–18 MV photons.
The Clinical target volume CTV included the primary tumour volume, operative bed and the regional lymph nodes. The tumour bed was defined by preoperative computed tomography (CT) imaging and in some instances, surgical clips, surgery note and pathological findings. Typically, 3-field or 4-field techniques were used.
POSTOPERATIVE FOLLOW-UP
To calculate disease-free survival, information about recurrence was collected from the Danish Cancer Register, a national center that receives information on all incidences of cancer or recurrence of cancer disease. The date of death was collected from the Central Death Register.
STATISTICS
Disease-free survival was defined as the time from the day of surgery untill death or to the date of registration of relapse. January 4, 2011 was the censoring date for survival.
Survival curves were estimated using the Kaplan-Meier method, and log rank test was used to evaluate the statistical significance of the differences. In order not to overestimate the benefit of adjuvant chemoradiotherapy, patients who died after experiencing severe complications after surgery were excluded from the survival analysis. In accordance with the Intergroup 0116 protocol, patients with superficial tumours (T0N0 or T1N0) were also excluded because patients of this category were not given adjuvant therapy (Fig. 1).
Differences between the surgery alone group and the surgery and adjuvant therapy group found during univariate analysis were entered into a logistic regression analysis to control for the potential confounding effects of these differences.
Categorical data were compared using chi-square test or Fischer's exact test. Continuous data are shown in mean ± SD and were compared using Mann-Whitney test. A two-sided P-value < 0.05 was accepted as statistically significant. The SPSS statistical package (version 11.0; SPSS inc., Chicago, IL) was used for all analyses.
ETHICS
The Danish Data Protection Agency has approved the processing of data (2001-41-1452).
RESULTS
Characteristics of the 211 patients who underwent curative resection and those who were not candidates to postoperative chemoradiation are shown in Table 1 and Fig. 1. Seven patients died due to complications in relation to surgery (in-hospital mortality: 3,3%).
Characteristics of the 211 patients, curatively resected for adenocarcinoma at the GEJ from 2003–2009.
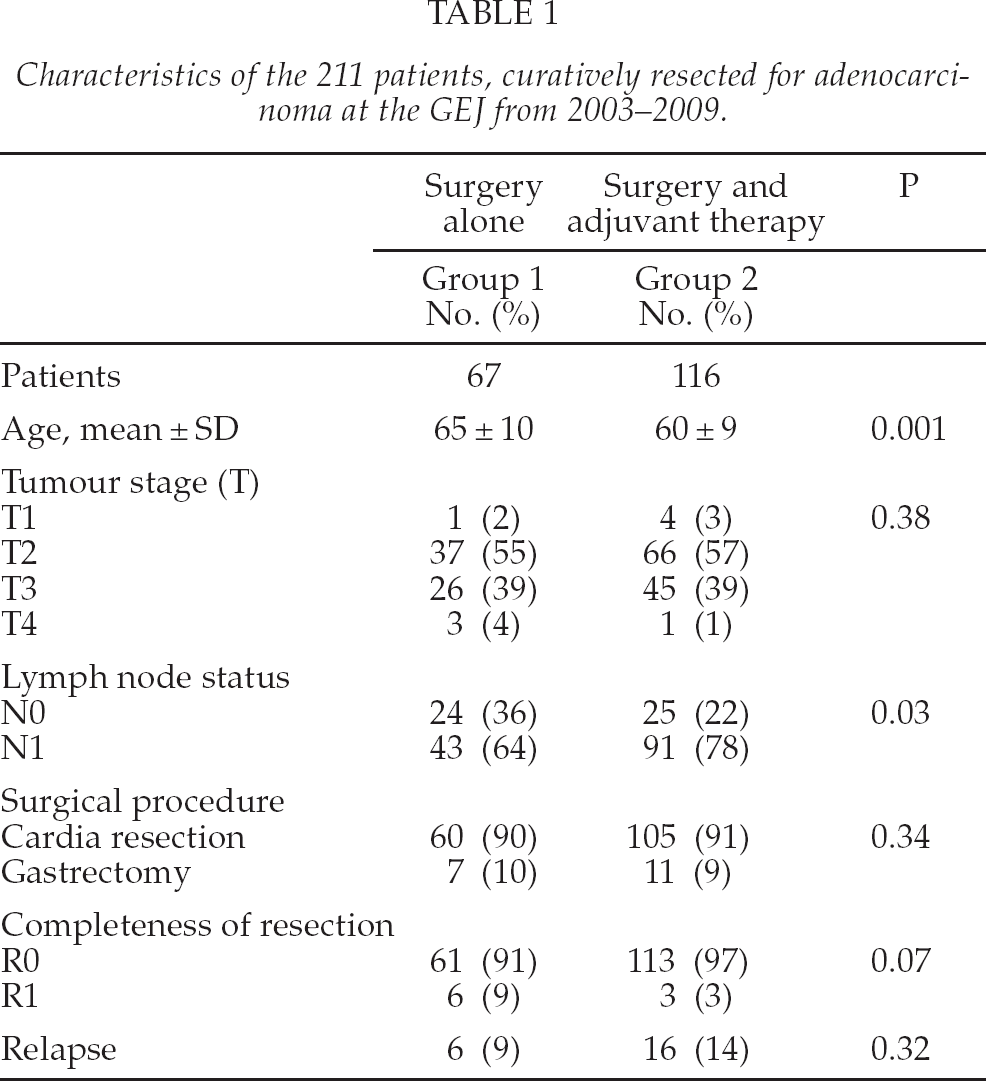
Patients that received adjuvant therapy were significantly younger than patients who underwent surgery alone.
During the period from 2003 to 2009, 55% of the patients received adjuvant chemoradiotherapy. In Table 2 the reasons for not receiving adjuvant therapy are listed.
Reasons for refraining from chemoradiotherapy.
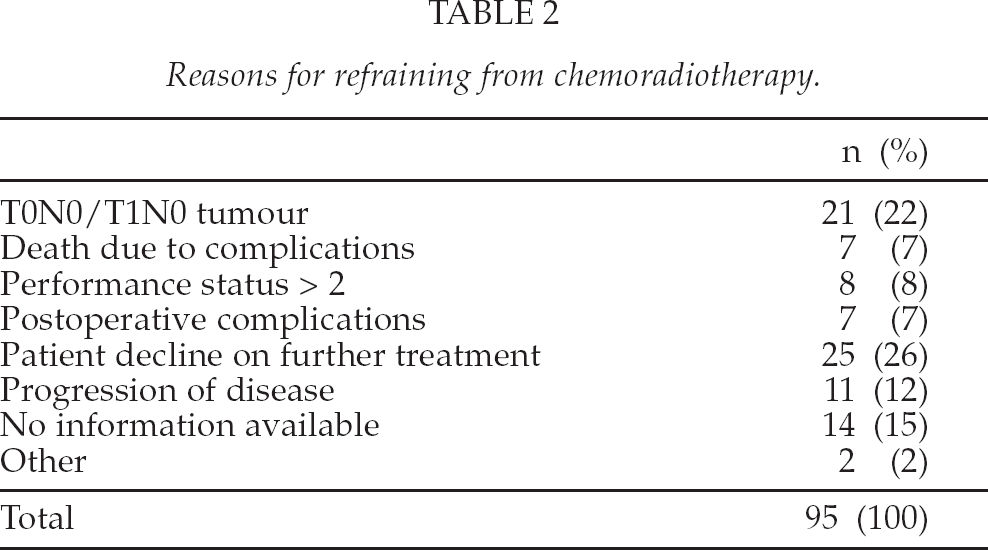
Fig. 2 shows the overall disease-free survival in patients who underwent surgery alone (n = 67) or underwent surgery and received adjuvant therapy (n = 116). No significant difference was seen in the overall survival (P = 0.36).
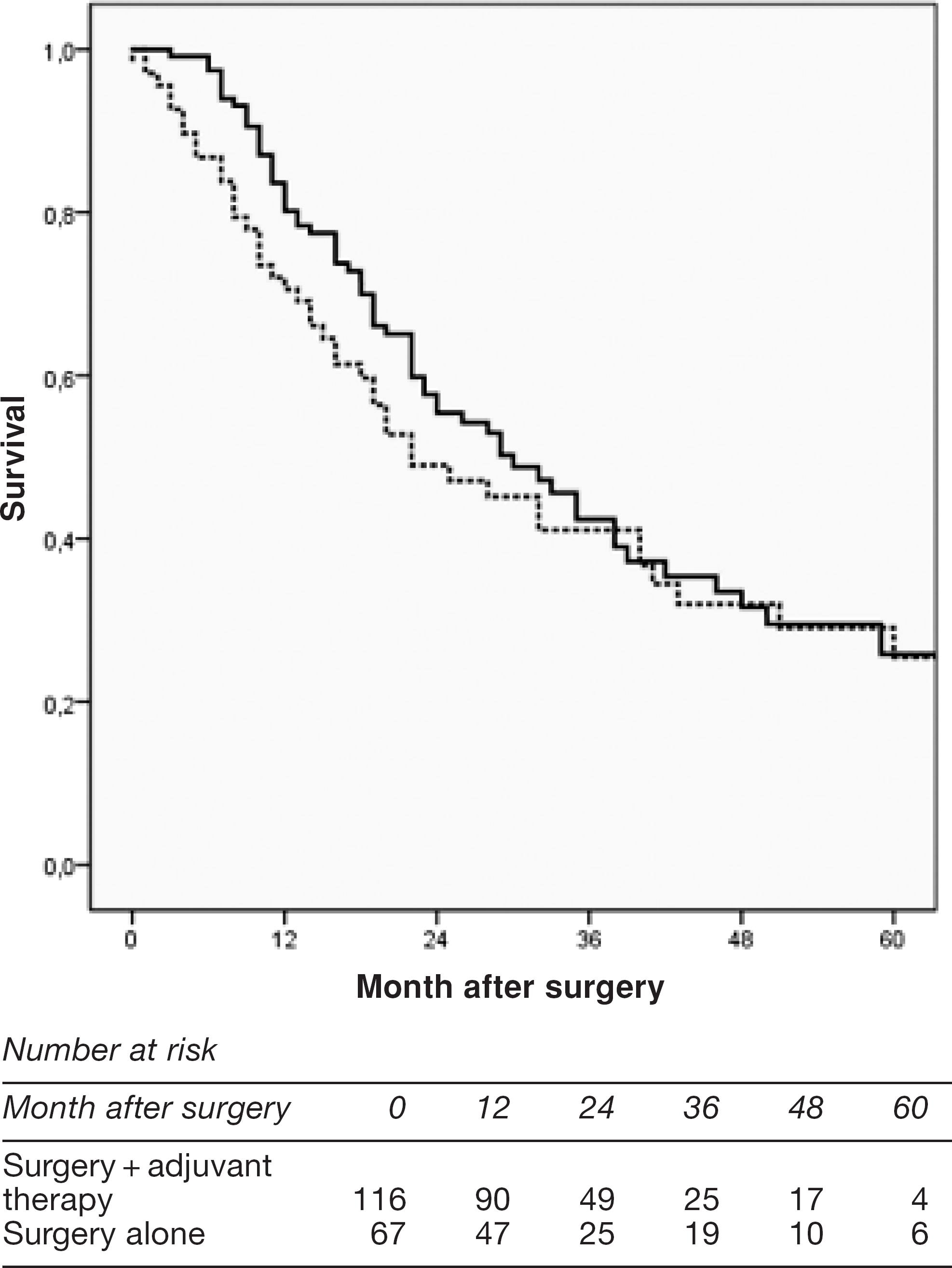
Disease-free survival after adjuvant chemoradiotherapy (n = 116) (solid line) or surgery alone (n = 67) (dashed line) in curatively resected patients with adenocarcinoma at the GEJ (P = 0.36).; Patients with T0N0/T1N0 tumour and deaths due to complications were excluded.
Fig. 3 shows the disease-free survival after adjuvant chemoradiotherapy (n = 91) or surgery alone (n = 43) in patients with positive node status in the resected specimen.
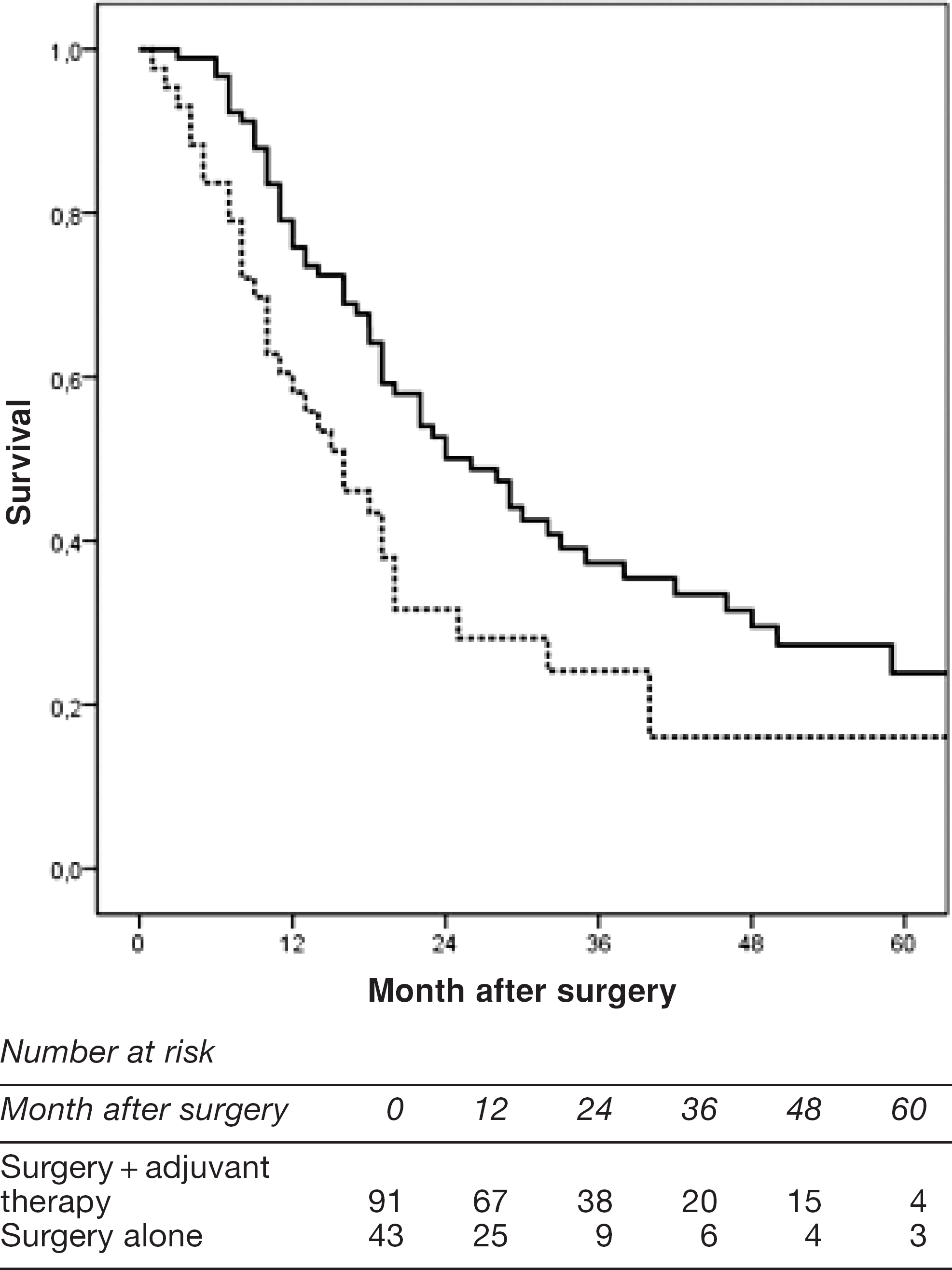
Disease-free survival after adjuvant chemoradiotherapy (n = 91) (solid line) or surgery alone (n = 43) (dashed line) in patients with positive node status in the resected specimen (P = 0.014).; Patients with T0N0/T1N0 tumour and deaths due to complications were excluded.
The 3-year survival rate in the surgery alone group was 24% compared to 37% in the surgery and adjuvant therapy group. Median time of survival was 16 month (CI:10–22) in the surgery alone group versus 26 month (CI:19–33) in the adjuvant therapy group (P = 0.014).
In patients with N0-disease, no significant difference in survival was found between those who underwent surgery alone versus those who received adjuvant therapy (P = 0.28, data not shown).
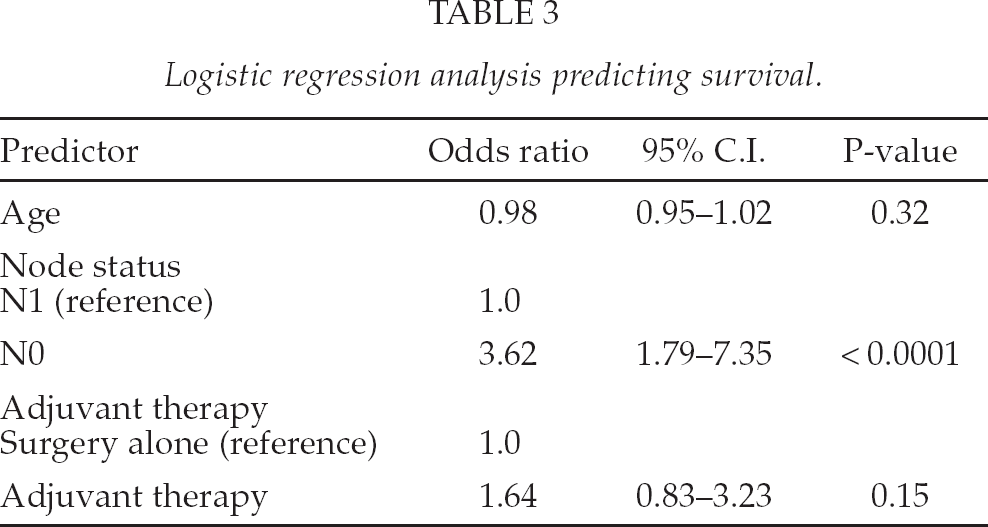
Table 3 shows the logistic regression predicting probability of survival (odds ratio) for the variables age and node status, where significant differences were found between the two groups by univariate analysis. Only node status had significantly partial effect on survival.
Logistic regression analysis predicting survival.
Patients receiving adjuvant therapy, clinically important acute toxicities were mainly gastrointestinal, including nausea, vomiting and diarrhea. A previous report from our institution regarding adjuvant therapy according to the Intergroup-0116 regimen, described three early deaths, where cardiotoxicity to 5-FU could not be excluded as the cause of death and 33% experienced therapy-related toxicities requiring dose-reduction (6).
DISCUSSION
Adenocarcinomas of the GEJ are often lumped in therapeutic trials and analyzed with either esophageal cancer or gastric cancer. To our knowledge this is the first study to report survival data after curative surgery and adjuvant chemoradiotherapy solely at the GEJ, and it reinforces the role of adjuvant chemoradiotherapy in this setting.
Adjuvant chemoradiotherapy has been evaluated in primarily gastric cancer in the pivotal Intergroup-0116 study (4), where only 20% of the tumours were located at the GEJ. The median overall survival was prolonged from 27 months to 36 months, favouring the combined treatment. The three-year survival rates were 50 percent in the chemoradiotherapy group and 41 percent in the surgery alone group.
We found that compared to patients who underwent surgery alone, patients with positive node status in the resected specimen the 3-year disease-free survival was 13% higher in the adjuvant therapy group and the median survival prolonged by 10 month. However, after controlling for the confounding effect of age and node status, the survival benefit of postoperative chemoradiation was no longer significant probably because of the relatively low number of patients.
The 3-year disease-free overall survival in our material was lower compared with the Intergroup-0116 study since survival after curative resection for gastric cancer is generally higher compared with survival after resection for GEJ cancer.
The survival benefit of adjuvant therapy observed might be explained by microscopic metastases present at the time of surgical resection, receptive for chemoradiation.
Neoadjuvant chemoradiotherapy has mainly been evaluated in a number of smaller studies in esophageal cancer, several of those showing a trend towards improved survival. In a metanalysis by Gebski et al (7), a significant survival benefit was found for neoadjuvant chemoradiotherapy in adenocarcinomas of the esophagus. The hazard ratio for all-cause mortality with neoadjuvant chemoradiotherapy versus surgery alone was 0.75 (0.59–0.95; P = 0.02) in the group of adenocarcinomas. Three of 4 studies with adenocarcinomas in this metanalysis included patients with GEJ tumours (8 –10).
Neoadjuvant chemotherapy has proved superiority to surgery alone in esophagogastric cancer (11) and perioperative chemotherapy has now become a standard treatment after the publication of the pivotal MAGIC-trial with a 13% improvement in overall survival at 5 years (23% vs. 36%) favouring perioperative chemotherapy. In a large metanalysis a significant benefit with neoadjuvant chemotherapy for patients with adenocarcinoma in the esophagus and GEJ was found (hazard ratio for all-cause mortality 0.78 (0.64–0.95); P = 0.014) (7).
Stahl et al (12) compares neoadjuvant chemotherapy with neoadjuvant chemoradiotherapy in a phaseIII trial with 126 patients showing an improved 3-year survival in favour of neoadjuvant chemoradiotherapy (27.7% vs. 47.4%), not reaching statistical significance (P = 0.07), the study was closed early due to low accrual.
No randomized trial has tested neoadjuvant (perioperative) chemotherapy against adjuvant chemoradiotherapy. The future role for adjuvant chemoradiotherapy is explored in the ongoing CRITICS trial in gastric and GEJ cancer. It aims at answering the question, whether adjuvant chemoradiotherapy (after neoadjuvant chemotherapy) or perioperative chemotherapy improves survival and/or locoregional control after radical surgery (CRITICS-trial) (13).
At present we therefore do not know the best way to combine the treatment modalities in GEJ cancers.
The significant survival benefit among patients with lymph node involvement and the 3.6-times higher survival seen in the N0 — group in our study, emphasizes the importance of thorough lymph node dissection during surgery and during pathological examination in order to improve precision of staging and decide whether adjuvant therapy is relevant. Long-term follow-up of the Dutch D1D2 trial has recently been reported, showing better cancer-related survival after D2 resection (14). Increased focus on the importance of lymph node status and proper staging has resulted in a changed procedure at our institution: all lymph node stations from the resected specimen are forwarded separately to the pathologist, a procedure reported to increase the number of dissected lymph nodes (15). No international standardization exists neither in terminology nor methodology for the pathological examination of the lymph nodes (16).
The present retrospective study has of course its limitations. Patients were not allocated to this therapy by randomisation. Therefore, a considerable selection bias is present in this material. It might be argued that only the “survivors” received the treatment. Even without adjuvant therapy, this subgroup might have had a superior survival. Furthermore, the surgery alone group included 25 patients who declined adjuvant therapy and 11 who already had progression of disease at the time for the adjuvant therapy.
On the other hand, in the surgery and adjuvant therapy group, 3 early deaths were reported where cardiotoxicity to 5-FU might have been the cause of death and one third of the patients receiving adjuvant therapy required dose-reduction due to sideeffects. Additionally, in this group, significantly more patients had positive nodes in the resected specimen.
Finally, information regarding relapse was collected from the Danish National Cancer Register and not by regular postoperative follow up. This definitely underestimates the number of relapses. D'Angelica el al have shown that in a cohort of patients who were curatively resected for gastric cancer 42% had relapse of disease. Among these patients, 54% had locoregional recurrence (17).
CONCLUSION
Our results indicate that adjuvant chemoradiotherapy according to the Intergroup-0116 protocol might still be a reasonable option after curative resection in patients with GEJ adenocarcinomas and positive lymph node status, who did not receive neoadjuvant chemotherapy.
Footnotes
APPENDIX
This study was presented at the European Society of Thorasic Surgery (ESTS) annual meeting 2010 in Valladolid, Spain and at the Digestive Disease Week (DDW) 2010 in New Orleans, LA, U.S.A.